Acquired Electrophysiological Remodeling and Cardiac Arrhythmias
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
The QT Interval: How Long Is Too Long?
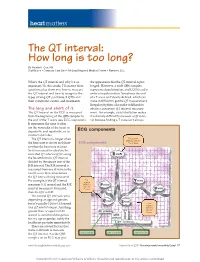
heart matters The QT interval: How long is too long? By Natalie K. Cox, RN Staff Nurse • Coronary Care Unit • McLeod Regional Medical Center • Florence, S.C. What’s the QT interval and why’s it so the appearance that the QT interval is pro- important? In this article, I’ll answer these longed. However, a wide QRS complex questions plus show you how to measure represents depolarization, and LQTS is a dis- the QT interval and how to recognize the order of repolarization. Sometimes the end types of long QT syndrome (LQTS) and of a T wave isn’t clearly defi ned, which can their symptoms, causes, and treatments. make it diffi cult to get the QT measurement. Irregular rhythms also make it diffi cult to The long and short of it obtain a consistent QT interval measure- The QT interval on the ECG is measured ment. For example, atrial fi brillation makes from the beginning of the QRS complex to it extremely diffi cult to measure a QT inter- the end of the T wave (see ECG components). val because fi nding a T wave isn’t always It represents the time it takes for the ventricles of the heart to depolarize and repolarize, or to ECG components contract and relax. The QT interval is longer when First positive deflection after the the heart rate is slower and short- ECG components P or Q wave er when the heart rate is faster. So it’s necessary to calculate the corrected QT interval (QTc) using the Bazett formula: QT interval divided by the square root of the R-R interval. -

Heart Rate Information Sheet Finding Your Pulse Taking Your Pulse
Heart rate In this activity you will measure your heart rate and investigate the effect that other things have on your heart rate. Information sheet You can measure your heart (pulse) rate anywhere on your body where a major artery is close to the surface of your skin. The easiest places are: • on the front of your forearm • just above your wrist on your thumb side • on the side of your neck about half way between your chin and your ear. Finding your pulse Try to locate your pulse in one of these places, using the tips of your index and middle fingers. You should feel a gentle, regular beat. This is your heart rate. Do not use your thumb, as your thumb has a pulse of its own. Taking your pulse When you find your pulse, use a stopwatch or a watch with a second hand to count how many beats there are in a full minute (60 seconds). In most situations, taking your pulse rate over one minute will give a reasonably accurate result, but if you want to take your pulse after exercise, you should do so over a much shorter time interval. After exercise your pulse rate will be changing rapidly. To get a reasonably accurate result, start to measure the rate immediately after the exercise and count the number of beats in 10 seconds. Multiply this number by six to find your heart rate. For an adult, a normal resting heart rate is between 60–100 beats a minute. The fitter you are, the lower your resting heart beat will be. -

Heart to Heart - STEAM Activity
Heart to Heart - STEAM Activity Purpose: The main objective of this exercise is to introduce how the human heart works. This lesson will be divided into four different lessons, including an introduction to heart anatomy, heart beats and pulses, and the circulatory system. We will be using coloring activities, stethoscopes, and handmade pumps to reinforce the concepts seen in this lesson. Vocabulary ● Artery: A blood vessel that carries blood high in oxygen content away from the heart to the farthest reaches of the body. ● Vein: a Blood vessel that carries blood low in oxygen content from the body back to the heart. ● Atrium: One of the two upper cavities of the heart that passes blood to the ventricles. ● Ventricles: One of the two lower chambers of the heart that receives blood from the atria. ● Valves: Tissue-paper thin membranes attached to the heart wall that constantly open and close to regulate blood flow. ● Pulse: A rhythmical, mechanical throbbing of the arteries as blood pumps through them. ● Heart Rate: The number of times per minute that the heart contracts - the number of heart beats per minute (bpm). ● Taquicardia: A high resting heart rate that is usually higher than 100 beats per minute. ● Bradycardia: A low resting heart rate that is usually lower than 60 beats per minute. ● Circulation: The movement of blood through the vessels of the body by the pumping action of the heart. It distributes nutrients and oxygen and removes waste products from all parts of the body. ● Pulmonary Circulation: The portion of the circulatory system that carries deoxygenated blood from the heart to the lungs and oxygenated blood back to the heart. -

書 名 等 発行年 出版社 受賞年 備考 N1 Ueber Das Zustandekommen Der
書 名 等 発行年 出版社 受賞年 備考 Ueber das Zustandekommen der Diphtherie-immunitat und der Tetanus-Immunitat bei thieren / Emil Adolf N1 1890 Georg thieme 1901 von Behring N2 Diphtherie und tetanus immunitaet / Emil Adolf von Behring und Kitasato 19-- [Akitomo Matsuki] 1901 Malarial fever its cause, prevention and treatment containing full details for the use of travellers, University press of N3 1902 1902 sportsmen, soldiers, and residents in malarious places / by Ronald Ross liverpool Ueber die Anwendung von concentrirten chemischen Lichtstrahlen in der Medicin / von Prof. Dr. Niels N4 1899 F.C.W.Vogel 1903 Ryberg Finsen Mit 4 Abbildungen und 2 Tafeln Twenty-five years of objective study of the higher nervous activity (behaviour) of animals / Ivan N5 Petrovitch Pavlov ; translated and edited by W. Horsley Gantt ; with the collaboration of G. Volborth ; and c1928 International Publishing 1904 an introduction by Walter B. Cannon Conditioned reflexes : an investigation of the physiological activity of the cerebral cortex / by Ivan Oxford University N6 1927 1904 Petrovitch Pavlov ; translated and edited by G.V. Anrep Press N7 Die Ätiologie und die Bekämpfung der Tuberkulose / Robert Koch ; eingeleitet von M. Kirchner 1912 J.A.Barth 1905 N8 Neue Darstellung vom histologischen Bau des Centralnervensystems / von Santiago Ramón y Cajal 1893 Veit 1906 Traité des fiévres palustres : avec la description des microbes du paludisme / par Charles Louis Alphonse N9 1884 Octave Doin 1907 Laveran N10 Embryologie des Scorpions / von Ilya Ilyich Mechnikov 1870 Wilhelm Engelmann 1908 Immunität bei Infektionskrankheiten / Ilya Ilyich Mechnikov ; einzig autorisierte übersetzung von Julius N11 1902 Gustav Fischer 1908 Meyer Die experimentelle Chemotherapie der Spirillosen : Syphilis, Rückfallfieber, Hühnerspirillose, Frambösie / N12 1910 J.Springer 1908 von Paul Ehrlich und S. -
The ECG Made Very Easy Indeed: a Beginner’S Guide
Part 1 The ECG made very easy indeed: a beginner’s guide The ECG made very easy indeed 1 What is an ECG? 1 The heart is a pump driven by intrinsic electrical When do you need an ECG? 1 impulses which make the heart beat. An ECG is a paper recording of that electrical activity. The ECG records where How to record an ECG 2 electrical impulses start and how they flow through the How to interpret an ECG: the basics 2 heart. It does not measure how well the heart is pumping. The electrical activity of the heart starts in the ‘inter- The ECG waves and what they mean 2 nal pacemaker’, which is called the sinoatrial node. This Interpretation starts here! 4 is in the right atrium. The normal rhythm is called ‘sinus rhythm’ (properly it should be called sinoatrial rhythm, Rhythms you must be able to recognize 8 but it isn’t). The way electrical impulses flow through the Patterns you must be able to recognize 10 heart is called conduction. Abnormalities in the electrical activity of the heart can The normal ECG and its variants 13 result in abnormal conduction or rhythms where the heart ECG red flags 14 may go too quickly, too slowly, or beat irregularly. Changes to the normal flow of electricity through the heart can be shown on an ECG and may indicate damaged This guide has been written for those who are just starting heart muscle. Heart muscle can be damaged by many to use ECGs in their clinical practice. -

Baroreflex Sensitivity Impairment During Hypoglycemia
Diabetes Volume 65, January 2016 209 Ajay D. Rao,1,2 Istvan Bonyhay,3 Joel Dankwa,1 Maria Baimas-George,1 Lindsay Kneen,1 Sarah Ballatori,3 Roy Freeman,3 and Gail K. Adler1 Baroreflex Sensitivity Impairment During Hypoglycemia: Implications for Cardiovascular Control Diabetes 2016;65:209–215 | DOI: 10.2337/db15-0871 Studies have shown associations between exposure to of cardiovascular benefit(4–7). These results raise the hypoglycemia and increased mortality, raising the pos- possibility that exposure to hypoglycemia has adverse sibility that hypoglycemia has adverse cardiovascular and unknown effects that persist after hypoglycemia effects. In this study, we determined the acute effects resolves and may oppose cardiovascular benefits of im- of hypoglycemia on cardiovascular autonomic control. proved glycemic control (8,9). Seventeen healthy volunteers were exposed to exper- Prior exposure to hypoglycemia impairs the hormonal imental hypoglycemia (2.8 mmol/L) for 120 min. Car- and muscle sympathetic nerve activity (MSNA) response fl COMPLICATIONS diac vagal barore ex function was assessed using the to subsequent hypoglycemia (10), the hormonal responses fi modi ed Oxford method before the initiation of the to subsequent exercise (11), and autonomic control of hypoglycemic-hyperinsulinemic clamp protocol and dur- cardiovascular function (12). After exposure to hypogly- ing the last 30 min of hypoglycemia. During hypoglycemia, cemia, induced by the hypoglycemic-hyperinsulinemic compared with baseline euglycemic conditions, 1)baro- clamp protocol, individuals exhibit decreased baroreflex reflex sensitivity decreases significantly (19.2 6 7.5 vs. 32.9 6 16.6 ms/mmHg, P < 0.005), 2) the systolic blood sensitivity (BRS), decreased MSNA response to transient pressure threshold for baroreflex activation increases hypotension, and decreased norepinephrine response to significantly (the baroreflex function shifts to the right; orthostatic stress compared with prior exposure to 120 6 14 vs. -

Baroreflex and Cerebral Autoregulation Are Inversely
2460 NASR N et al. Circulation Journal ORIGINAL ARTICLE Official Journal of the Japanese Circulation Society http://www.j-circ.or.jp Hypertension and Circulatory Control Baroreflex and Cerebral Autoregulation Are Inversely Correlated Nathalie Nasr, MD, PhD; Marek Czosnyka, PhD; Anne Pavy-Le Traon, MD, PhD; Marc-Antoine Custaud, MD, PhD; Xiuyun Liu, BSc; Georgios V. Varsos, BSc; Vincent Larrue, MD Background: The relative stability of cerebral blood flow is maintained by the baroreflex and cerebral autoregulation (CA). We assessed the relationship between baroreflex sensitivity (BRS) and CA in patients with atherosclerotic carotid stenosis or occlusion. Methods and Results: Patients referred for assessment of atherosclerotic unilateral >50% carotid stenosis or oc- clusion were included. Ten healthy volunteers served as a reference group. BRS was measured using the sequence method. CA was quantified by the correlation coefficient (Mx) between slow oscillations in mean arterial blood pres- sure and mean cerebral blood flow velocities from transcranial Doppler. Forty-five patients (M/F: 36/9), with a me- dian age of 68 years (IQR:17) were included. Thirty-four patients had carotid stenosis, and 11 patients had carotid occlusion (asymptomatic: 31 patients; symptomatic: 14 patients). The median degree of carotid steno-occlusive disease was 90% (IQR:18). Both CA (P=0.02) and BRS (P<0.001) were impaired in patients as compared with healthy volunteers. CA and BRS were inversely and strongly correlated with each other in patients (rho=0.58, P<0.001) and in healthy volunteers (rho=0.939; P<0.001). Increasing BRS remained strongly associated with im- paired CA on multivariate analysis (P=0.004). -

Long QT Syndrome: from Channels to Cardiac Arrhythmias
Long QT syndrome: from channels to cardiac arrhythmias Arthur J. Moss, Robert S. Kass J Clin Invest. 2005;115(8):2018-2024. https://doi.org/10.1172/JCI25537. Review Series Long QT syndrome, a rare genetic disorder associated with life-threatening arrhythmias, has provided a wealth of information about fundamental mechanisms underlying human cardiac electrophysiology that has come about because of truly collaborative interactions between clinical and basic scientists. Our understanding of the mechanisms that control the critical plateau and repolarization phases of the human ventricular action potential has been raised to new levels through these studies, which have clarified the manner in which both potassium and sodium channels regulate this critical period of electrical activity. Find the latest version: https://jci.me/25537/pdf Review series Long QT syndrome: from channels to cardiac arrhythmias Arthur J. Moss1 and Robert S. Kass2 1Heart Research Follow-up Program, Department of Medicine, University of Rochester School of Medicine and Dentistry, Rochester, New York, USA. 2Department of Pharmacology, Columbia University Medical Center, New York, New York, USA. Long QT syndrome, a rare genetic disorder associated with life-threatening arrhythmias, has provided a wealth of information about fundamental mechanisms underlying human cardiac electrophysiology that has come about because of truly collaborative interactions between clinical and basic scientists. Our understanding of the mecha- nisms that control the critical plateau and repolarization phases of the human ventricular action potential has been raised to new levels through these studies, which have clarified the manner in which both potassium and sodium channels regulate this critical period of electrical activity. -

Toolbox-Talks--Blood-Pressure.Pdf
TOOLBOX Toolbox Talk #1 TALKS Blood Pressure vs. Heart Rate While your blood pressure is the force of your blood moving through your blood vessels, your heart rate is the number of times your heart beats per minute. They are two separate measurements and indicators of health. • For people with high blood pressure (HBP or hypertension), there’s no substitute for measuring blood pressure. • Heart rate and blood pressure do not necessarily increase at the same rate. A rising heart rate does not cause your blood pressure to increase at the same Quarter: rate. Even though your heart is beating more times a minute, healthy blood BLOOD vessels dilate (get larger) to allow more blood to flow through more easily. PRESSURE When you exercise, your heart speeds up so more blood can reach your muscles. It may be possible for your heart rate to double safely, while your blood pressure may respond by only increasing a modest amount. Talk Number: Heart Rate and Exercise 1 In discussions about high blood pressure, you will often see heart rate Blood mentioned in relation to exercise. Your target heart rate is based on age and Pressure can help you monitor the intensity of your exercise. vs. • If you measure your heart rate (take your pulse) before, during and after Heart Rate physical activity, you’ll notice it will increase over the course of the exercise. • The greater the intensity of the exercise, the more your heart rate will increase. • When you stop exercising, your heart rate does not immediately return to your normal (resting) heart rate. -

Cardiovascular Physiology
CARDIOVASCULAR PHYSIOLOGY Ida Sletteng Karlsen • Trym Reiberg Second Edition 15 March 2020 Copyright StudyAid 2020 Authors Trym Reiberg Ida Sletteng Karlsen Illustrators Nora Charlotte Sønstebø Ida Marie Lisle Amalie Misund Ida Sletteng Karlsen Trym Reiberg Booklet Disclaimer All rights reserved. No part oF this book may be reproduced in any Form on by an electronic or mechanical means, without permission From StudyAid. Although the authors have made every efFort to ensure the inFormation in the booklet was correct at date of publishing, the authors do not assume and hereby disclaim any liability to any part For any inFormation that is omitted or possible errors. The material is taken From a variety of academic sources as well as physiology lecturers, but are Further incorporated and summarized in an original manner. It is important to note, the material has not been approved by professors of physiology. All illustrations in the booklet are original. This booklet is made especially For students at the Jagiellonian University in Krakow by tutors in the StudyAid group (students at JU). It is available as a PDF and is available for printing. If you have any questions concerning copyrights oF the booklet please contact [email protected]. About StudyAid StudyAid is a student organization at the Jagiellonian University in Krakow. Throughout the academic year we host seminars in the major theoretical subjects: anatomy, physiology, biochemistry, immunology, pathophysiology, supplementing the lectures provided by the university. We are a group of 25 tutors, who are students at JU, each with their own Field oF specialty. To make our seminars as useful and relevant as possible, we teach in an interactive manner often using drawings and diagrams to help students remember the concepts. -

Increased Baroreflex Sensitivity and Reduced Cardiovascular Reactivity
1873 Hypertens Res Vol.31 (2008) No.10 p.1873-1878 Original Article Increased Baroreflex Sensitivity and Reduced Cardiovascular Reactivity in Individuals with Chronic Low Blood Pressure Stefan DUSCHEK1), Anja DIETEL1), Rainer SCHANDRY1), and Gustavo A. REYES DEL PASO2) This study investigated aberrations in baroreflex function and cardiovascular reactivity related to the con- dition of chronic low blood pressure. In 40 hypotensive and 40 normotensive control subjects, blood pres- sures were continuously recorded at rest and during mental stress. Baroreflex sensitivity was determined in the time domain using sequence analysis. Beat-to-beat hemodynamic indices were estimated from the blood pressure waveforms by means of Modelflow analysis. In the hypotensive sample, a higher baroreflex sensitivity was observed under both conditions. Furthermore, this group experienced a less pronounced increase of blood pressure and stroke volume under stress. The findings underline the involvement of the baroreflex in the long-term setting of tonic blood pressure and suggest its relevance in the etiology of chronic hypotension. In addition, this study documents reduced cardiovascular reactivity and thus deficient hemodynamic adjustment to situational requirements in chronic low blood pressure. (Hypertens Res 2008; 31: 1873–1878) Key Words: hypotension, blood pressure, baroreflex, cardiac output, mental stress tory problems when assuming an upright position (5). Introduction The cardiac baroreflex has been considered to be involved in the etiology of chronic hypotension (1, 6). This regulatory Chronic low blood pressure is relatively widespread; it affects system consists of a negative feedback loop in which changes approximately 3% of the general population (1). It is typically in the firing rate of the arterial baroreceptors lead to compen- accompanied by symptoms such as fatigue, reduced drive, satory alterations of heart rate, cardiac contractility, and vaso- faintness, dizziness, headaches, cold limbs, and reduced cog- motor activity (7, 8). -

Non-Coding Rnas in the Cardiac Action Potential and Their Impact on Arrhythmogenic Cardiac Diseases
Review Non-Coding RNAs in the Cardiac Action Potential and Their Impact on Arrhythmogenic Cardiac Diseases Estefania Lozano-Velasco 1,2 , Amelia Aranega 1,2 and Diego Franco 1,2,* 1 Cardiovascular Development Group, Department of Experimental Biology, University of Jaén, 23071 Jaén, Spain; [email protected] (E.L.-V.); [email protected] (A.A.) 2 Fundación Medina, 18016 Granada, Spain * Correspondence: [email protected] Abstract: Cardiac arrhythmias are prevalent among humans across all age ranges, affecting millions of people worldwide. While cardiac arrhythmias vary widely in their clinical presentation, they possess shared complex electrophysiologic properties at cellular level that have not been fully studied. Over the last decade, our current understanding of the functional roles of non-coding RNAs have progressively increased. microRNAs represent the most studied type of small ncRNAs and it has been demonstrated that miRNAs play essential roles in multiple biological contexts, including normal development and diseases. In this review, we provide a comprehensive analysis of the functional contribution of non-coding RNAs, primarily microRNAs, to the normal configuration of the cardiac action potential, as well as their association to distinct types of arrhythmogenic cardiac diseases. Keywords: cardiac arrhythmia; microRNAs; lncRNAs; cardiac action potential Citation: Lozano-Velasco, E.; Aranega, A.; Franco, D. Non-Coding RNAs in the Cardiac Action Potential 1. The Electrical Components of the Adult Heart and Their Impact on Arrhythmogenic The adult heart is a four-chambered organ that propels oxygenated blood to the entire Cardiac Diseases. Hearts 2021, 2, body. It is composed of atrial and ventricular chambers, each of them with distinct left and 307–330.