Nerve-Muscle Pedicle Flap Implantation Combined with Arytenoid Adduction
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Superior Laryngeal Nerve Identification and Preservation in Thyroidectomy
ORIGINAL ARTICLE Superior Laryngeal Nerve Identification and Preservation in Thyroidectomy Michael Friedman, MD; Phillip LoSavio, BS; Hani Ibrahim, MD Background: Injury to the external branch of the su- recorded and compared on an annual basis for both be- perior laryngeal nerve (EBSLN) can result in detrimen- nign and malignant disease. Overall results were also com- tal voice changes, the severity of which varies according pared with those found in previous series identified to the voice demands of the patient. Variations in its ana- through a 50-year literature review. tomic patterns and in the rates of identification re- ported in the literature have discouraged thyroid sur- Results: The 3 anatomic variations of the distal aspect geons from routine exploration and identification of this of the EBSLN as it enters the cricothyroid were encoun- nerve. Inconsistent with the surgical principle of pres- tered and are described. The total identification rate over ervation of critical structures through identification, mod- the 20-year period was 900 (85.1%) of 1057 nerves. Op- ern-day thyroidectomy surgeons still avoid the EBSLN erations performed for benign disease were associated rather than identifying and preserving it. with higher identification rates (599 [86.1%] of 696) as opposed to those performed for malignant disease Objectives: To describe the anatomic variations of the (301 [83.4%] of 361). Operations performed in recent EBSLN, particularly at the junction of the inferior con- years have a higher identification rate (over 90%). strictor and cricothyroid muscles; to propose a system- atic approach to identification and preservation of this Conclusions: Understanding the 3 anatomic variations nerve; and to define the identification rate of this nerve of the distal portion of the EBSLN and its relation to the during thyroidectomy. -

Unusual Morphology of the Superior Belly of Omohyoid Muscle
Case Report http://dx.doi.org/10.5115/acb.2014.47.4.271 pISSN 2093-3665 eISSN 2093-3673 Unusual morphology of the superior belly of omohyoid muscle Rajesh Thangarajan, Prakashchandra Shetty, Srinivasa Rao Sirasanagnadla, Melanie Rose D’souza Department of Anatomy, Melaka Manipal Medical College (Manipal Campus), Manipal University, Manipal, Karnataka, India Abstract: Though anomalies of the superior belly of the omohyoid have been described in medical literature, absence of superior belly of omohyoid is rarely reported. Herein, we report a rare case of unilateral absence of muscular part of superior belly of omohyoid. During laboratory dissections for medical undergraduate students, unusual morphology of the superior belly of the omohyoid muscle has been observed in formalin embalmed male cadaver of South Indian origin. The muscular part of the superior belly of the omohyoid was completely absent. The inferior belly originated normally from the upper border of scapula, and continued with a fibrous tendon which ran vertically lateral to sternohyoid muscle and finally attached to the lower border of the body of hyoid bone. The fibrous tendon was about 1 mm thick and received a nerve supply form the superior root of the ansa cervicalis. As omohyoid mucle is used to achieve the reconstruction of the laryngeal muscles and bowed vocal folds, the knowledge of the possible anomalies of the omohyoid muscle is important during neck surgeries. Key words: Superior belly, Fibrous tendon, Omohyoid, Neck surgery Received March 12, 2014; Revised April 3, 2014; Accepted April 28, 2014 Introduction bellies, absence and adhesion to sternohyoid are the reported anomalies of the superior belly of the OH [2]. -

Unusual Organization of the Ansa Cervicalis: a Case Report
CASE REPORT ISSN- 0102-9010 UNUSUAL ORGANIZATION OF THE ANSA CERVICALIS: A CASE REPORT Ranjana Verma1, Srijit Das2 and Rajesh Suri3 Department of Anatomy, Maulana Azad Medical College, New Delhi-110002, India. ABSTRACT The superior root of the ansa cervicalis is formed by C1 fibers carried by the hypoglossal nerve, whereas the inferior root is contributed by C2 and C3 nerves. We report a rare finding in a 40-year-old male cadaver in which the vagus nerve fused with the hypoglossal nerve immediately after its exit from the skull on the left side. The vagus nerve supplied branches to the sternohyoid, sternothyroid and superior belly of the omohyoid muscles and also contributed to the formation of the superior root of the ansa cervicalis. In this arrangement, paralysis of the infrahyoid muscles may result following lesion of the vagus nerve anywhere in the neck. The cervical location of the vagus nerve was anterior to the common carotid artery within the carotid sheath. This case report may be of clinical interest to surgeons who perform laryngeal reinnervation and neurologists who diagnose nerve disorders. Key words: Ansa cervicalis, hypoglossal nerve, vagus nerve, variations INTRODUCTION cadaver. The right side was normal. The neck region The ansa cervicalis is a nerve loop formed was dissected and the neural structures in the carotid by the union of superior and inferior roots. The and muscular triangle regions were exposed, with superior root is a branch of the hypoglossal nerve particular attention given to the organization of the containing C1 fibers, whereas the inferior root is ansa cervicalis. -

The Role of Strap Muscles in Phonation Laryngeal Model in Vivo
Journal of Voice Vol. 11, No. 1, pp. 23-32 © 1997 Lippincott-Raven Publishers, Philadelphia The Role of Strap Muscles in Phonation In Vivo Canine Laryngeal Model Ki Hwan Hong, *Ming Ye, *Young Mo Kim, *Kevin F. Kevorkian, and *Gerald S. Berke Department of Otolaryngology, Chonbuk National University, Medical School, Chonbuk, Korea; and *Division of Head and Neck Surgery, UCLA School of Medicine, Los Angeles, California, U.S.A. Summary: In spite of the presumed importance of the strap muscles on laryn- geal valving and speech production, there is little research concerning the physiological role and the functional differences among the strap muscles. Generally, the strap muscles have been shown to cause a decrease in the fundamental frequency (Fo) of phonation during contraction. In this study, an in vivo canine laryngeal model was used to show the effects of strap muscles on the laryngeal function by measuring the F o, subglottic pressure, vocal in- tensity, vocal fold length, cricothyroid distance, and vertical laryngeal move- ment. Results demonstrated that the contraction of sternohyoid and sternothy- roid muscles corresponded to a rise in subglottic pressure, shortened cricothy- roid distance, lengthened vocal fold, and raised F o and vocal intensity. The thyrohyoid muscle corresponded to lowered subglottic pressure, widened cricothyroid distance, shortened vocal fold, and lowered F 0 and vocal inten- sity. We postulate that the mechanism of altering F o and other variables after stimulation of the strap muscles is due to the effects of laryngotracheal pulling, upward or downward, and laryngotracheal forward bending, by the external forces during strap muscle contraction. -

Cervical Spine and Cervicothoracic Junction Alexander R
46 Cervical Spine and Cervicothoracic Junction Alexander R. Riccio, Tyler J. Kenning, John W. German SUMMARY OF KEY POINTS the approximate cervical spinal levels for the purposes of the skin incision. These include the hyoid bone (C3), thyroid • Understanding the anatomy of the cervical spine and cartilage (C4-5), cricoid cartilage (C6), and carotid tubercle neck is of the utmost importance for the surgeon (C6). These landmarks, however, may not be universally reli- operating in this region. able because, depending on a patient’s body habitus, they may be difficult to palpate reliably; moreover, the relationships are • The anatomy of this region can be classified from only an estimate and variability exists. superficial to deep and further analyzed by system, The most prominent structure of the upper dorsal surface including muscle, bone, nerves, vasculature, and soft of the nuchal region is the inion, or occipital protuberance. tissue. This may be palpated in the midline and is a part of the • Regarding the nerves in the neck, more focused occipital bone. The spinous processes of the cervical vertebrae consideration is taken for surgical purposes when may then be followed caudally to the vertebral prominence, discussing the laryngeal nerve as a result of the variably corresponding to the spinous process of C6, C7 (most potential morbidity associated with iatrogenic injury common), or T1. to this nerve. The prominent surface structure of the ventral neck is the • The vertebral artery is discussed in specific detail as laryngeal prominence, which is produced by the underlying well due to its clinical importance and proximity to thyroid cartilage. -

A Case of the Human Sternocleidomastoid Muscle Additionally Innervated by the Hypoglossal Nerve
Okajimas Folia Anat. Jpn., 69(6): 361-368, March, 1993 A Case of the Human Sternocleidomastoid Muscle Additionally Innervated by the Hypoglossal Nerve By Masahiro KOIZUMI, Masaharu HORIGUCHI, Shin'ichi SEKIYA, Sumio ISOGAI and Masato NAKANO Department of Anatomy, Iwate Medical University School of Medicine. Morioka, 020 Japan -Received for Publication, October 19, 1992- Key Words: Sternocleidomastoid muscle, Hypoglossal nerve, Superior sternoclavicular muscle (Hyrtl), Dual nerve supply, Gross anatomy Summary: An anomalous nerve supply from the hypoglossal nerve (XII) to the sternocleidomastoid muscle (SM) was observed in the right neck of an 82-year-old Japanese female. This nerve branch arose from the hypoglossal nerve at the origin of the superior root of the ansa cervicalis. The nerve fiber analysis revealed that this branch consisted of fibers from the hypoglossal nerve, the first and the second cervical nerves and had the same component as the superior root of the ansa cervicalis. SM appeared quite normal and the most part was innervated by the accessory nerve and a branch from the cervical plexus. The anomalous branch from XII supplied the small deep area near the anterior margin of the middle of the sternomastoid portion of SM. It is reasonable to think that the small deep area of SM, which was innervated by the anomalous branch from XII, occurs as the result of fusion of the muscular component from infrahyoid muscles. If the muscular component does not fuse with SM, it is thought to appear as an aberrant muscle such as the superior sternoclavicular muscle (Hyrtl) which is also supplied from a branch of the superior root of the ansa cervicalis. -

Transoral Approach to Laser Thyroarytenoid Myoneurectomy for Treatment of Adductor Spasmodic Dysphonia: Short-Term Results
Annals of Oioliigy, Rhinohgy & Laryngology 116(1); 11-1 ©2007 Annals Publishing Company, All righis reserved. Transoral Approach to Laser Thyroarytenoid Myoneurectomy for Treatment of Adductor Spasmodic Dysphonia: Short-Term Results Chih-Ying Su. MD: Hui-Ching Chuang. MD; Shang-Shyue Tsai. PhD: Jeng-FenChiu,PhD Objectives: The surgical technique for the resection of the recurrent larvngeal nerve for adductor spasmodic dysphonia (ASD) ha.s high late failure rates. During the pa.st decade, botulinum toxin has emerged as the treatment of choice for ASD. Although effective, it also has significant disadvantages, including a temporary effect and an unpredictable dose- response relationship. In this study we investigated the effectiveness of a new transoral approach to laser thyroarytenoid mynneurectomy for treatment of ASD. Methods: Fourteen patients with ASD underwent transoral laser myoneurectomy of bilateral thyroarytenoid muscles. Under general anesthesia, an operating miLTOscope and a carbon dioxide laser were used to pertorm myectomy of the mid-posterior belly of bilateral thyroarytenoid muscles together with neurectomy ofthe terminal nerve fibers among the deep muscle bundles. Care was taken not to damage ihe vocal is ligaments, arytenoid cartilages, and lateral cricoarytenoid muscles. Preoperative and postoperative videolaryngostroboscopy and vocal assessments were studied, Results: The 13 patients who completed more than 6 months follow-up were enrolled in this study. Moderate and marked vocal improvement was achieved in 92^;? of the patient.s (12 of 13) after laser surgery during an average tbllow-up period of !7 months (range. 6 to 31 months). No vocaifoldatrophy or paralysis was observed in any patient. None of the patients had a recurrence during the foilow-up period. -

Anatomy Module 3. Muscles. Materials for Colloquium Preparation
Section 3. Muscles 1 Trapezius muscle functions (m. trapezius): brings the scapula to the vertebral column when the scapulae are stable extends the neck, which is the motion of bending the neck straight back work as auxiliary respiratory muscles extends lumbar spine when unilateral contraction - slightly rotates face in the opposite direction 2 Functions of the latissimus dorsi muscle (m. latissimus dorsi): flexes the shoulder extends the shoulder rotates the shoulder inwards (internal rotation) adducts the arm to the body pulls up the body to the arms 3 Levator scapula functions (m. levator scapulae): takes part in breathing when the spine is fixed, levator scapulae elevates the scapula and rotates its inferior angle medially when the shoulder is fixed, levator scapula flexes to the same side the cervical spine rotates the arm inwards rotates the arm outward 4 Minor and major rhomboid muscles function: (mm. rhomboidei major et minor) take part in breathing retract the scapula, pulling it towards the vertebral column, while moving it upward bend the head to the same side as the acting muscle tilt the head in the opposite direction adducts the arm 5 Serratus posterior superior muscle function (m. serratus posterior superior): brings the ribs closer to the scapula lift the arm depresses the arm tilts the spine column to its' side elevates ribs 6 Serratus posterior inferior muscle function (m. serratus posterior inferior): elevates the ribs depresses the ribs lift the shoulder depresses the shoulder tilts the spine column to its' side 7 Latissimus dorsi muscle functions (m. latissimus dorsi): depresses lifted arm takes part in breathing (auxiliary respiratory muscle) flexes the shoulder rotates the arm outward rotates the arm inwards 8 Sources of muscle development are: sclerotome dermatome truncal myotomes gill arches mesenchyme cephalic myotomes 9 Muscle work can be: addacting overcoming ceding restraining deflecting 10 Intrinsic back muscles (autochthonous) are: minor and major rhomboid muscles (mm. -

FIPAT-TA2-Part-2.Pdf
TERMINOLOGIA ANATOMICA Second Edition (2.06) International Anatomical Terminology FIPAT The Federative International Programme for Anatomical Terminology A programme of the International Federation of Associations of Anatomists (IFAA) TA2, PART II Contents: Systemata musculoskeletalia Musculoskeletal systems Caput II: Ossa Chapter 2: Bones Caput III: Juncturae Chapter 3: Joints Caput IV: Systema musculare Chapter 4: Muscular system Bibliographic Reference Citation: FIPAT. Terminologia Anatomica. 2nd ed. FIPAT.library.dal.ca. Federative International Programme for Anatomical Terminology, 2019 Published pending approval by the General Assembly at the next Congress of IFAA (2019) Creative Commons License: The publication of Terminologia Anatomica is under a Creative Commons Attribution-NoDerivatives 4.0 International (CC BY-ND 4.0) license The individual terms in this terminology are within the public domain. Statements about terms being part of this international standard terminology should use the above bibliographic reference to cite this terminology. The unaltered PDF files of this terminology may be freely copied and distributed by users. IFAA member societies are authorized to publish translations of this terminology. Authors of other works that might be considered derivative should write to the Chair of FIPAT for permission to publish a derivative work. Caput II: OSSA Chapter 2: BONES Latin term Latin synonym UK English US English English synonym Other 351 Systemata Musculoskeletal Musculoskeletal musculoskeletalia systems systems -
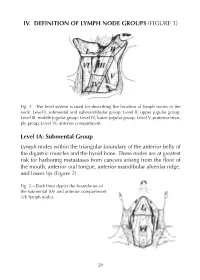
IV. DEFINITION of LYMPH NODE GROUPS (FIGURE 1) Level IA
IV. DEFINITION OF LYMPH NODE GROUPS (FIGURE 1) Fig. 1—The level system is used for describing the location of lymph nodes in the neck: Level I, submental and submandibular group; Level II, upper jugular group; Level III, middle jugular group; Level IV, lower jugular group; Level V, posterior trian - gle group; Level VI, anterior compartment. Level IA: Submental Group Lymph nodes within the triangular boundary of the anterior belly of the digastric muscles and the hyoid bone. These nodes are at greatest risk for harboring metastases from cancers arising from the floor of the mouth, anterior oral tongue, anterior mandibular alveolar ridge, and lower lip (Figure 2). Fig. 2—Dark lines depict the boundaries of the submental (IA) and anterior compartment (VI) lymph nodes. 29 Level IB: Submandibular Group Lymph nodes within the boundaries of the anterior and posterior bel - lies of the digastric muscles, the stylohyoid muscle, and the body of the mandible. Radiographically, the vertical plane at the posterior aspect of the submandibular gland forms a use means of demarcat - ing the posterior aspect of Level IB from IIA.The group includes the pre- and postglandular nodes, and the pre- and postvascular nodes. The submandibular gland is included in the specimen when the lymph nodes within this triangle are removed. These nodes are at greatest risk for harboring metastases from the cancers arising from the oral cavity, anterior nasal cavity, soft tissue structures of the mid - face, and submandibular gland (Figure 3). Fig. 3—The boundaries dividing levels I, II, and V into sublevels A and B. -

Pig Dissection Slides
Contents Pig Dissection •• ContentsContents External Features Sex Determination Mouth and Maxillary Nerve Muscles Index Internal Systems Index External features Contents Answers Sex determination Contents Male Answers Female Male Contents Answers to External anatomy 1. Pinna 2. External auditory meatus 3. Nictitating membrane 4. Rooter 5. Vibrissae 6. Umbilical cord 7. Genital papilla 8. Urogential orifice Sex Determination 9. Scrotum Back to externals 10. Mammary papilla 11. Anus Mouth and Maxillary nerve Contents Answers Contents Answers to Mouth and Facial nerve 1. Hard palate 2. Epiglottis 3. Canine teeth 4. Soft palate 5. Eustachian tube 6. Nasopharynx 7. Oral pharynx 8. Glottis 9. External nostril Mouth and Facial 10. Maxillary nerve 11. Infraorbital foramen 12. Opening to nasopharynx Contents Muscle Index • Neck and shoulder muscles Ventral view neck Lateral view neck Lateral view neck and shoulder Lateral view shoulder and leg muscles Lower limb Lateral view Medial view 1 Medial view 2 Neck and Shoulder Muscles 1 Contents Answers Back to Muscle index Neck and Shoulder Muscles 2 Contents Answers Back to Muscle index Neck and Shoulder Muscles 3 Contents Answers Back to Muscle index Lateral view Shoulder Contents and leg muscles Answers Back to Muscle index Lower limb lateral muscles Contents Answers Back to Muscle index Lower limb medial muscles 1 Contents Answers Back to Muscle index Lower limb medial muscles 2 Contents Answers Back to Muscle index Answers to Muscles Contents Neck and shoulder Lower limb 1. Masseter 18. Biceps femoris muscle 2. Submaxillary gland (Mandibular gland) 19. Tensor fasciae latae 3. Parotid gland 20. Gluteus medius muscle 4. -

Function of the Posterior Cricoarytenoid Muscle in Phonation: in Vivo Laryngeal Model
Function of the posterior cricoarytenoid muscle in phonation: In vivo laryngeal model HONG-SHIK CHOI, MD, GERALD S. BERKE, MD, MING YE, MD, and JODY KREIMAN, PhD, Los Angeles, California The function of the posterior cricoarytenoid (PCA) muscle In phonation has not been well documented. To date, several electromyographlc studies have suggested that the PCA muscle Is not simply an abductor of the vocal folds, but also functions In phonation. This study used an In vivo canine laryngeal model to study the function of the PCA muscle. SUbglottic pressure and electroglottographlc, photoglottographlc, and acoustic waveforms were gathered from fiVe adult mongrel dogs under varying conditions of nerve stimulation. Subglottic pressure. fundamental frequency, sound Intensity, and vocal efficiency decreased with Increasing stimulation of the posterior branch of the recurrent laryngeal nerve. These results suggest that the PCA muscle not only acts to brace the larynx against the anterior pull of the adductor and cricothyroid muscles, but also functions Inhlbltorlly In phonation by controlling the phonatory glottal width. (OTOLARYNGOL HEAD NECK SURG 1993;109: 1043-51.) The important physiologicfunctions of the larynx during phonation in some clinical cases. Kotby and protection of the lower airway, phonation, and res Haugen? also observed increased activity in the 1 piration - are all mediated by the laryngeal mus PCA muscle during phonation and postulated that cles. Intrinsic laryngeal muscles are classified into the muscle is not simply an abductor of the vocal three groups: the tensors, which regulate the length cord. and tension of the vocal folds; the adductors, which Gay et al." observed increased activity in the PCA close the glottis; and the abductor, which opens the muscle during phonation in chest voice at high glottis.