Comparison of Diagnostic Accuracy of Physical Examination and MRI in the Most Common Knee Injuries
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Journal of Clinical Trails Market Analysis Advances in Clinical Research and Clinical Trials 2020
Journal of Clinical Trails Market Analysis Advances in Clinical Research and Clinical Trials 2020 Raymond Chong The research report on Global Clinical Trials Market 2019 Other prominent players in the value chain include Mednet keenly analyzes significant features of the industry. The Solutions, Arisglobal, eClinForce Inc., DZS Software Solutions, DSG, analysis servers market size, latest trends, drivers, threats, Inc., Guger Technologies Inc., ICON, Plc., ChemWare Inc., and opportunities, as well as key market segments. It is based on iWeb Technologies Limited. past data and present market needs. Also, involve distinct business approaches accepted by the decision makers. Those intensify growth and make a remarkable stand in the industry. The Clinical Trials market will grow with a significant CAGR between 2019 to 2028. The report segregates the complete market on the basis of key players, geographical areas, and segments. Increasing demand for new medical equipments and medicines among end users, coupled with growing investment for research and development activities for development of effective medicines are major factors driving growth of the global clinical trials market. In addition, increasing number of individuals suffering from chronic diseases as well as changing The clinical trials market is projected to arrive at USD 1.76 conditions and nature of certain types of chronic diseases is billion by 2025, from USD 1.04 billion in 2017 growing at a another factor anticipated to support growth of the global CAGR of 6.7 percent from 2018 to 2025. An upcoming clinical trials market to significant extent. market report contains data for historic year 2016, and the base year of calculation is 2017. -

Physical Esxam
Pearls in the Musculoskeletal Exam Frank Caruso MPS, PA-C, EMT-P Skin, Bones, Hearts & Private Parts 2019 Examination Key Points • Area that needs to be examined, gown your patients - well exposed • Understand normal functional anatomy • Observe normal activity • Palpation • Range of Motion • Strength/neuro-vascular assessment • Special Tests General Exam Musculoskeletal Overview Physical Exam Preview Watch Your Patients Walk!! Inspection • Posture – Erectness – Symmetry – Alignment • Skin and subcutaneous tissues – Swelling – Redness – Masses Inspection • Extremities – Size – Deformities – Enlargement – Alignment – Contour – Symmetry Inspection • Muscles – Bilateral symmetry – Hypertrophy – Atrophy – Fasciculations – Spasms Palpation • Palpate bones, joints, and surrounding muscles for the following: – Heat – Tenderness – Swelling – Fluctuation – Crepitus – Resistance to pressure – Muscle tone Muscles • Size and strength affected by the following: – Genetics – Exercise – Nutrition • Muscles move joints through range of motion (ROM). Muscle Strength • Compare bilateral muscles – Strength – Symmetry – Equality – Resistance End Feel Think About It!! • The sensation the examiner feels in the joint as it reaches the end of the range of motion of each passive movement • Bone to bone: This is hard, unyielding – normal would be elbow extension. • Soft–tissue approximation: yielding compression that stops further movement – elbow and knee flexion. End Feel • Tissue stretch: hard – springy type of movement with a slight give – toward the end of range of motion – most common type of normal end feel : knee extension and metacarpophalangeal joint extension. Abnormal End Feel • Muscle spasm: invoked by movement with a sudden dramatic arrest of movement often accompanied by pain - sudden hard – “vibrant twang” • Capsular: Similar to tissue stretch but it does not occur where one would expect – range of motion usually reduced. -

Examination of the Knee
Examination of the Knee The Examination For every joint of the lower extremity always begin with the patient in standing IN STANDING INSPECTION 1. Cutaneous Structures: Look for Erythema, scarring, bruising, and swelling in the following areas: a. Peripatellar grooves b. Suprapatellar bursa c. Prepatellar bursa d. Infrapatellar tendon e. Anserine bursa f. Popliteal fossa 2. Muscle & Soft Tissue: a. Quadriceps atrophy b. Hamstring atrophy c. Calf atrophy 3. Bones & Alignment: a. Patella position (Alta, Baha, Winking, Frog eyed), b. Varus or Valgus alignment c. Flexion contracture or Genu recurvatum RANGE OF MOTION - ACTIVE Standing is the best opportunity to assess active range of motion of the knee. 1. Ask the patient to squat into a deep knee bend. Both knees should bend symmetrically. 2. Ask the patient to then stand and extend the knee fully – lock the knee. The knee should straighten to 0 degrees of extension. Some people have increased extension referred to as genu recurvatum. GAIT 1. Look for a short stance phase on the affected limb and an awkward gait if a concomitant leg length discrepancy 2. Look for turning on block 3. Screening 1. Walk on the toes 2. Walk on the heels 3. Squat down – Active Range of Motion testing SPECIAL TESTS 1. Leg Length Discrepancy a. Look at patients back for evidence of a functional scoliosis b. Place your hands on the patients Iliac crests looking for inequality which may mean a leg length discrepancy IN SITTING NEUROLOGIC EXAMINATION 1. Test the reflexes a. L4 – Quadriceps reflex VASCULAR EXAMINATION 1. Feel for the posterior tibial artery SUPINE POSITION INSPECTION 1. -

SIMMONDS TEST: Patient Is Prone Doctor Flexes the Patients Knee to 90 Degrees Doctor Squeezes the Patient’S Calf
Clinical Orthopedic Testing Review SIMMONDS TEST: Patient is prone Doctor flexes the patients knee to 90 degrees Doctor squeezes the patient’s calf. Classical response: Failure of ankle plantarflexion Classical Importance= torn Achilles tendon Test is done bilaterally ACHILLES TAP: Patient is prone Doctor flexes the patient’s knee to 90 degree Doctor dorsiflexes the ankle and then strikes the Achilles tendon with a percussion hammer Classical response: Plantar response Classical Importance= Intact Achilles tendon Test is done bilaterally FOOT DRAWER TEST: Patient is supine with their ankles off the edge of the examination table Doctor grasps the heel of the ankle being tested with one hand and the tibia just above the ankle with the other. Doctor applies and anterior to posterior and then a posterior to anterior sheer force. Classical response: Anterior or posterior translation of the ankle Classical Importance= Anterior talofibular or posterior talofibular ligament laxity. Test is done bilaterally LATERAL STABILITY TEST: Patient is supine Doctor grasps the tibia with one hand and the foot with the other. Doctor rotates the foot into inversion Classical response: Excessive inversion Classical Importance= Anterior talofibular ligament sprain Test is done bilaterally MEDIAL STABILITY TEST: Patient is supine Doctor grasps the tibia with one hand and the foot with the other Doctor rotates the foot into eversion Classical response: Excessive eversion Classical Importance= Deltoid ligament sprain Test is done bilaterally 1 Clinical Orthopedic Testing Review KLEIGER’S TEST: Patient is seated with the legs and feet dangling off the edge of the examination table. Doctor grasps the patient’s foot while stabilizing the tibia with the other hand Doctor pulls the ankle laterally. -

Knee Pain in Children: Part I: Evaluation
Knee Pain in Children: Part I: Evaluation Michael Wolf, MD* *Pediatrics and Orthopedic Surgery, St Christopher’s Hospital for Children, Philadelphia, PA. Practice Gap Clinicians who evaluate knee pain must understand how the history and physical examination findings direct the diagnostic process and subsequent management. Objectives After reading this article, the reader should be able to: 1. Obtain an appropriate history and perform a thorough physical examination of a patient presenting with knee pain. 2. Employ an algorithm based on history and physical findings to direct further evaluation and management. HISTORY Obtaining a thorough patient history is crucial in identifying the cause of knee pain in a child (Table). For example, a history of significant swelling without trauma suggests bacterial infection, inflammatory conditions, or less likely, intra- articular derangement. A history of swelling after trauma is concerning for potential intra-articular derangement. A report of warmth or erythema merits consideration of bacterial in- fection or inflammatory conditions, and mechanical symptoms (eg, lock- ing, catching, instability) should prompt consideration of intra-articular derangement. Nighttime pain and systemic symptoms (eg, fever, sweats, night sweats, anorexia, malaise, fatigue, weight loss) are associated with bacterial infections, inflammatory conditions, benign and malignant musculoskeletal tumors, and other systemic malignancies. A history of rash or known systemic inflammatory conditions, such as systemic lupus erythematosus or inflammatory bowel disease, should raise suspicion for inflammatory arthritis. Ascertaining the location of the pain also can aid in determining the cause of knee pain. Anterior pain suggests patellofemoral syndrome or instability, quad- riceps or patellar tendinopathy, prepatellar bursitis, or apophysitis (patellar or tibial tubercle). -
Using a Study on Arsenic Ingestion and Bladder Cancer As an Example How-Ran Guo1,2,3
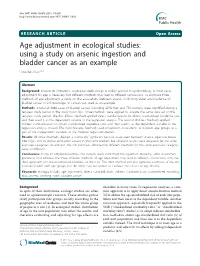
Guo BMC Public Health 2011, 11:820 http://www.biomedcentral.com/1471-2458/11/820 RESEARCHARTICLE Open Access Age adjustment in ecological studies: using a study on arsenic ingestion and bladder cancer as an example How-Ran Guo1,2,3 Abstract Background: Despite its limitations, ecological study design is widely applied in epidemiology. In most cases, adjustment for age is necessary, but different methods may lead to different conclusions. To compare three methods of age adjustment, a study on the associations between arsenic in drinking water and incidence of bladder cancer in 243 townships in Taiwan was used as an example. Methods: A total of 3068 cases of bladder cancer, including 2276 men and 792 women, were identified during a ten-year study period in the study townships. Three methods were applied to analyze the same data set on the ten-year study period. The first (Direct Method) applied direct standardization to obtain standardized incidence rate and then used it as the dependent variable in the regression analysis. The second (Indirect Method) applied indirect standardization to obtain standardized incidence ratio and then used it as the dependent variable in the regression analysis instead. The third (Variable Method) used proportions of residents in different age groups as a part of the independent variables in the multiple regression models. Results: All three methods showed a statistically significant positive association between arsenic exposure above 0.64 mg/L and incidence of bladder cancer in men and women, but different results were observed for the other exposure categories. In addition, the risk estimates obtained by different methods for the same exposure category were all different. -

Sensitivity and Specificity. Wikipedia. Last Modified on 16 November 2013
Sensitivity and specificity - Wikipedia, the free encyclopedia Create account Log in Article Talk Read Edit View Sensitivity and specificity From Wikipedia, the free encyclopedia Main page Contents Sensitivity and specificity are statistical measures of the performance of a binary classification test, also known in statistics as Featured content classification function. Sensitivity (also called the true positive rate, or the recall rate in some fields) measures the proportion of Current events actual positives which are correctly identified as such (e.g. the percentage of sick people who are correctly identified as having Random article the condition). Specificity measures the proportion of negatives which are correctly identified as such (e.g. the percentage of Donate to Wikipedia healthy people who are correctly identified as not having the condition, sometimes called the true negative rate). These two measures are closely related to the concepts of type I and type II errors. A perfect predictor would be described as 100% Interaction sensitive (i.e. predicting all people from the sick group as sick) and 100% specific (i.e. not predicting anyone from the healthy Help group as sick); however, theoretically any predictor will possess a minimum error bound known as the Bayes error rate. About Wikipedia For any test, there is usually a trade-off between the measures. For example: in an airport security setting in which one is testing Community portal for potential threats to safety, scanners may be set to trigger on low-risk items like belt buckles and keys (low specificity), in Recent changes order to reduce the risk of missing objects that do pose a threat to the aircraft and those aboard (high sensitivity). -
A Beginner's Guide to Conducting Reproducible Research
1 A Beginner’s Guide to Conducting Reproducible 2 Research 1,2 1,3 3 Jesse M. Alston and Jessica A. Rick 1 4 Program in Ecology, University of Wyoming, 1000 E University Dr., Laramie, WY 82072 USA 2 5 Department of Zoology and Physiology, University of Wyoming, 1000 E University Dr., Laramie, WY 6 82072 USA 3 7 Department of Botany, University of Wyoming, 1000 E University Dr., Laramie, WY 82072 USA 1 8 Abstract 9 Reproducible research is widely acknowledged as an important tool for improving science and 10 reducing harm from the “replication crisis”, yet research in most fields within biology remains 11 largely irreproducible. In this article, we make the case for why all research should be 12 reproducible, explain why research is often not reproducible, and offer a simple framework that 13 researchers can use to make their research more reproducible. Researchers can increase the 14 reproducibility of their work by improving data management practices, writing more readable 15 code, and increasing use of the many available platforms for sharing data and code. While 16 reproducible research is often associated with a set of advanced tools for sharing data and code, 17 reproducibility is just as much about maintaining work habits that are already widely 18 acknowledged as best practices for research. Increasing reproducibility will increase rigor, 19 trustworthiness, and transparency while benefiting both practitioners of reproducible research and 20 their fellow researchers. 21 Key words: data management, data repository, software, open science, replication 22 Introduction 23 Replication is a fundamental tenet of science, but there is increasing fear among scientists that too 24 few scientific studies can be replicated. -
Coffee Consumption and Its Inverse Relationship with Gastric
nutrients Communication Coffee Consumption and Its Inverse Relationship with Gastric Cancer: An Ecological Study Luis G. Parra-Lara 1 , Diana M. Mendoza-Urbano 2 , Juan C. Bravo 3, Constain H. Salamanca 4 and Ángela R. Zambrano 5,* 1 Facultad de Ciencias de la Salud, Universidad Icesi, Cali 760032, Valle del Cauca, Colombia; [email protected] 2 Centro de Investigaciones Clínicas (CIC), Fundación Valle del Lili, Cali 760032, Valle del Cauca, Colombia; [email protected] 3 Department of Pathology, Fundación Valle del Lili, Cali 760032, Valle del Cauca, Colombia; [email protected] 4 Laboratorio de Diseño y Formulación de Producto, Departamento de Ciencias Farmacéuticas, Facultad de Ciencias Naturales, Universidad Icesi, Cali 760032, Valle del Cauca, Colombia; [email protected] 5 Department of Hemato-Oncology, Fundación Valle del Lili, Cali 760032, Valle del Cauca, Colombia * Correspondence: [email protected]; Tel.: +57-314-888-39-72 Received: 3 August 2020; Accepted: 21 September 2020; Published: 2 October 2020 Abstract: Coffee is the second most popular drink worldwide, and it has various components with antioxidant and antitumor properties. Due to its chemical composition, it could act as an antitumor substance in the gastrointestinal tract. The objective of this study was to explore the relationship between coffee consumption and the incidence/mortality of stomach cancer in the highest-consuming countries. An ecological study using Spearman’s correlation coefficient was performed. The WorldAtlas’s dataset of coffee consumption and the incidence/mortality rates database of the International Agency for Research were used as sources of information. A total of 25 countries were entered to the study. -

Physical Examination Findings and Their Relationship with Performance-Based Function in Adults with Knee Osteoarthritis Maura D
Iversen et al. BMC Musculoskeletal Disorders (2016) 17:273 DOI 10.1186/s12891-016-1151-3 RESEARCH ARTICLE Open Access Physical examination findings and their relationship with performance-based function in adults with knee osteoarthritis Maura D. Iversen1,2,3*, Lori Lyn Price4,5, Johan von Heideken1,3, William F. Harvey6 and Chenchen Wang6 Abstract Background: Many physical examination (PE) maneuvers exist to assess knee function, none of which are specific to knee osteoarthritis (KOA). The Osteoarthritis Research Society International also recommends the use of six functional performance measures to assess function in adults with KOA. While earlier studies have examined the relationship between PE findings and self-reported function or PE findings and select performance tests in adults with knee pain and KOA, few have examined the all three types of measures. This cross-sectional study specifically examines the relationships between results of PE findings, functional performance tests and self-reported function in adults with symptomatic KOA. Methods: We used baseline PE data from a prospective randomized controlled trial in 87 participants aged ≥40 years with symptomatic and radiographic KOA. The PE performed by three experienced physical therapists included: muscle assessment, function and special tests. Participants also completed functional performance tests and the Western Ontario and McMaster Osteoarthritis Index (WOMAC). Multivariate linear regression identified contributions of PE findings towards functional performance and WOMAC scores, adjusting for age and gender. Results: Participants’ mean age was 60.4 years (SD = 10.5), mean disease duration was 8.4 years (SD = 10.1) and 27 participants had varus knee alignment. Mean WOMAC pain and function scores were 211 (SD = 113) and 709 (SD = 394), respectively. -

Overview of Epidemiological Study Designs
University of Massachusetts Medical School eScholarship@UMMS PEER Liberia Project UMass Medical School Collaborations in Liberia 2018-11 Overview of Epidemiological Study Designs Richard Ssekitoleko Yale University Let us know how access to this document benefits ou.y Follow this and additional works at: https://escholarship.umassmed.edu/liberia_peer Part of the Clinical Epidemiology Commons, Epidemiology Commons, Family Medicine Commons, Infectious Disease Commons, Medical Education Commons, and the Quantitative, Qualitative, Comparative, and Historical Methodologies Commons Repository Citation Ssekitoleko R. (2018). Overview of Epidemiological Study Designs. PEER Liberia Project. https://doi.org/ 10.13028/fp3z-mv12. Retrieved from https://escholarship.umassmed.edu/liberia_peer/5 This material is brought to you by eScholarship@UMMS. It has been accepted for inclusion in PEER Liberia Project by an authorized administrator of eScholarship@UMMS. For more information, please contact [email protected]. Overview of Epidemiological study Designs Richard Ssekitoleko Department of Global Health Yale University 1.1 Objectives • Understand the different epidemiological study types • Get to know what is involved in each type of study • Understand the strengths and Limitations of each study type Key terms • Population • Consists of all elements and is the group from which a sample is drawn • A sample is a subset of a population • Parameters • Summary data from a population • Statistics • Summary data from a sample • Validity • Extent to which a conclusion or statistic is well-founded and likely corresponds accurately to the parameter. Hierarchy of Evidence Study type Observational Interventional Descriptive Experiment Ecological Randomized Controlled Trial Cross-sectional Case-control Cohort Overview of Epidemiologic Study Designs Validity *anecdotes Cost Understanding What Physicians Mean: In my experience … once. -
What Can Ecological Studies Tell Us About Death? Yehuda Neumark
Neumark Israel Journal of Health Policy Research (2017) 6:52 DOI 10.1186/s13584-017-0176-x COMMENTARY Open Access What can ecological studies tell us about death? Yehuda Neumark Abstract: Using an ecological study design, Gordon et al. (Isr J Health Policy Res 6:39, 2017) demonstrate variations in mortality patterns across districts and sub-districts of Israel during 2008–2013. Unlike other epidemiological study designs, the units of analysis in ecological studies are groups of people, often defined geographically, and the exposures and outcomes are aggregated, and often known only at the population-level. The ecologic study has several appealing characteristics (suchasrelianceonpublic-domain anonymous data) alongside a number of important potential limitations including the often mentioned ‘ecological fallacy’.Advantagesand disadvantages of the ecological design are described briefly below. Keywords: Ecological fallacy, Ecological studies, Epidemiology, Mortality, Study design Main text In this journal, Gordon et al. [4] employ an ecological "The aim of epidemiology is to decipher nature with re- design to demonstrate variations in mortality patterns spect to human health and disease, and no one should across districts and sub-districts of Israel during the underestimate the complexities of epidemiological research" five-year period of 2008–2013. Standardized mortality [1]. To achieve this lofty and complex goal, the epide- ratios (SMRs) reveal a 25% excess of kidney disease re- miologic investigative toolbox contains various study lated deaths in the Haifa district, for example, while the methodologies including individual-based experimental risk of death from influenza/pneumonia is 25% lower designs (e.g., randomized controlled trial), individual- there than the national average.