Maximising Access to Essential Medicines for Church Health
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
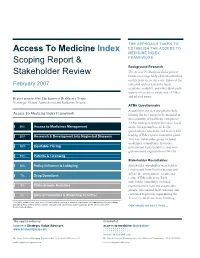
Access to Medicine Index Scoping Report & Stakeholder Review
THE APPROACH TAKEN TO Access To Medicine Index ESTABLISH THE ACCESS TO MEDICINE INDEX Scoping Report & FRAMEWORK Background Research The Access To Medicine Index project Stakeholder Review builds on a large body of work published on this issue in recent years. Innovest has February 2007 collected and reviewed the latest academic, industry, and other third-party reports on access to medicines (ATMs) and related issues. Report prepared by The Innovest Healthcare Team: Veronique Menou, Adam Savitz and Katharine Preston. ATMs Questionnaire A questionnaire was designed to help Access To Medicine Index Framework identify the key issues to be included in an evaluation of healthcare companies’ ATMs strategies and performance based 20% Access to Medicines Management on the background research. The questionnaire was delivered to over 200 20% Research & Development into Neglected Diseases leading ATMs experts around the globe. This key stakeholder group included academics, consultants, investors, 18% Equitable Pricing government representatives, and non- governmental organizations (NGOs). 15% Patents & Licensing Stakeholder Roundtables 10% Policy Influence & Lobbying Stakeholder roundtables were held in London and New York to discuss and debate the questionnaire results and 7% Drug Donations refine ATMs indicators. Each stakeholder roundtable included 5% Philanthropic Activities representatives from the stakeholder groups, who shared their expertise and 5% Ethical Promotion & Marketing Activities continued to provide input during the Access To Medicine Index building This table includes the eight most relevant criteria, ranked in order of importance, as indicated by the percentage weighting. This criteria will be used to evaluate each pharmaceutical company’s performance during the CONTINUED ON NEXT PAGE… benchmarking phase. -

In South Africa: Access to Medicines in the Neoliberal Era an Insight Into the Public Market of Antiretroviral Treatments in South Africa
Angles New Perspectives on the Anglophone World 8 | 2019 Neoliberalism in the Anglophone World How To “Talk Left and Walk Right” in South Africa: Access to Medicines in the Neoliberal Era An insight into the public market of antiretroviral treatments in South Africa Charlotte Pelletan Electronic version URL: http://journals.openedition.org/angles/613 DOI: 10.4000/angles.613 ISSN: 2274-2042 Publisher Société des Anglicistes de l'Enseignement Supérieur Electronic reference Charlotte Pelletan, « How To “Talk Left and Walk Right” in South Africa: Access to Medicines in the Neoliberal Era », Angles [Online], 8 | 2019, Online since 01 April 2019, connection on 28 July 2020. URL : http://journals.openedition.org/angles/613 ; DOI : https://doi.org/10.4000/angles.613 This text was automatically generated on 28 July 2020. Angles. New Perspectives on the Anglophone World is licensed under a Creative Commons Attribution- NonCommercial-ShareAlike 4.0 International License. How To “Talk Left and Walk Right” in South Africa: Access to Medicines in the... 1 How To “Talk Left and Walk Right” in South Africa: Access to Medicines in the Neoliberal Era An insight into the public market of antiretroviral treatments in South Africa Charlotte Pelletan Introduction “I am not using strong words; I am using appropriate words. This is genocide”. Health Minister Aaron Motsoaledi (De Wet 2014) When the Minister of Health talks left… 1 In 1997, while the AIDS epidemic was spreading, the South African government explored changes to its regulation of patents in the Medicines Act and its National Drug Policy. It triggered a world-famous law case pitting the South African state against a coalition of pharmaceutical companies: the Medicines Act case, which concluded in 2001, also known as the Pretoria trial. -

IFMSA Policy Document Access to Medicines
IFMSA Policy Document Access to Medicines Proposed by Team of Officials Adopted by IFMSA General Assembly March Meeting 2019, in Portorož, Slovenia. Policy Statement Introduction: Access to affordable medicines and vaccines is an essential part of achieving Universal Health Coverage (UHC) and resilient health systems, as mentioned in Sustainable Development Goal (SDG) 3, Target 3.8. However, 2 billion people worldwide currently do not have access to essential medicines. IFMSA position: The International Federation of Medical Students' Associations (IFMSA), strongly believes that access to affordable, effective, and safe technologies is a human right. We believe that the current research and development (R&D) system lacks transparency and is driven by commercial interests rather than public health needs, which is in turn reducing the availability of affordable medicines. Publicly funded research, with its publicly-oriented incentives, makes an essential contribution to the development of medicines which should not be appropriated for commercial profit. Global patent monopolies for the protection of intellectual property (IP), as well as Free Trade Agreements (FTAs), such as Trade- Related Aspects of Intellectual Property Rights (TRIPS), are one of the most important barriers to generic medicine production. Additionally, TRIPS plus provisions, included in smaller FTAs, grant data exclusivity which stifles market approval for lower-cost alternatives. We support the use of TRIPS flexibilities as an internationally accepted tool to mitigate -

Missing Medicines in Malawi: Campaigning Against Stock-Outs of Essential Drugs Oxfam Programme Insights
Missing Medicines in Malawi Campaigning against ‘stock-outs’ of essential drugs A community march to protest about the lack of basic medicines at the local clinic. The march was followed by an event to discuss health issues with partner organizations and local leaders. Photo: Word Alive Commission for Relief and Development (WACRAD), Malawi. Malawi is one of the poorest countries in the world. The government has introduced some measures to improve the health of its people, but a number of major problems remain. One of these is the lack of essential medicines in government health clinics – known as ‘stock-outs’. These medicines should be free to poor people, but most find that they have to pay. This paper looks at an innovative campaign which aimed to tackle this problem by enhancing the capacity of local communities and civil society organizations to demand the right to access these medicines. The campaign also lobbied for a commitment to ensure increased availability and accessibility in rural areas and carried out budget and resource tracking. This paper looks at the difficulties the Programme Insights Programme campaign faced and outlines the factors that contributed to its success. Introduction Malawi is one of the poorest countries in the world, with more than half its population living on less than a dollar a day. Local-level campaigning on access to medicines took place in six districts in the southern part of the country. ‘Access to essential medicines is a human right and a 1 cornerstone of an effective primary health care system.’ Malawi is one of the poorest countries in the world. -

Access to Essential Medicines As a Component of the Right to Health Stephen P
Health: A Human Rights Perspective 82 ACCESS TO ESSENTIAL MEDICINES AS A COMPONENT OF THE RIGHT TO HEALTH Stephen P. Marks Introduction In Human Rights Obligations of Non-State Actors, Andrew Clapham wrote, “Perhaps the most obvious threat to human rights has come from the in- ability of people to achieve access to expensive medicine, particularly in the context of HIV and AIDS.”1 He was referring to threats to human rights from intellectual property agreements under the World Trade Organiza- tion, which are often seen as obeying a different – and many would say ut- terly incompatible – logic than human rights. The right to health, in the interpretation of the Committee on Economic Social and Cultural Rights, means that “States Parties … have a duty to prevent unreasonably high costs for access to essential medicines.”2 This chapter will explain the significance and place of the human right to essential medicines as a derivative right within the broader right to the highest attainable standard of physical and mental health. As a component of the right to health, the right to essential medicines depends not only on the production, distribution, and pricing of medicines, but also on the in- centives for research and development of drugs needed to treat diseases in developing countries, functioning health systems so that drugs are part of a rational system of quality treatment and care, as well as on infrastructure, Access to Essential Medicines as a Component of the Right to Health 83 so that they can be delivered to all areas where they are needed. Consider- ing that these broader issues are examined in other chapters, this chap- ter will focus more on the impediment to the realization of the right to essential medicines caused by the protection of intellectual property. -

Roadmap for Access 2019 – 2023 ‘Comprehensive Support for Access to Medicines and Vaccines’ Statement by Médecins Sans Frontières International
Roadmap for access 2019 – 2023 ‘Comprehensive support for access to medicines and vaccines’ Statement by Médecins Sans Frontières International. Speaker: Katy Athersuch Médecins Sans Frontières welcomes the decision of the Seventy-first World Health Assembly to elaborate a road map outlining the programming of WHO’s work on access to medicines and vaccines. As an international medical humanitarian organisation, our teams see the devastating impact that widespread lack of access to essential health technologies has on people’s lives. Inadequate access to affordable health technologies and the failures of the global research and development (R&D) system are crises of international concern that touch on our operations every day. With this experience in mind and having reviewed the zero draft, we would like to highlight the following points: 1. In line with commitments in the Global Strategy and Plan Of Action on Public Health and Intellectual Property (GSPOA) and previous resolutions, we urge WHO to include a deliverable on the provision of technical assistance and capacity building to countries to implement health needs-driven R&D that is evidence based and guided by the core principles of affordability, effectiveness, efficiency, equity and the principle of delinkage. 2. We urge WHO to fix the Roadmap’s definition of fair pricing. It is not about finding an algorithm that will mechanically give a fair price for each medicine. It is about the conditions of the price negotiations between public health and commercial interests in order to achieve a balance. It requires management of exclusive rights to avoid undue or abusive monopolies, and far more transparency and disclosure on public and private investments in a product’s development from basic research through to the delivery to people. -
Access to Medicine Index 2018 METHODOLOGY 2017 Access to Medicine Index 2018 Methodology Report 2017
Access to Medicine Foundation Access to Medicine Index 2018 METHODOLOGY 2017 Access to Medicine Index 2018 Methodology Report 2017 ACCESS TO MEDICINE FOUNDATION September 2017 1 Methodology for the 2018 Access to Medicine Index ACKNOWLEDGEMENTS The Access to Medicine Foundation would like to thank the following people and organisations for their contributions to this report. FUNDERS Bill & Melinda Gates Foundation The UK government The Netherlands Ministry of Foreign Affairs EXPERT REVIEW COMMITTEE Hans Hogerzeil (Chair) Sanne Frost-Helt Fumie Griego Suzanne Hill Frasia Karua Dennis Ross-Degnan Dilip Shah Yo Takatsuki Joshua Wamboga Prashant Yadav TECHNICAL SUBCOMMITTEES RESEARCH TEAM EDITORIAL TEAM Esteban Burrone Danny Edwards Anna Massey Nick Chapman Beth Boyer Deirdre Cogan Jennifer Dent Clarke Cole Michele Forzley Luca Genovese Warren Kaplan Catherine Gray Jillian Kohler Nestor Papanikolaou Niranjan Konduri Tara Prasad Stine Trolle ADDITIONAL CONTRIBUTORS We would like to thank the many other experts who contributed their views to the development of this methodology (see page 56). ACCESS TO MEDICINE FOUNDATION The Access to Medicine Foundation is an independent non-profit org- anisation based in the Netherlands. It aims to advance access to medi- cine in low- and middle-income countries by stimulating and guiding the pharmaceutical industry to play a greater role in improving access. Naritaweg 227-A 1043 CB, Amsterdam The Netherlands For questions about this report, please contact Danny Edwards, Research Programme Manager [email protected] +31 (0) 20 215 35 35 www.accesstomedicineindex.org 2 Access to Medicine Foundation A good practice framework There is no simple blueprint for making medicine accessible During ten years of research, we have identified real progress to all who need them. -

ACCESS CHALLENGES for HIV TREATMENT Among People Living with HIV and Key Populations in Middle-Income Countries
ACCESS CHALLENGES FOR HIV TREATMENT Among People Living with HIV and Key Populations in Middle-Income Countries POLICY BRIEF // OCTOBER 2013 Acronyms ACTA Anti-Counterfeiting Trade Agreement AIDS Acquired Immunodeficiency Syndrome ART Antiretroviral Therapy ARV Antiretroviral EPA Economic Partnership Agreement EU European Union FTA Free Trade Agreement HAART Highly Active Antiretroviral Therapy HIV Human Immunodeficiency Virus ICESCR International Convention on Economic, Social and Cultural Rights IP Intellectual Property MDG Millennium Development Goal MICs Middle Income Countries MSM Men Who Have Sex With Men NCDs Non-Communicable Diseases PEPFAR President’s Emergency Plan for AIDS Relief PLHIV People Living with HIV PMTCT Preventing Mother-to-Child Transmission PWID People Who Inject Drugs SW Sex Workers TG Trans-gender Persons TRIPS Trade-Related Aspects of Intellectual Property Rights UNAIDS Joint United Nations Program on HIV/AIDS WHO World Health Organization WTO World Trade Organization 1 Access Challenges for HIV Treatment // Background ACCESS CHALLENGES FOR HIV TREATMENT Among People Living with HIV and Key Populations in Middle-Income Countries BACKGROUND More than two billion people in middle-income countries (MICs) lack access to essential medicines. Medicines are expensive, and consume 25 to 65 percent of the total private and public spending on health, and 60 to 90 percent of household expenditure in MICs.1 In the public sector, there is poor availability of medicines and patients are forced to purchase medicines from the private market. The Global Burden of Diseases 2010 study shows that MICs rather than experiencing a classic ‘epidemiological transition’ in which infectious diseases dissipate and non-communicable diseases (NCD) emerge, are facing a ‘dual burden’ in which infectious diseases are still prevalent, especially HIV, viral hepatitis and tuberculosis, while NCD rates are rising.2 Access to affordable medicines3 is therefore of central importance in ensuring universal access to health care in these countries. -

People and Communities Factsheet
The Novartis Malaria Initiative Access – improving affordability and availability of medicines Over the past decade, the Novartis Malaria – We have completed one of the largest and Initiative has pioneered the pharmaceutical fastest scale-ups in the industry: from four response to the fight against malaria by million treatments in 2004 to over 82 million spearheading what has become one of the treatments delivered in 2010; and from industry’s largest access-to-medicine programs 12 countries served to more than 60 today. In today. the same timeframe, thanks to economies of scale in sourcing and manufacturing, Pioneering the not-for-profit supply significant cost reductions could be achieved of treatments that allowed to reduce the price for public- Through a partnership with the World Health sector buyers by more than half. Organization (WHO) in 2001, Novartis was the – In order to ensure patient access in countries first company in the pharmaceutical industry to where the need is greatest and resources are commit to the not-for-profit supply of antimalarial most limited, Novartis has adopted a treatments to the public sector of endemic differential pricing strategy.* We are also countries. exploring differential pricing structures – Since 2001, we have provided more than 400 through novel channels to improve access. It million treatments of our artemisinin-based is estimated that up to half of malaria combination therapies (ACTs), Coartem® for patients in Africa do not have access to public adults and Coartem® Dispersible for children, health services and buy antimalarial without profit to malaria-endemic countries, treatments at local market stalls and drug saving an estimated 1 million lives.1 shops where they often purchase sub- – Treatments are brought to malaria-endemic standard or counterfeit medicines because countries through grants from the Global they are cheaper. -
Access to Medicines in the Context of the Right to Health
©UN Photo/Albert González Farran Access to Medicines in the context of the Right to Health Access to Medicines in the context of the Right to Health Summary The present report contains a summary of discussions and recommendations of the 2015 Social Forum. In accordance with Human Rights Council resolution 26/28, the Forum was held in Geneva from 18 to 20 February 2015, and focused on access to medicines in the context of the right of everyone to the enjoyment of the highest attainable standard of physical and mental health, including best practices in that regard. © point-of-views.ch © point-of-views.ch Contents paragraphs page I. Introduction 1–3 4 II. Opening of the Social Forum 4–6 5 III. Summary of proceedings 7–58 7 A. Keynote speakers and general statements 7–10 7 B. Overview of access to medicines in the context of the right to health 11–15 9 C. Improving health delivery systems in challenging contexts 16–20 10 D. Access to medicines for women and children 21–25 12 E. Intellectual property rights and access to medicines 26–30 13 F. Lessons learned and emerging challenges in the global response to AIDS 31–35 15 G. Patient-centred approaches to access to medicines 36–41 16 H. Breakout discussion groups and plenary discussion 42–43 18 I. Innovative approaches to promoting access to medicines 44–49 19 J. Good practices in promoting access to medicines (round table) 50–58 20 IV. Conclusions and recommendations 59–74 26 A. Conclusions 60–66 26 B. -

Takeda's Position on Access to Medicines
Takeda’s Position on Access to Medicines Key messages Takeda believes access to healthcare, medicines and vaccines is a priority for people globally. As part of our Access to Medicines strategy, we are committed to addressing the unmet needs of patients wherever they may be, and sustainably strengthening local health systems at every stage of the patient journey. We complement this approach with a commitment towards developing an end-to-end access approach to make our highly-innovative medicines available as soon as practically possible. Background The past decade has seen major public health gains and scientific breakthroughs, yet more than two billion people today cannot access the healthcare they need when facing serious, complex and rare diseases. The communities most severely impacted are resource-poor countries with a higher need to strengthen their healthcare systems. This is the frontier in access to medicines that cannot be addressed alone and needs collective action with deep collaboration and lasting commitments between partners across the public and private sector. Takeda’s position Access to Medicines is deeply embedded within Takeda’s vision to serve patients wherever they are, focused on long-term commitments and supported across our organization. We have created a practical framework to increase sustainable access to our medicines through our innovative affordability programs and initiatives that build sustainable capacity across the patient journey, while collaborating with policy makers and experts from NGOs, patient organizations, and governments. Across our programs we have controls in place to mitigate the risk of non-compliance in our operations, including internal controls, risk-based country audits, and formal processes applying to third parties. -

Access to Medicines in Southern Africa
47 CASE STUDY 04 Access to Medicines in Southern Africa Problem description The production and sale of medicines is a contested yet lucrative global industry, considering that the use of certain drugs is not optional. Medicine is not subject to normal economic perceptions of price and demand elasticity. There are specific dominant players in the market, including large pharmaceutical corporations, distributors and pharmacies, which often collude with one another in environments where government regulation is weak. Governments in the Southern African Development Community (SADC) region aim to control prices and standards through local medical regulatory authorities (MRAs, also known as drug regulatory agencies or DRAs).1 1 MRAs establish standards of manufacturing and evaluation of safety and efficacy for medicines. Regulatory standards are not as advanced and also subject to WHO pre- qualifications, as a prerequisite for WHO accreditation. These qualifications are not prescriptive to local conditions and can be requested on demand. 48 CASE STUDY 04 / Access to medicines in Southern Africa Apart from their regulatory function, MRAs are also responsible for some sourcing of medicines. The private sector and donor agencies are also involved: the Global Fund and the President’s Emergency Plan for AIDS Relief (PEPFAR) both do extensive sourcing of medicines as organisations or through procurement agencies in individual countries. Africa’s three killer diseases are HIV/AIDS, tuberculosis (TB) and malaria. The World Health Organization (WHO) says that more than two-thirds of new HIV infections occur in sub-Saharan Africa. In 2012, there were an estimated 207 million cases. Approximately 8.6 million new TB cases were reported in 2012 (in 1.1 million cases, those infected were also HIV-positive) and an estimated 1.3 million deaths were reported (including those of 320 000 people with HIV).