Why a New Research Agenda on Green Spaces and Health Is Needed in Latin America: Results of a Systematic Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Journal of Clinical Trails Market Analysis Advances in Clinical Research and Clinical Trials 2020
Journal of Clinical Trails Market Analysis Advances in Clinical Research and Clinical Trials 2020 Raymond Chong The research report on Global Clinical Trials Market 2019 Other prominent players in the value chain include Mednet keenly analyzes significant features of the industry. The Solutions, Arisglobal, eClinForce Inc., DZS Software Solutions, DSG, analysis servers market size, latest trends, drivers, threats, Inc., Guger Technologies Inc., ICON, Plc., ChemWare Inc., and opportunities, as well as key market segments. It is based on iWeb Technologies Limited. past data and present market needs. Also, involve distinct business approaches accepted by the decision makers. Those intensify growth and make a remarkable stand in the industry. The Clinical Trials market will grow with a significant CAGR between 2019 to 2028. The report segregates the complete market on the basis of key players, geographical areas, and segments. Increasing demand for new medical equipments and medicines among end users, coupled with growing investment for research and development activities for development of effective medicines are major factors driving growth of the global clinical trials market. In addition, increasing number of individuals suffering from chronic diseases as well as changing The clinical trials market is projected to arrive at USD 1.76 conditions and nature of certain types of chronic diseases is billion by 2025, from USD 1.04 billion in 2017 growing at a another factor anticipated to support growth of the global CAGR of 6.7 percent from 2018 to 2025. An upcoming clinical trials market to significant extent. market report contains data for historic year 2016, and the base year of calculation is 2017. -
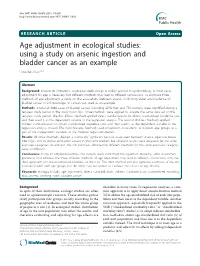
Using a Study on Arsenic Ingestion and Bladder Cancer As an Example How-Ran Guo1,2,3
Guo BMC Public Health 2011, 11:820 http://www.biomedcentral.com/1471-2458/11/820 RESEARCHARTICLE Open Access Age adjustment in ecological studies: using a study on arsenic ingestion and bladder cancer as an example How-Ran Guo1,2,3 Abstract Background: Despite its limitations, ecological study design is widely applied in epidemiology. In most cases, adjustment for age is necessary, but different methods may lead to different conclusions. To compare three methods of age adjustment, a study on the associations between arsenic in drinking water and incidence of bladder cancer in 243 townships in Taiwan was used as an example. Methods: A total of 3068 cases of bladder cancer, including 2276 men and 792 women, were identified during a ten-year study period in the study townships. Three methods were applied to analyze the same data set on the ten-year study period. The first (Direct Method) applied direct standardization to obtain standardized incidence rate and then used it as the dependent variable in the regression analysis. The second (Indirect Method) applied indirect standardization to obtain standardized incidence ratio and then used it as the dependent variable in the regression analysis instead. The third (Variable Method) used proportions of residents in different age groups as a part of the independent variables in the multiple regression models. Results: All three methods showed a statistically significant positive association between arsenic exposure above 0.64 mg/L and incidence of bladder cancer in men and women, but different results were observed for the other exposure categories. In addition, the risk estimates obtained by different methods for the same exposure category were all different. -

Sensitivity and Specificity. Wikipedia. Last Modified on 16 November 2013
Sensitivity and specificity - Wikipedia, the free encyclopedia Create account Log in Article Talk Read Edit View Sensitivity and specificity From Wikipedia, the free encyclopedia Main page Contents Sensitivity and specificity are statistical measures of the performance of a binary classification test, also known in statistics as Featured content classification function. Sensitivity (also called the true positive rate, or the recall rate in some fields) measures the proportion of Current events actual positives which are correctly identified as such (e.g. the percentage of sick people who are correctly identified as having Random article the condition). Specificity measures the proportion of negatives which are correctly identified as such (e.g. the percentage of Donate to Wikipedia healthy people who are correctly identified as not having the condition, sometimes called the true negative rate). These two measures are closely related to the concepts of type I and type II errors. A perfect predictor would be described as 100% Interaction sensitive (i.e. predicting all people from the sick group as sick) and 100% specific (i.e. not predicting anyone from the healthy Help group as sick); however, theoretically any predictor will possess a minimum error bound known as the Bayes error rate. About Wikipedia For any test, there is usually a trade-off between the measures. For example: in an airport security setting in which one is testing Community portal for potential threats to safety, scanners may be set to trigger on low-risk items like belt buckles and keys (low specificity), in Recent changes order to reduce the risk of missing objects that do pose a threat to the aircraft and those aboard (high sensitivity). -
A Beginner's Guide to Conducting Reproducible Research
1 A Beginner’s Guide to Conducting Reproducible 2 Research 1,2 1,3 3 Jesse M. Alston and Jessica A. Rick 1 4 Program in Ecology, University of Wyoming, 1000 E University Dr., Laramie, WY 82072 USA 2 5 Department of Zoology and Physiology, University of Wyoming, 1000 E University Dr., Laramie, WY 6 82072 USA 3 7 Department of Botany, University of Wyoming, 1000 E University Dr., Laramie, WY 82072 USA 1 8 Abstract 9 Reproducible research is widely acknowledged as an important tool for improving science and 10 reducing harm from the “replication crisis”, yet research in most fields within biology remains 11 largely irreproducible. In this article, we make the case for why all research should be 12 reproducible, explain why research is often not reproducible, and offer a simple framework that 13 researchers can use to make their research more reproducible. Researchers can increase the 14 reproducibility of their work by improving data management practices, writing more readable 15 code, and increasing use of the many available platforms for sharing data and code. While 16 reproducible research is often associated with a set of advanced tools for sharing data and code, 17 reproducibility is just as much about maintaining work habits that are already widely 18 acknowledged as best practices for research. Increasing reproducibility will increase rigor, 19 trustworthiness, and transparency while benefiting both practitioners of reproducible research and 20 their fellow researchers. 21 Key words: data management, data repository, software, open science, replication 22 Introduction 23 Replication is a fundamental tenet of science, but there is increasing fear among scientists that too 24 few scientific studies can be replicated. -
Coffee Consumption and Its Inverse Relationship with Gastric
nutrients Communication Coffee Consumption and Its Inverse Relationship with Gastric Cancer: An Ecological Study Luis G. Parra-Lara 1 , Diana M. Mendoza-Urbano 2 , Juan C. Bravo 3, Constain H. Salamanca 4 and Ángela R. Zambrano 5,* 1 Facultad de Ciencias de la Salud, Universidad Icesi, Cali 760032, Valle del Cauca, Colombia; [email protected] 2 Centro de Investigaciones Clínicas (CIC), Fundación Valle del Lili, Cali 760032, Valle del Cauca, Colombia; [email protected] 3 Department of Pathology, Fundación Valle del Lili, Cali 760032, Valle del Cauca, Colombia; [email protected] 4 Laboratorio de Diseño y Formulación de Producto, Departamento de Ciencias Farmacéuticas, Facultad de Ciencias Naturales, Universidad Icesi, Cali 760032, Valle del Cauca, Colombia; [email protected] 5 Department of Hemato-Oncology, Fundación Valle del Lili, Cali 760032, Valle del Cauca, Colombia * Correspondence: [email protected]; Tel.: +57-314-888-39-72 Received: 3 August 2020; Accepted: 21 September 2020; Published: 2 October 2020 Abstract: Coffee is the second most popular drink worldwide, and it has various components with antioxidant and antitumor properties. Due to its chemical composition, it could act as an antitumor substance in the gastrointestinal tract. The objective of this study was to explore the relationship between coffee consumption and the incidence/mortality of stomach cancer in the highest-consuming countries. An ecological study using Spearman’s correlation coefficient was performed. The WorldAtlas’s dataset of coffee consumption and the incidence/mortality rates database of the International Agency for Research were used as sources of information. A total of 25 countries were entered to the study. -

Overview of Epidemiological Study Designs
University of Massachusetts Medical School eScholarship@UMMS PEER Liberia Project UMass Medical School Collaborations in Liberia 2018-11 Overview of Epidemiological Study Designs Richard Ssekitoleko Yale University Let us know how access to this document benefits ou.y Follow this and additional works at: https://escholarship.umassmed.edu/liberia_peer Part of the Clinical Epidemiology Commons, Epidemiology Commons, Family Medicine Commons, Infectious Disease Commons, Medical Education Commons, and the Quantitative, Qualitative, Comparative, and Historical Methodologies Commons Repository Citation Ssekitoleko R. (2018). Overview of Epidemiological Study Designs. PEER Liberia Project. https://doi.org/ 10.13028/fp3z-mv12. Retrieved from https://escholarship.umassmed.edu/liberia_peer/5 This material is brought to you by eScholarship@UMMS. It has been accepted for inclusion in PEER Liberia Project by an authorized administrator of eScholarship@UMMS. For more information, please contact [email protected]. Overview of Epidemiological study Designs Richard Ssekitoleko Department of Global Health Yale University 1.1 Objectives • Understand the different epidemiological study types • Get to know what is involved in each type of study • Understand the strengths and Limitations of each study type Key terms • Population • Consists of all elements and is the group from which a sample is drawn • A sample is a subset of a population • Parameters • Summary data from a population • Statistics • Summary data from a sample • Validity • Extent to which a conclusion or statistic is well-founded and likely corresponds accurately to the parameter. Hierarchy of Evidence Study type Observational Interventional Descriptive Experiment Ecological Randomized Controlled Trial Cross-sectional Case-control Cohort Overview of Epidemiologic Study Designs Validity *anecdotes Cost Understanding What Physicians Mean: In my experience … once. -
What Can Ecological Studies Tell Us About Death? Yehuda Neumark
Neumark Israel Journal of Health Policy Research (2017) 6:52 DOI 10.1186/s13584-017-0176-x COMMENTARY Open Access What can ecological studies tell us about death? Yehuda Neumark Abstract: Using an ecological study design, Gordon et al. (Isr J Health Policy Res 6:39, 2017) demonstrate variations in mortality patterns across districts and sub-districts of Israel during 2008–2013. Unlike other epidemiological study designs, the units of analysis in ecological studies are groups of people, often defined geographically, and the exposures and outcomes are aggregated, and often known only at the population-level. The ecologic study has several appealing characteristics (suchasrelianceonpublic-domain anonymous data) alongside a number of important potential limitations including the often mentioned ‘ecological fallacy’.Advantagesand disadvantages of the ecological design are described briefly below. Keywords: Ecological fallacy, Ecological studies, Epidemiology, Mortality, Study design Main text In this journal, Gordon et al. [4] employ an ecological "The aim of epidemiology is to decipher nature with re- design to demonstrate variations in mortality patterns spect to human health and disease, and no one should across districts and sub-districts of Israel during the underestimate the complexities of epidemiological research" five-year period of 2008–2013. Standardized mortality [1]. To achieve this lofty and complex goal, the epide- ratios (SMRs) reveal a 25% excess of kidney disease re- miologic investigative toolbox contains various study lated deaths in the Haifa district, for example, while the methodologies including individual-based experimental risk of death from influenza/pneumonia is 25% lower designs (e.g., randomized controlled trial), individual- there than the national average. -

Analytic Studies Number of Observations Directionality Of
Introductory Epidemiology (HSC4933) Analytic studies • Analytic studies serve to identify the causes of disease and thus are important as they can lead to the prevention of disease Analytic Epidemiology • They are also useful for evaluating treatments and other health interventions Types of study design • They can be either observational or interventional • They explore associations between exposures and outcomes Factors to help identify the type of The selection of study subjects study design • How individuals are selected for the study • Have a new disease or exposure – Case series, case report • Number of observations • Representative of a group • Directionality of the exposure – Cross sectional study, ecological study • Chosen based on having and not having a disease • Data collection methods – Case‐control study • Timing of data collection • Chosen based on having and not having a certain exposure – Cohort study • Unit of observation • Chosen because they have (or are at risk o having) a condition and the researcher wants to evaluate a treatment • Availability of subjects – Randomized clinical trial, intervention study Number of observations Directionality of exposure • Only one data collection period • Retrospective approach ‐ a researcher obtains information on past exposures – Generally a cross‐sectional or ecologic study, and many case‐control studies – Common in case‐control studies • Single point in time • Multiple observations and followed over time Cross‐sectional study, ecologic study – – Cohort study, randomized clinical -

Linkage Failures in Ecologic Studiesa
Linkage failures in ecologic studiesa Markku Nurminenb World Health Statistics Quaterly 1995; 48, 78-84 Abstract Ecological studies require a methodological theory distinct from that used in individual-level epidemiological studies. This article discusses the special problems that need to be considered when planning ecological studies or using the results of such studies. Ecological studies are much more sensitive to bias from model mis-specification than are results from individual-level studies. For example, deviations from linearity in the underlying individual-level regressions can lead to inability to control for confounding in ecological studies, even if no misclassification is present. Conditions for confounding differ in individual-level and ecological analyses. For ecological analyses of means, for example, a covariate will not be a confounder if its mean value in a study region is not associated with either (i) the mean exposure level across regions, or (ii) the mean outcome (disease rate) across regions. On the other hand, effect modification across areas can induce ecological bias even when the number of areas is very large and there is no confounding. In contrast to individual-level studies, independent and nondifferential misclassification of a dichotomous exposure usually leads to bias away from the null hypothesis in aggregate data studies. Failure to standardize disease, exposure and covariate data for other confounders (not included in the regression model) can lead to bias. It should be borne in mind that there is no method available to identify or measure ecological bias. While this conclusion may sound like a general criticism of ecological studies, it is not. -

Drug Designing: Open Access
Drug Designing: Open Access Market Analysis 2nd Global expo on Clinical Trials and Clinical Research Alena Clancy The worldwide clinical trials advertise estimate was needs. Also, involve distinct business approaches accepted esteemed at USD 40.0 billion of every 2016 and is relied by the choice makers. That intensifies growth and makes a upon to develop at a CAGR of 5.7% over the gauge time remarkable stand in the industry. The Clinical Trials frame. Key drivers affecting the market development are market will grow with a big CAGR between 2019 to 2028. globalization of clinical trials, improvement of latest The report segregates the entire market on the idea of key medications, for instance, customized prescription, players, geographical areas, and segments. expanding advancement in innovation, and boosting interest for CROs to lead clinical trials. CROs enhanced Increasing demand for brand spanking new medical mastery when contrasted with pharma organizations equipment’s and medicines among end users, including concerning performing clinical trials in wide exhibit of growing investment for research and development activities topographies and advancement of medications in particular for development of effective medicines are major factors restorative zones are few components in charge of the driving growth of the global clinical trials market. In developing interest for the CROs in pharmaceutical addition, increasing number of individuals suffering from section. As indicated by BioOutsource, the interest for chronic diseases as well as changing conditions and nature biosimilars testing is required to increment in the U.S. This of certain types of chronic diseases is another factor is credited to the way that the FDA at long last began anticipated to support growth of the worldwide clinical tending to the absence of clear direction with respect to trials market to significant extent. -

Cohort Studies and Relative Risks
University of Massachusetts Medical School eScholarship@UMMS PEER Liberia Project UMass Medical School Collaborations in Liberia 2019-2 Cohort Studies and Relative Risks Richard Ssekitoleko Yale University Let us know how access to this document benefits ou.y Follow this and additional works at: https://escholarship.umassmed.edu/liberia_peer Part of the Clinical Epidemiology Commons, Epidemiology Commons, Family Medicine Commons, Infectious Disease Commons, Medical Education Commons, and the Statistics and Probability Commons Repository Citation Ssekitoleko R. (2019). Cohort Studies and Relative Risks. PEER Liberia Project. https://doi.org/10.13028/ 17f0-7y26. Retrieved from https://escholarship.umassmed.edu/liberia_peer/14 This material is brought to you by eScholarship@UMMS. It has been accepted for inclusion in PEER Liberia Project by an authorized administrator of eScholarship@UMMS. For more information, please contact [email protected]. Cohort studies and Relative risks Richard Ssekitoleko Objectives • Define a cohort study and the steps for the study • Understand the populations in a cohort study • Understand timing in a cohort study and the difference between retrospective, prospective and ambi-directional cohort studies • Understand the selection of the cohort population and the collection of exposure and outcome data • Understand the sources of bias in a cohort study • Understand the calculation and interpretation of the relative risk • Understand use of the new-castle Ottawa quality assessment score for cohort studies -
Bias and Confounding
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this site. Copyright 2008, The Johns Hopkins University and Sukon Kanchanaraksa. All rights reserved. Use of these materials permitted only in accordance with license rights granted. Materials provided “AS IS”; no representations or warranties provided. User assumes all responsibility for use, and all liability related thereto, and must independently review all materials for accuracy and efficacy. May contain materials owned by others. User is responsible for obtaining permissions for use from third parties as needed. Bias and Confounding Sukon Kanchanaraksa, PhD Johns Hopkins University Section A Exposure and Disease Association The Study Question An epidemiologic investigation ⇒ etiology of disease − Study hypothesis X A specific statement regarding the relationship between two variables: exposure and disease outcome 4 Association An epidemiologic study ⇒ test the hypothesis of association between exposure and outcome − If there is an association, the exposure is called a risk factor of the disease A risk factor can be either: − A predictor (marker or proxy) X Such as employment in a specific industry or − A causal factor X Such as exposure to benzene at work 5 From Association to Causation Steps in the study of the etiology of disease Limitations and issues in deriving inferences from epidemiologic studies − Bias and confounding −