Ma2015-7 Marine Accident Investigation Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Takings Jurisprudence of the Warren Court: a Constitutional Siesta
University of Chicago Law School Chicago Unbound Journal Articles Faculty Scholarship 1996 The Takings Jurisprudence of the Warren Court: A Constitutional Siesta Richard A. Epstein Follow this and additional works at: https://chicagounbound.uchicago.edu/journal_articles Part of the Law Commons Recommended Citation Richard A. Epstein, "The Takings Jurisprudence of the Warren Court: A Constitutional Siesta," 31 Tulsa Law Journal 643 (1996). This Article is brought to you for free and open access by the Faculty Scholarship at Chicago Unbound. It has been accepted for inclusion in Journal Articles by an authorized administrator of Chicago Unbound. For more information, please contact [email protected]. TULSA LAW JOURNAL Volume 31 Summer 1996 Number 4 THE TAKINGS JURISPRUDENCE OF THE WARREN COURT: A CONSTITUTIONAL SIESTA* Richard A. Epsteint I. EBB TIDE FOR PROPERTY RIGHTS ...................... 644 II. A CRITIQUE OF THE WARREN COURT DECISIONS ...... 650 A. The Prima Facie Case: A Taking of Private Property ............................................ 651 1. Water ........................................... 651 2. Overflight Easements ........................... 656 3. Lien Rights ..................................... 658 B. General Regulations................................. 660 1. Prohibition on Use ............................. 660 2. Contract Regulation ............................ 662 3. Rate of Return Regulation ..................... 664 4. Civil Rights Cases .............................. 666 III. POLICE POWER JUSTIFICATIONS -

International MARINE ACCIDENT REPORTING SCHEME
International MARINE ACCIDENT REPORTING SCHEME MARS REPORT No 160 February 2006 MARS 200604 Fall from Gangway 0220 Vessel all fast. Main shore gangway, which could 0900 Stations called fore and aft. Moorings tended and only be moved up-down vertically and not in a made tight as required. Duty officer on poop deck horizontal direction, nor could it be slewed in any for aft stations and Chief Officer on forward other direction, lowered to correct height. stations. No one was paying any particular Connecting gangway (sometimes referred to as attention near the gangway as it was located on an MOT gangway or formerly known as a brow) main deck and out of view from aft stations and was placed on the main gangway. The other end nobody was expected to visit the ship. of the brow was placed on the ship’s rails and 0918 Main engines tried out ahead/astern. made fast there. The ship’s safety net was used 0920 One person from the Seaman’s Club tried to board and a step ladder was made fast to ship’s railings the vessel, in spite of having been warned by the to facilitate the safe access onto the deck. Also a terminal operator (in his native language) against life buoy with a line was placed near the gangway. doing so, and caused the brow to over balance The gangway was manned at all times by a duty and he fell into the water along with the brow. A.B. The Cadet saw this happen from the forecastle deck and raised the alarm. -
Chapter 3 Ship Compartmentation and Watertight Integrity
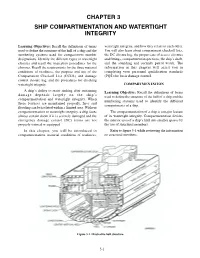
CHAPTER 3 SHIP COMPARTMENTATION AND WATERTIGHT INTEGRITY Learning Objectives: Recall the definitions of terms watertight integrity, and how they relate to each other. used to define the structure of the hull of a ship and the You will also learn about compartment checkoff lists, numbering systems used for compartment number the DC closure log, the proper care of access closures designations. Identify the different types of watertight and fittings, compartment inspections, the ship’s draft, closures and recall the inspection procedures for the and the sounding and security patrol watch. The closures. Recall the requirements for the three material information in this chapter will assist you in conditions of readiness, the purpose and use of the completing your personnel qualification standards Compartment Checkoff List (CCOL) and damage (PQS) for basic damage control. control closure log, and the procedures for checking watertight integrity. COMPARTMENTATION A ship’s ability to resist sinking after sustaining Learning Objective: Recall the definitions of terms damage depends largely on the ship’s used to define the structure of the hull of a ship and the compartmentation and watertight integrity. When numbering systems used to identify the different these features are maintained properly, fires and compartments of a ship. flooding can be isolated within a limited area. Without compartmentation or watertight integrity, a ship faces The compartmentation of a ship is a major feature almost certain doom if it is severely damaged and the of its watertight integrity. Compartmentation divides emergency damage control (DC) teams are not the interior area of a ship’s hull into smaller spaces by properly trained or equipped. -
Sailing Trans-Atlantic on the USCG Barque Eagle
PassageRite of Sailing Trans-Atlantic On The USCG Barque Eagle odern life is complicated. I needed a car, a bus, a train and a taxi to get to my square-rigger. When no cabs could be had, a young police officer offered me a lift. Musing on my last conveyance in such a vehicle, I thought, My, how a touch of gray can change your circumstances. It was May 6, and I had come to New London, Connecticut, to join the Coast Guard training barque Eagle to sail her to Dublin, Ireland. A snotty, wet Measterly met me at the pier, speaking more of March than May. The spires of New Lon- don and the I-95 bridge jutted from the murk, and a portion of a nuclear submarine was discernible across the Thames River at General Dynamics Electric Boat. It was a day for sitting beside a wood stove, not for going to sea, but here I was, and somehow it seemed altogether fitting for going aboard a sailing ship. The next morning was organized chaos. Cadets lugged sea bags aboard. Human chains passed stores across the gangway and down into the deepest recesses of the ship. Station bills were posted and duties disseminated. I met my shipmates in passing and in passageways. Boatswain Aaron Stapleton instructed me in the use of a climbing harness and then escorted me — and the mayor of New London — up the foremast. By completing this evolution, I was qualified in the future to work aloft. Once stowed for sea, all hands mustered amidships. -
NTP 13 (B): Flags, Pennants, & Customs
UNCLASSIFIED NTP 13 (B) NAVAL TELECOMMUNICATIONS PROCEDURES FLAGS, PENNANTS & CUSTOMS NTP 13 (B) NAVAL COMPUTER AND TELECOMMUNICATIONS COMMAND 4401 MASSACHUSETTS AVE., N.W. WASHINGTON, D.C. 20394-5460 DISTRIBUTION AUTHORIZED TO U.S. GOVERNMENT AGENCIES ONLY FOR OPERATIONAL USE (29 August 1986). OTHER REQUESTS FOR THIS DOCUMENT SHALL BE REFERRED TO COMNAVCOMTELCOM. AUGUST 1986 This publication contains U.S. military information and release to other than U.S. military agencies will be on a need-to-know basis. UNCLASSIFIED ORIGINAL (Reverse Blank) NTP-13(B) DEPARTMENT OF THE NAVY NAVAL TELECOMMUNICATIONS COMMAND 440l MASSACHUSETTS AVENUE, N.W. WASHINGTON, D.C. 20394-5460 15 September 1986 LETTER OF PROMULGATION 1. NTP 13(B), FLAGS, PENNANTS AND CUSTOMS, was developed under the direction of the Commander, Naval Telecommunications Command, and is promulgated for use by the U.S. Navy and Coast Guard. 2. NTP 13(B) is an unclassified, non-registered publication. 3. NTP 13(B) is EFFECTIVE UPON RECEIPT and supersedes NTP 13(A). 4. Permission is granted to copy or make extracts from this publication without the consent of the Commander, Naval Telecommunications Command. 5. This publication, or extracts thereof, may be carried in aircraft for use therein. 6. Correspondence concerning this publication should be addressed via the normal military chain of command to the Commander, Naval Telecommunications Command (32), 4401 Massachusetts Avenue, N.W., Washington, D.C. 20394-5460. 7. This publication has been reviewed and approved in accordance with SECNAV Instruction 5600.16. A. F. CAMPBELL Rear Admiral, U.S. Navy Commander, Naval Telecommunications Command ORIGINAL ii NTP-13(B) RECORD OF CHANGES AND CORRECTIONS Enter Change or Correction in Appropriate Column Identification of Change or Correction; Reg. -

The Wire the Complete Guide
The Wire The Complete Guide PDF generated using the open source mwlib toolkit. See http://code.pediapress.com/ for more information. PDF generated at: Tue, 29 Jan 2013 02:03:03 UTC Contents Articles Overview 1 The Wire 1 David Simon 24 Writers and directors 36 Awards and nominations 38 Seasons and episodes 42 List of The Wire episodes 42 Season 1 46 Season 2 54 Season 3 61 Season 4 70 Season 5 79 Characters 86 List of The Wire characters 86 Police 95 Police of The Wire 95 Jimmy McNulty 118 Kima Greggs 124 Bunk Moreland 128 Lester Freamon 131 Herc Hauk 135 Roland Pryzbylewski 138 Ellis Carver 141 Leander Sydnor 145 Beadie Russell 147 Cedric Daniels 150 William Rawls 156 Ervin Burrell 160 Stanislaus Valchek 165 Jay Landsman 168 Law enforcement 172 Law enforcement characters of The Wire 172 Rhonda Pearlman 178 Maurice Levy 181 Street-level characters 184 Street-level characters of The Wire 184 Omar Little 190 Bubbles 196 Dennis "Cutty" Wise 199 Stringer Bell 202 Avon Barksdale 206 Marlo Stanfield 212 Proposition Joe 218 Spiros Vondas 222 The Greek 224 Chris Partlow 226 Snoop (The Wire) 230 Wee-Bey Brice 232 Bodie Broadus 235 Poot Carr 239 D'Angelo Barksdale 242 Cheese Wagstaff 245 Wallace 247 Docks 249 Characters from the docks of The Wire 249 Frank Sobotka 254 Nick Sobotka 256 Ziggy Sobotka 258 Sergei Malatov 261 Politicians 263 Politicians of The Wire 263 Tommy Carcetti 271 Clarence Royce 275 Clay Davis 279 Norman Wilson 282 School 284 School system of The Wire 284 Howard "Bunny" Colvin 290 Michael Lee 293 Duquan "Dukie" Weems 296 Namond Brice 298 Randy Wagstaff 301 Journalists 304 Journalists of The Wire 304 Augustus Haynes 309 Scott Templeton 312 Alma Gutierrez 315 Miscellany 317 And All the Pieces Matter — Five Years of Music from The Wire 317 References Article Sources and Contributors 320 Image Sources, Licenses and Contributors 324 Article Licenses License 325 1 Overview The Wire The Wire Second season intertitle Genre Crime drama Format Serial drama Created by David Simon Starring Dominic West John Doman Idris Elba Frankie Faison Larry Gilliard, Jr. -

Vessel Information Sheet
Note/Reminder: 1. Please refer to the back page for the instructions on how to fill up this form. 2. Put ‘N/A’ in the items that are not applicable to the vessel. 3. VESSEL INFORMATION SHEET Type of Application: New Registration Amendment Classification of Ships by Types: Voyage Type: Foreign Domestic Vessel Type: Vessel Category: Liner Tramping Ferry Bay and River Others Vessel Name: Port of Registry: Expiry Date: Master: License Number: Owner: _________________________________________________ Nationality: _______________ Address: _______________________________________________ Contact Number: ___________ _______________________________________________ Shipping Agent: _________________________________________ Contact Number: ___________ Address: _______________________________________________ _______________________________________________ Conference Name: Charterer Name: Year Built: Call Sign: Gross Tonnage: ____________________ (ton) Stern Length: ______________________ (meter) Net Tonnage: _______________________ (ton) Bow Length: _______________________ (meter) Dead Weight Tonnage: _______________ (ton) Self-sustaining Non Self-sustaining Length Over All: ___________________ (meter) Deck Crane: Yes No Beam: ____________________________ (meter) Swing Boom: Yes No Max. Allowable Draft: _______________ (meter) Heavy Lift Boom: Yes No Other Lifting Equipment: Yes No Hatch Cover Type: _________________ Grain Capacity: ______________________ (ton) No. of Hatches/Holds: _______________ Bales Capacity: ______________________ (ton) Max. Deck -

GENERAL COURTESY DOCK SPECIFICATIONS 1. Scope of Work the Work Covered by This Section Consists of Furnishing All Materials
GENERAL COURTESY DOCK SPECIFICATIONS 1. Scope of Work The work covered by this section consists of furnishing all materials, hardware, gangway, cable connectors for anchorage system, fasteners and other marina hardware necessary to provide the dock system as shown in the plans and specifications. The dock shall be delivered to the site prefabricated as possible with floats attached. Installation of courtesy dock and gangway is not part of this scope of work. 2. WORKMANSHIP AND QUALITY Applicable Standards American Institute of Steel Construction Aluminum Association- Aluminum Design Manuel American Welding Society America Iron and Steel Institute-Light Gauge Cold- Frames Steel Design Manual ASCE Report No. 50 “Small Crafts Harbors”, Third Edition (2012) or Current Edition American Society of Testing Materials Galvanizing Conforms to ASTM A-123 Steel Conforms to ASTM Designation: A-36 A. All finished steel members shall be free from twists, bends, distortions and open joints. All steel construction shall be free of sharp edges and burrs; ends of exposed steel members shall be rounded or beveled. Projecting material and burrs which would prevent bearing of the various members on each other shall be removed. All steel components shall be hot dipped galvanized after fabrication. B. Aluminum extrusions for dock, pier, and gangway structures shall be aluminum alloy 6061-T6 E-channels extruded in accordance with the requirements of applicable sections of Federal Specifications QQ-A-200. Miscellaneous aluminum may be 6063-T5 or 5052-H32. C. All welding shall conform to the requirements of the American Welding Society. Welds shall be a solid and homogenous part of metal joined and shall be free of pits and scale, and shall be full areas and length required to develop the required strength for the intended use. -

LEXIQUE NAUTIQUE ANGLAIS-FRANÇAIS – 2E ÉDITION, NUMÉRIQUE, ÉVOLUTIVE, GRATUITE
Aa LEXIQUE NAUTIQUE ANGLAIS-FRANÇAIS – 2e ÉDITION, NUMÉRIQUE, ÉVOLUTIVE, GRATUITE « DIX MILLE TERMES POUR NAVIGUER EN FRANÇAIS » ■ Dernière mise à jour le 19 octobre 2017 ■ Présenté sur MS Word 2011 pour Mac ■ Taille du fichier 2,3 Mo – Pages : 584 - Notes de bas de page : 51 ■ Ordre de présentation : alphabétique anglais ■ La lecture en mode Page sur deux colonnes est recommandée Mode d’emploi: Cliquer [Ctrl-F] sur PC ou [Cmd-F] sur Mac pour trouver toutes les occurrences d’un terme ou expression en anglais ou en français AVERTISSEMENT AUX LECTEURS Ouvrage destiné aux plaisanciers qui souhaitent naviguer en français chez eux comme à l’étranger, aux instructeurs, modélistes navals et d’arsenal, constructeurs amateurs, traducteurs en herbe, journalistes et adeptes de sports nautiques et lecteurs de revues spécialisées. Il subsiste moult coquilles, doublons et lacunes dont l’auteur s’excuse à l’avance. Des miliers d’ajouts et corrections ont été apportés depuis les années 80 et les entrées sont dorénavant accompagnées d’un ou plusieurs domaines. L’auteur autodidacte n’a pas fait réviser l’ouvrage entier par un traducteur professionnel mais l’apport de généreux plaisanciers, qui ont fait parvenir corrections et suggestions depuis plus de trois décennies contribue à cet ouvrage offert gracieusement dans un but strictement non lucratif, pour usage personnel et libre partage en ligne avec les amoureux de la navigation et de la langue française. Les clubs et écoles de voile sont encouragés à s’en servir, à le diffuser aux membres et aux étudiants. Tous droits réservés de propriété intellectuelle de l’ouvrage dans son ensemble (Copyright 28.10.1980 Ottawa); toutefois la citation de courts extraits est autorisée et encouragée. -

Glossary of Terms
Glossary of Terms Below are new words for our Glossary of Terms based on AB Barlow’s activities the last couple of weeks. To see all the terms from AB Barlow’s past activities, please scroll down. Battle of Cape St. Vincent – one of the first battles of the Anglo-Spanish War (1796-1808). The battle was a decisive English victory and saw four Spanish ships of the line captured by the British; two by Horatio Nelson Battle of Flamborough Head – a battle fought during the American War of Independence during which Captain John Paul Jones captured the British frigate Serapis even as his own ship, Bonhomme Richard, sank out from under him Boarding – the act of sending sailors or soldiers from one’s own ship to an enemy ship for the purpose of capturing the other vessel. In modern context, boarding can also occur for more peaceful purposes such as a safety or customs inspection Brig – a ship with two masts, both carrying square sails. Also, a jail located on board a ship Cutting Out – the act of attacking a ship from small boats filled with sailors or marines. Often used as a surprise tactic Fighting Top – a platform part way up a ship’s mast used as a firing position by sharpshooters during a naval engagement First-Rate – the largest warships in the now-obsolete Royal Navy ranking system. Generally, first-rates mounted around 100 carriage guns Frigate – a small, fast warship; usually built for maneuverability and speed over firepower Gangway – traditionally, a narrow passage connecting a ship’s quarterdeck and forecastle. -

The-Ebb-Tide.Pdf
Produced by Dianne Bean THE EBB-TIDE A TRIO AND QUARTETTE By Robert Louis Stevenson and Lloyde Osbourne 'There is a tide in the affairs of men.' 1 Part I. Chapter 1. NIGHT ON THE BEACH Throughout the island world of the Pacific, scattered men of many European races and from almost every grade of society carry activity and disseminate disease. Some prosper, some vegetate. Some have mounted the steps of thrones and owned islands and navies. Others again must marry for a livelihood; a strapping, merry, chocolate-coloured dame supports them in sheer idleness; and, dressed like natives, but still retaining some foreign element of gait or attitude, still perhaps with some relic (such as a single eye-glass) of the officer and gentleman, they sprawl in palm-leaf verandahs and entertain an island audience with memoirs of the music-hall. And there are still others, less pliable, less capable, less fortunate, perhaps less base, who continue, even in these isles of plenty, to lack bread. At the far end of the town of Papeete, three such men were seated on the beach under a purao tree. It was late. Long ago the band had broken up and marched musically home, a motley troop of men and women, merchant clerks and navy officers, dancing in its wake, arms about waist and crowned with garlands. Long ago darkness and silence had gone from house to house about the tiny pagan city. Only the street lamps shone on, making a glow-worm halo in the umbrageous alleys or drawing a tremulous image on the waters of the 2 port. -

And All the Pieces Matter: Thoughts on the Wire and the Criminal Justice System
And All the Pieces Matter: Thoughts on The Wire and the Criminal Justice System Susan A. Bandes* "Whatever it was, they don't teach it in law school."' I. INTRODUCTION The standard police procedural, even including great dramas like NYPD Blue and Hill Street Blues, adheres to time-honored narrative conventions. It focuses on good, if sometimes imperfect, cops trying to find the real bad guys-the perpetrators-and bring them to justice. The episode begins when a crime ruptures the social fabric, and ends when guilt is determined and things are put to right. The standard procedural is concerned mainly with individual fault and individual heroism. It does not raise disquieting questions about the criminal justice system, the legal system, or the social and political arrangements that lead to a permanent underclass. There are eight million stories in the Naked City,2 and in the police procedural, every one of them stands on its own. This standard cop show narrative reflects and reaffirms a deeply ingrained, reassuring view of the world. The Wire is a different kind of television. It aims not to reassure but to unsettle, or as David Simon once put it, "to pick[] a fight."3 On its surface a police procedural, The Wire has been aptly described as a portrayal of "the social, political, and economic life of an American city with the scope, observational precision, and moral vision of great literature." Unlike the standard police procedural, which presents and resolves a discrete problem every week, The * Distinguished Research Professor, DePaul University College of Law.