International MARINE ACCIDENT REPORTING SCHEME
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Chapter 3 Ship Compartmentation and Watertight Integrity
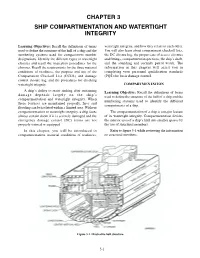
CHAPTER 3 SHIP COMPARTMENTATION AND WATERTIGHT INTEGRITY Learning Objectives: Recall the definitions of terms watertight integrity, and how they relate to each other. used to define the structure of the hull of a ship and the You will also learn about compartment checkoff lists, numbering systems used for compartment number the DC closure log, the proper care of access closures designations. Identify the different types of watertight and fittings, compartment inspections, the ship’s draft, closures and recall the inspection procedures for the and the sounding and security patrol watch. The closures. Recall the requirements for the three material information in this chapter will assist you in conditions of readiness, the purpose and use of the completing your personnel qualification standards Compartment Checkoff List (CCOL) and damage (PQS) for basic damage control. control closure log, and the procedures for checking watertight integrity. COMPARTMENTATION A ship’s ability to resist sinking after sustaining Learning Objective: Recall the definitions of terms damage depends largely on the ship’s used to define the structure of the hull of a ship and the compartmentation and watertight integrity. When numbering systems used to identify the different these features are maintained properly, fires and compartments of a ship. flooding can be isolated within a limited area. Without compartmentation or watertight integrity, a ship faces The compartmentation of a ship is a major feature almost certain doom if it is severely damaged and the of its watertight integrity. Compartmentation divides emergency damage control (DC) teams are not the interior area of a ship’s hull into smaller spaces by properly trained or equipped. -
Sailing Trans-Atlantic on the USCG Barque Eagle
PassageRite of Sailing Trans-Atlantic On The USCG Barque Eagle odern life is complicated. I needed a car, a bus, a train and a taxi to get to my square-rigger. When no cabs could be had, a young police officer offered me a lift. Musing on my last conveyance in such a vehicle, I thought, My, how a touch of gray can change your circumstances. It was May 6, and I had come to New London, Connecticut, to join the Coast Guard training barque Eagle to sail her to Dublin, Ireland. A snotty, wet Measterly met me at the pier, speaking more of March than May. The spires of New Lon- don and the I-95 bridge jutted from the murk, and a portion of a nuclear submarine was discernible across the Thames River at General Dynamics Electric Boat. It was a day for sitting beside a wood stove, not for going to sea, but here I was, and somehow it seemed altogether fitting for going aboard a sailing ship. The next morning was organized chaos. Cadets lugged sea bags aboard. Human chains passed stores across the gangway and down into the deepest recesses of the ship. Station bills were posted and duties disseminated. I met my shipmates in passing and in passageways. Boatswain Aaron Stapleton instructed me in the use of a climbing harness and then escorted me — and the mayor of New London — up the foremast. By completing this evolution, I was qualified in the future to work aloft. Once stowed for sea, all hands mustered amidships. -
NTP 13 (B): Flags, Pennants, & Customs
UNCLASSIFIED NTP 13 (B) NAVAL TELECOMMUNICATIONS PROCEDURES FLAGS, PENNANTS & CUSTOMS NTP 13 (B) NAVAL COMPUTER AND TELECOMMUNICATIONS COMMAND 4401 MASSACHUSETTS AVE., N.W. WASHINGTON, D.C. 20394-5460 DISTRIBUTION AUTHORIZED TO U.S. GOVERNMENT AGENCIES ONLY FOR OPERATIONAL USE (29 August 1986). OTHER REQUESTS FOR THIS DOCUMENT SHALL BE REFERRED TO COMNAVCOMTELCOM. AUGUST 1986 This publication contains U.S. military information and release to other than U.S. military agencies will be on a need-to-know basis. UNCLASSIFIED ORIGINAL (Reverse Blank) NTP-13(B) DEPARTMENT OF THE NAVY NAVAL TELECOMMUNICATIONS COMMAND 440l MASSACHUSETTS AVENUE, N.W. WASHINGTON, D.C. 20394-5460 15 September 1986 LETTER OF PROMULGATION 1. NTP 13(B), FLAGS, PENNANTS AND CUSTOMS, was developed under the direction of the Commander, Naval Telecommunications Command, and is promulgated for use by the U.S. Navy and Coast Guard. 2. NTP 13(B) is an unclassified, non-registered publication. 3. NTP 13(B) is EFFECTIVE UPON RECEIPT and supersedes NTP 13(A). 4. Permission is granted to copy or make extracts from this publication without the consent of the Commander, Naval Telecommunications Command. 5. This publication, or extracts thereof, may be carried in aircraft for use therein. 6. Correspondence concerning this publication should be addressed via the normal military chain of command to the Commander, Naval Telecommunications Command (32), 4401 Massachusetts Avenue, N.W., Washington, D.C. 20394-5460. 7. This publication has been reviewed and approved in accordance with SECNAV Instruction 5600.16. A. F. CAMPBELL Rear Admiral, U.S. Navy Commander, Naval Telecommunications Command ORIGINAL ii NTP-13(B) RECORD OF CHANGES AND CORRECTIONS Enter Change or Correction in Appropriate Column Identification of Change or Correction; Reg. -

Vessel Information Sheet
Note/Reminder: 1. Please refer to the back page for the instructions on how to fill up this form. 2. Put ‘N/A’ in the items that are not applicable to the vessel. 3. VESSEL INFORMATION SHEET Type of Application: New Registration Amendment Classification of Ships by Types: Voyage Type: Foreign Domestic Vessel Type: Vessel Category: Liner Tramping Ferry Bay and River Others Vessel Name: Port of Registry: Expiry Date: Master: License Number: Owner: _________________________________________________ Nationality: _______________ Address: _______________________________________________ Contact Number: ___________ _______________________________________________ Shipping Agent: _________________________________________ Contact Number: ___________ Address: _______________________________________________ _______________________________________________ Conference Name: Charterer Name: Year Built: Call Sign: Gross Tonnage: ____________________ (ton) Stern Length: ______________________ (meter) Net Tonnage: _______________________ (ton) Bow Length: _______________________ (meter) Dead Weight Tonnage: _______________ (ton) Self-sustaining Non Self-sustaining Length Over All: ___________________ (meter) Deck Crane: Yes No Beam: ____________________________ (meter) Swing Boom: Yes No Max. Allowable Draft: _______________ (meter) Heavy Lift Boom: Yes No Other Lifting Equipment: Yes No Hatch Cover Type: _________________ Grain Capacity: ______________________ (ton) No. of Hatches/Holds: _______________ Bales Capacity: ______________________ (ton) Max. Deck -

GENERAL COURTESY DOCK SPECIFICATIONS 1. Scope of Work the Work Covered by This Section Consists of Furnishing All Materials
GENERAL COURTESY DOCK SPECIFICATIONS 1. Scope of Work The work covered by this section consists of furnishing all materials, hardware, gangway, cable connectors for anchorage system, fasteners and other marina hardware necessary to provide the dock system as shown in the plans and specifications. The dock shall be delivered to the site prefabricated as possible with floats attached. Installation of courtesy dock and gangway is not part of this scope of work. 2. WORKMANSHIP AND QUALITY Applicable Standards American Institute of Steel Construction Aluminum Association- Aluminum Design Manuel American Welding Society America Iron and Steel Institute-Light Gauge Cold- Frames Steel Design Manual ASCE Report No. 50 “Small Crafts Harbors”, Third Edition (2012) or Current Edition American Society of Testing Materials Galvanizing Conforms to ASTM A-123 Steel Conforms to ASTM Designation: A-36 A. All finished steel members shall be free from twists, bends, distortions and open joints. All steel construction shall be free of sharp edges and burrs; ends of exposed steel members shall be rounded or beveled. Projecting material and burrs which would prevent bearing of the various members on each other shall be removed. All steel components shall be hot dipped galvanized after fabrication. B. Aluminum extrusions for dock, pier, and gangway structures shall be aluminum alloy 6061-T6 E-channels extruded in accordance with the requirements of applicable sections of Federal Specifications QQ-A-200. Miscellaneous aluminum may be 6063-T5 or 5052-H32. C. All welding shall conform to the requirements of the American Welding Society. Welds shall be a solid and homogenous part of metal joined and shall be free of pits and scale, and shall be full areas and length required to develop the required strength for the intended use. -

LEXIQUE NAUTIQUE ANGLAIS-FRANÇAIS – 2E ÉDITION, NUMÉRIQUE, ÉVOLUTIVE, GRATUITE
Aa LEXIQUE NAUTIQUE ANGLAIS-FRANÇAIS – 2e ÉDITION, NUMÉRIQUE, ÉVOLUTIVE, GRATUITE « DIX MILLE TERMES POUR NAVIGUER EN FRANÇAIS » ■ Dernière mise à jour le 19 octobre 2017 ■ Présenté sur MS Word 2011 pour Mac ■ Taille du fichier 2,3 Mo – Pages : 584 - Notes de bas de page : 51 ■ Ordre de présentation : alphabétique anglais ■ La lecture en mode Page sur deux colonnes est recommandée Mode d’emploi: Cliquer [Ctrl-F] sur PC ou [Cmd-F] sur Mac pour trouver toutes les occurrences d’un terme ou expression en anglais ou en français AVERTISSEMENT AUX LECTEURS Ouvrage destiné aux plaisanciers qui souhaitent naviguer en français chez eux comme à l’étranger, aux instructeurs, modélistes navals et d’arsenal, constructeurs amateurs, traducteurs en herbe, journalistes et adeptes de sports nautiques et lecteurs de revues spécialisées. Il subsiste moult coquilles, doublons et lacunes dont l’auteur s’excuse à l’avance. Des miliers d’ajouts et corrections ont été apportés depuis les années 80 et les entrées sont dorénavant accompagnées d’un ou plusieurs domaines. L’auteur autodidacte n’a pas fait réviser l’ouvrage entier par un traducteur professionnel mais l’apport de généreux plaisanciers, qui ont fait parvenir corrections et suggestions depuis plus de trois décennies contribue à cet ouvrage offert gracieusement dans un but strictement non lucratif, pour usage personnel et libre partage en ligne avec les amoureux de la navigation et de la langue française. Les clubs et écoles de voile sont encouragés à s’en servir, à le diffuser aux membres et aux étudiants. Tous droits réservés de propriété intellectuelle de l’ouvrage dans son ensemble (Copyright 28.10.1980 Ottawa); toutefois la citation de courts extraits est autorisée et encouragée. -

Glossary of Terms
Glossary of Terms Below are new words for our Glossary of Terms based on AB Barlow’s activities the last couple of weeks. To see all the terms from AB Barlow’s past activities, please scroll down. Battle of Cape St. Vincent – one of the first battles of the Anglo-Spanish War (1796-1808). The battle was a decisive English victory and saw four Spanish ships of the line captured by the British; two by Horatio Nelson Battle of Flamborough Head – a battle fought during the American War of Independence during which Captain John Paul Jones captured the British frigate Serapis even as his own ship, Bonhomme Richard, sank out from under him Boarding – the act of sending sailors or soldiers from one’s own ship to an enemy ship for the purpose of capturing the other vessel. In modern context, boarding can also occur for more peaceful purposes such as a safety or customs inspection Brig – a ship with two masts, both carrying square sails. Also, a jail located on board a ship Cutting Out – the act of attacking a ship from small boats filled with sailors or marines. Often used as a surprise tactic Fighting Top – a platform part way up a ship’s mast used as a firing position by sharpshooters during a naval engagement First-Rate – the largest warships in the now-obsolete Royal Navy ranking system. Generally, first-rates mounted around 100 carriage guns Frigate – a small, fast warship; usually built for maneuverability and speed over firepower Gangway – traditionally, a narrow passage connecting a ship’s quarterdeck and forecastle. -

Glossary of Nautical Terms: English – Italian Italian – English
Glossary of Nautical Terms: English – Italian Italian – English 2 Approved and Released by: Dal Bailey, DIR-IdC United States Coast Guard Auxiliary Interpreter Corps http://icdept.cgaux.org/ 6/29/2012 3 Index Glossary of Nautical Terms: English ‐ Italian Italian ‐ English A………………………………………………………...…..page 4 A………………………………………………………..pages 40 ‐ 42 B……………………………………………….……. pages 5 ‐ 6 B……………………………………….……………….pages 43 ‐ 44 C…………………………………………….………...pages 7 ‐ 8 C……………………………………………….……….pages 45 ‐ 47 D……………………………………………………..pages 9 ‐ 10 D………………………………………………………………..page 48 E……………………………………………….…………. page 11 E………………………………….……….…..………….......page 49 F…………………………………….………..……pages 12 ‐ 13 F.………………………………….…………………….pages 50 ‐ 51 G………………………………………………...…………page 14 G…………………………………………………….………….page 52 H………………………………………….………………..page 15 I ………………………………………………………..pages 53 ‐ 54 I………………………………………….……….……... page 16 K………………………………………………..………………page 55 J…………………………….……..……………………... page 17 L…………………………………………………………………page 56 K……………………….…………..………………………page 18 M……………………………………………………….pages 57 ‐ 58 L…………………………………………….……..pages 19 ‐ 20 N……………………………………………….……………….page 59 M…………………………………………………....….. page 21 O……………………………………………………….……….page 60 N…………………………………………………..…….. page 22 P……………………………………….……………….pages 61 ‐ 62 O………………………………………………….…….. page 23 Q…………………………………………………….………….page 63 P………………………............................. pages 24 ‐ 25 R…………………………………………………….….pages 64 ‐ 65 Q…………………………………………….……...…… page 26 S…………………………….……….………………...pages 66 ‐ 68 R…………………………………….…………... pages 27 ‐ 28 -

Wars with the Barbary Powers, Volume VI Part 3
Naval Documents related to the United States Wars with the Barbary Powers Volume VI Part 3 of 4 Naval Operations including diplomatic background from May 1805 through 1807 United States Government Printing Office Washington, 1944 Electronically published by American Naval Records Society Bolton Landing, New York 2011 AS A WORK OF THE UNITED STATES FEDERAL GOVERNMENT THIS PUBLICATION IS IN THE PUBLIC DOMAIN. WARS WITH BARBARY POWERS To Secretary of the Navy from Cap- John Rodgers, U. S. Navy U S SHIPConstitution Syracuse 1 ** Janr 1806 SIB In answer to Duplicate of your letter of the 25'P of June 1805 by the Store Brig Washington permit me to say, that the Marine cloathing, in lieu of that ship'd in the Huntress, has been procured by Cap. Gale, of Marines, agreeabk to your Orders, - But that Gun Boat NP7 has not yet arrived in the Mediter- ranean - at least I have not yet heard of her - therefore !presume that subse- quent to the 25 Q of June you had given orders for her not to proceed - [NDA. Captain's LB, Vol. 1, 1806.1 To Secretary of the Navy from Ceptain John Rodgers, U. S. Bevy U. S. SHIP Comtituiion Syracuse 10,Jan? 1806 SIR The contents of your letter of the 25tb of July, directing that five PI Cent be allow'd, on the am$ of all purchases made by the Navy Agent a[t] Syracuse for the Use of the Squadron, I have made him acquainted of [LC. JRP, L Bk 3,May, 1805-July 1806.1 To Lieutenant David Porter, U. -
Directive 9180.48 April 8, 2009
United States Department of Agriculture Grain Inspection, Packers and Stockyards Administration Federal Grain Inspection Service Directive 9180.48 April 8, 2009 STOWAGE EXAMINATION SERVICES Contents STOWAGE EXAMINATION SERVICES ���������������������������������������������������������������������������������1 1� PURPOSE ����������������������������������������������������������������������������������������������������������������������������2 2� REPLACEMENT HIGHLIGHTS ��������������������������������������������������������������������������������������������2 3� DEFINITION �������������������������������������������������������������������������������������������������������������������������2 4� POLICY ��������������������������������������������������������������������������������������������������������������������������������2 5� RESPONSIBILITIES�������������������������������������������������������������������������������������������������������������5 6� SAFETY ��������������������������������������������������������������������������������������������������������������������������������6 7� STANDARDS OF FITNESS �����������������������������������������������������������������������������������������������12 8� APPLICATION, WORK RECORDS, AND CERTIFICATES ������������������������������������������������14 9� PROCEDURES ������������������������������������������������������������������������������������������������������������������16 Attachment �����������������������������������������������������������������������������������������������������������������������������24 -

Guide for Certification of Offshore Access Gangways 2016
Guide for Certification of Offshore Access Gangways GUIDE FOR CERTIFICATION OF OFFSHORE ACCESS GANGWAYS AUGUST 2016 American Bureau of Shipping Incorporated by Act of Legislature of the State of New York 1862 2016 American Bureau of Shipping. All rights reserved. ABS Plaza 16855 Northchase Drive Houston, TX 77060 USA Foreword Foreword As the demand for a safe and efficient walk to work (W2W) approach prevails in the offshore oil and gas industry, it is envisaged that there will be a significant growth in the use of offshore access gangway systems for the manning and transfer of personnel to and from offshore facilities. Noting the special design and operational characteristics of offshore access gangway systems, ABS has developed this Guide to provide provisions for the certification of offshore access gangway systems used for connecting two offshore units to transfer offshore personnel on a temporary basis. The requirements contained within this Guide included either via direct inclusion or a reference to other ABS Rules or Guides as well as relevant recognized international Regulations in existence prior to the issuance of this Guide. This Guide references relevant international statutory Regulations and guidelines that are considered to be applicable. While it is the intent of the Guide to be consistent with these Regulations and guidelines, it is the ultimate responsibility of the users of this Guide to refer to the most recent text of those Regulations and guidelines. This Guide is to be used in conjunction with other Rules published by ABS and the recognized international Regulations. This Guide is for the use of designers, builders, owners and operators of offshore access gangway systems. -

White Book Safety Regulations
International Longshore & Warehouse Union Canada B.C. Maritime Employers Association Safety Regulations Governing Vessels at British Columbia Ports As approved by Joint Industry Labour Relations Committee on March 21, 1997 These Safety Regulations shall apply in addition to all requirements of The Canada Shipping Act and the applicable Tackle Regulations. Section 1 - Duties and Responsibilities Section 2 - Rules Re Vessels' and Stevedoring Companies' Gear and Equipment and its Usage Section 3 - Rules Re Cargo Handling and Stowage Section 4 - General Safety Rules Section 1 - Duties and Responsibilities Index Rule 1 SECTION 1 DUTIES AND RESPONSIBILITIES Vessel Stevedoring Companies Stevedoring Superintendent and Foreman Foreman Hatchtender Winchdriver and/or Crane Driver Ship Gantry Crane Driver Side Runner Employees First Aid Attendant GENERAL Reporting Defects Reporting Injuries ____________________________________ THINK AND PRACTICE SAFETY These Safety Regulations have been prepared to govern Waterfront Operations at British Columbia Ports. All those engaged in Stevedoring and/or Dock work shall thoroughly familiarize themselves with ALL the Rules and Regulations contained herein. Co-operation is recognized by the BCMEA and the ILWU - Canadian Area as a key element in all accident prevention activity and the parties are committed to work together to ensure that hazards are identified and controlled, to promote safe working conditions, safe work practices and positive attitudes toward health and safety on the job. SAFETY REGULATIONS RULE 1. These regulations are to provide requirements for safety of life, limb and health. In case of practical difficulty or unnecessary hardship an employer or vessel may make exceptions from the literal requirements of this Code and permit the use of other devices or methods but ONLY when it is clearly evident that equivalent protection, as mutually agreed by the Parties, is provided.