Corrected Proof
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Public Expenditure Review of the WASH Sector in Malawi
PUBLIC EXPENDITURE REVIEW OF THE Water, Sanitation, and Hygiene Sector of Malawi February 2020 WATER, SANITATION AND HYGIENE SECTOR MALAWI FEBRUARY 2020 i PUBLIC EXPENDITURE REVIEW © UNICEF/2016/Sebastian Rich © UNICEF/2016/Sebastian ACKNOWLEDGEMENTS Appreciation goes to all individuals and institutions that Muchabaiwa, Patrick Okuni, Nkandu David Chilombo, Alessandro contributed to the development of this PER. The Government Ramella Pezza, Kelvin Tapiwa Mutambirwa and Chimwemwe would like to thank staff from several Ministries, Departments Nyimba for the technical and logistical support. and Agencies (MDAs) who were involved in this PER. Specifically, appreciation goes to staff from the M&E Division under the The Government would also like to deeply thank the Oxford Economic Planning and Development (EP&D) of the Ministry of Policy Management (OPM) consultancy team – comprising of Finance; the Water Supplies Department under the Ministry of Nick Hall (team leader), Zach White (project manager), Tuntufye Agriculture, Irrigation and Water Development (MoAIWD); and Mwalyambwire, and Tim Cammack for providing technical the Environmental Health Department under the Ministry of support that enabled the production of this PER. Also the OPM Health and Population (MoHP). staff that worked in the background to make this exercise a success are appreciated. Sincere gratitude goes to the following Government staff – Sophie Kang’oma, Victoria Geresomo, Richard Jack Kajombo, Gringoster The analysis in this PER draws on scores of interviews with Kajomba and Stevier Kaiyatsa from the EP&D; Emma Mbalame, district staff, with a list of those interviewed or consulted Bibo Charles Yatina and Gertrude Makuti Botomani from the provided in Annex I. The Government is extremely thankful to all MoAIWD; Allone Ganizani, Holystone Kafanikhale, Samuel district for their inputs. -

Chapter 7 Solar Power Generation Planning
CHAPTER 7 SOLAR POWER GENERATION PLANNING Chapter 7 Solar Power Generation Planning The electrification method based on the extension of distribution lines is known as on-grid electrification, while the method that utilizes photovoltaic solar power is known as off-grid electrification. In this chapter, results of the survey on the status of electrification by photovoltaic solar power in Malawi and the state of implementation of photovoltaic power projects funded by foreign countries are discussed. 7.1 The state of Solar Power in Malawi At present photovoltaic energy systems are used in Malawi in many rural sites far from the distribution line. PV residential systems are mostly owned by tobacco farmers, and PV systems for public facilities can be found at many hospitals, post offices, telephone exchange offices, etc. Photovoltaic energy in Malawi has enough potential for development with regard to environmental issues and also reflects a satisfactory degree of established technology. If the problem of the expense of photovoltaic could be solved, it is expected that this technology would spread throughout Malawi and contribute to overall electrification. Some specific knowledge is required to maintain PV systems although not as much as other systems. Furthermore, PV systems can generate electricity whenever solar irradiation is available. Most PV systems in Malawi are Solar Home Systems (SHS) as stand-alone type, being installed in areas far from the grid and where electricity generation by other methods (for example mini hydro) is not possible. There are also systems that are only installed temporarily until other electrification methods become available. The main components of a SHS are the Solar Panel, Battery and Battery Charge Controller (Fig. -

Malawi Coverage Survey 2017
Malawi Coverage Survey 2017 Measuring treatment coverage for schistosomiasis and soil transmitted helminths with preventive chemotherapy 1 Contents Contents .................................................................................................................................................. 2 Introduction ............................................................................................................................................ 4 Background to the Coverage Survey ....................................................................................................... 4 Schistosomiasis and STH in Malawi .................................................................................................... 5 Previous mapping ............................................................................................................................... 5 Treatment History ............................................................................................................................... 5 Previous Coverage Surveys ................................................................................................................. 6 2012 ................................................................................................................................................ 6 2014 ................................................................................................................................................ 6 2016 ............................................................................................................................................... -

Emergency Appeal 2020
EMERGENCY May - October APPEAL 2020 MALAWI MALAWI Overview Map Chitipa CHITIPA Chitipa v" District Hospital Karonga District Hospital v"v"Karonga old Hospital KARONGA Chilumba TANZANIA RUMPHI Rumphi Rumphi District v"Hospital ZAMBIA NORTHERN MZUZU CITY v" Mzuzu Mzuzu Central Hospital v" Nkhata Bay District Hospital NKHATA BAY MZIMBA Mzimba District v" Hospital LIKOMA LILONGWE CITY Lake Malawi MOZAMBIQUE Lilongwe Central Hospital "v KASUNGU \! NKHOTAKOTA "v v" Nkhotakota Bwaila/Bottom Hospital Kasungu District Hospital Kasungu v" District Hospital NTCHISI Ntchisi District ZOMBA CITY CENTRAL v"Hospital DOWA Dzaleka Refugee MCHINJI SALIMA Camp (44,385) v" Dowa District Hospital v"Salima District v" Mchinji District Hospital Hospital ZOMBA LILONGWE CITY v" \!v" DEDZA "v Zomba Central Hospital LILONGWE Dedza Dedza District v" Mangoche BLANTYRE CITY Hospital v" Mangochi District "v MANGOCHI Hospital NTCHEU Ntcheu Ntcheu District Hospitalv" !\ Capi Balaka District Hospital MACHINGA v" Liwonde Majo own BLANTYRE BALAKA v"Machinga District Hospital He ility "v Machinga Lake Centr ospital LIMBE "v Queen Elizabeth Chilwa ZOMBA CITY Central Hospital NENO "v Distr ospital v"Zomba Central Hospital Mwanza District Hospital SOUTHERN Refugee " ZOMBA (Numbe efugees) v BLANTYRE PHALOMBE v"Chiradzulu District Hospital MWANZA Road v" CHIRADZULU BLANTYRE CITY Ional der MULANJE Chikwawa District v" Thyolo District v" Mulanje District Region Hospital Hospital v" Hospital District CHIKWAWA THYOLO MOZAMBIQUE Popul en (People m) Bangula NSANJE ZIMBABWE Nsanje District v" Hospital The designations employed and the presentation of material in the report do not imply the expression of any opinion whatsoever on the part of the Secretariat of the United Nations concerning the legal status of any country, territory, city or area or Theof itdesignationss authorities, or conc eemployedrning the delim iandtation othef its fpresentationrontiers or boundarie sof. -

MALAWI Main Health Facilities and Population Density March 2020
MALAWI Main Health Facilities and Population Density March 2020 Chitipa Chitipa District CHITIPA Hospital Karonga District Karonga old Hospital Hospital KARONGA Chilumba UNITED REPUBLIC OF TANZANIA RUMPHI Rumphi Rumphi District Hospital ZAMBIA NORTHERN MZUZU CITY Mzuzu Central MZUZU Hospital Nkhata Bay NKHATA BAY Nkhata Bay MZIMBA District Hospital Mzimba District Hospital LIKOMA LILONGWE CITY Lake Malawi MOZAMBIQUE Lilongwe Central Hospital Bwaila/Bottom Hospital NKHOTAKOTA KASUNGU Nkhotakota District Hospital Kasungu Kasungu District Hospital NTCHISI ZOMBA CITY Ntchisi District CENTRAL Hospital DOWA Dzaleka Refugee Camp (44,385) MCHINJI Dowa SALIMA Dowa District Salima District Mchinji District Hospital Hospital ZOMBA Hospital LILONGWE CITY ZOMBA CITY Zomba Central Hospital DEDZA LILONGWE Dedza Dedza District BLANTYRE CITY Hospital Mangoche Mangochi District ZOMBA MANGOCHI Hospital NTCHEU Ntcheu Ntcheu District Hospital BLANTYRE CITY Capital City MACHINGA CHIRADZULU Balaka District Liwonde BLANTYRE Queen Elizabeth Central Hospital Hospital Major town MOZAMBIQUE Machinga District Hospital BALAKA Refugee camp / settlement Machinga LIMBE Lake (Number of refugees) ZOMBA CITY Chilwa NENO Road Zomba Central Hospital Mwanza District Hospital SOUTHERN ZOMBA District BLANTYRE PHALOMBE THYOLO BLANTYRE Region MWANZA Chiradzulu District Hospital CHIRADZULU International border BLANTYRE CITY MULANJE Chikwawa District Health facility Hospital Thyolo District Mulanje District Hospital Hospital Central Hospital District Hospital CHIKWAWA THYOLO Population density (People per Sq. Km) < 100 Bangula 101 - 250 NSANJE 251 - 500 ZIMBABWE Nsanje District Hospital 501 - 1,000 > 1,000 The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations. Creation date: 3 Apr 2020 Sources: OSM, UNCS, UNOCHA, Camps: UNHCR, Health Facilities: HDX/WHO-CDC, Population Density: Malawi NSO Feedback: [email protected] | Twitter: @UNOCHA_ROSEA | www.unocha.org/rosea | www.reliefweb.int. -

Geographic Accessibility Analysis for Emergency Obstetric Care Services in Malawi
Investing the Marginal Dollar for Maternal and Newborn Health: Geographic Accessibility Analysis for Emergency Obstetric Care services in Malawi Steeve Ebener, PhD 1 and Karin Stenberg, MSc 2 1 Consultant, Gaia GeoSystems, The Philippines 2 Technical Officer, Department of Health Systems Governance and Financing, World Health Organization, Geneva, Switzerland Geographic Accessibility Analysis for Emergency Obstetric Care services in Malawi © World Health Organization 2016 All rights reserved. Publications of the World Health Organization are available on the WHO website (http://www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; email: [email protected]). Requests for permission to reproduce or translate WHO publications –whether for sale or for non-commercial distribution– should be addressed to WHO Press through the WHO website (http://www.who.int/about/licensing/copyright_form/index.html). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. -

Study on Violence Against Children in Malawi
Government of Malawi Ministry of Gender, Child Welfare and Community Services Study on Violence Against Children in Malawi A Report prepared by: Government of Malawi Submitted to: The United Nations, Geneva. Switzerland. UNICEF LILONGWE MALAWI April 2005 TABLE OF CONTENTS LIST OF ACRONYMS. IV ACKNOWLEDGEMENT V 1.0 INTRODUCTION 7 1.1 THE STUDY ON VIOLENCE AGAINST CHILDREN 8 1.2 METHODOLOGY 8 1.3 LIMITATIONS OF THE STUDY 8 2. LEGAL FRAMEWORK 10 2.1 INTERNATIONAL HUMAN RIGHTS INSTRUMENTS 10 2.2 LEGAL PROVISIONS ON VIOLENCE AGAINST CHILDREN 10 2.2.1 MALAWI’S CONSTITUTION, LEGISLATION AND SUBSIDIARY LEGISLATION 10 2.2.2 CUSTOMARY LAW ON VIOLENCE AGAINST CHILDREN 11 2.2.3 SOME SPECIFIC LEGISLATIVE PROVISIONS DEALING WITH VIOLENCE AGAINST CHILDREN 12 2.2.4 COURTS TASKED WITH ADDRESSING VIOLENCE AGAINST CHILDREN. 13 2.2.5 MINIMUM AGE FOR SEXUAL ACTIVITY AND SEXUAL EXPLOITATION OF CHILDREN 13 2.2.6 COMPLAINTS PROCEDURES INCLUDING REPORTING OBLIGATIONS RELATING TO VIOLENCE AGAINST CHILDREN 15 2.2.7 JUVENILE JUSTICE ADMINISTRATION 16 2.2.8 OTHER ISSUES RELATING TO COMPLAINTS PROCEDURES 16 3.0 INSTITUTIONAL FRAMEWORK AND RESOURCES TO ADDRESS VAC 18 3.1 THE MINISTRY OF GENDER, CHILD WELFARE AND COMMUNITY SERVICES: 18 3.1.1 FOSTER PLACEMENT SERVICES 18 3.1.2 ADOPTION SERVICES 18 3.1.3 PUBLIC ASSISTANCE 18 3.1.4 INSTITUTIONAL CARE 19 3.2 OTHER GOVERNMENT MINISTRIES DEALING WITH VAC 19 3.3 COORDINATION OF WORK ON VIOLENCE AGAINST CHILDREN COORDINATED BY THE MINISTRY OF GENDER, CHILD WELFARE AND COMMUNITY SERVICES 21 3.2.1 JOINT COORDINATION COMMITTEE -
Malawi Situation Report No.4 Feb03
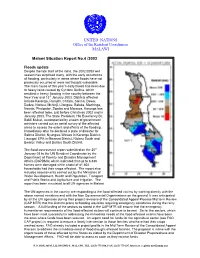
UNITED NATIONS Office of the Resident Coordinator MALAWI Malawi Situation Report No.4 /2003 Floods update Despite the late start of the rains, the 2002/2003 wet season has surprised many, with the early occurrence of flooding, particularly in areas where floods have not previously occurred or were not thought vulnerable. The main cause of this year’s early floods has been due to heavy rains caused by Cyclone Delfina, which resulted in heavy flooding in the country between the New Year and 13th January 2003. Districts affected include Karonga, Rumphi, Chitipa, Salima, Dowa, Dedza, Ntcheu, Mchinji, Lilongwe, Balaka, Machinga, Nsanje, Phalombe, Zomba and Mwanza. Karonga has been affected twice, just before Christmas 2002 and in January 2003. The State President, His Excellency Dr. Bakili Muluzi, accompanied by a team of government ministers carried out an aerial survey of the affected areas to assess the extent and effects of the flooding. Immediately after he declared a state of disaster for Salima District; Nyungwe-Wovwe in Karonga District; Lisungwi EPA in Mwanza District; Ntcheu South and Bwanje Valley and Balaka South District. The flood assessment report submitted on the 25th January 03 to the UN Resident Coordinator by the Department of Poverty and Disaster Management Affairs (DoPDMA) which indicated that up to 6,838 homes were damaged while a total of 81,604 households had their crops affected. The report also includes assessments carried out by the Ministries of Water Development, Health and Population, Transport and Public Works and Agriculture and Irrigation. The report has been circulated to all UN agencies in Malawi. -

1 Introduction to the Karonga DSS Site (Karonga Continuous Registration System, CRS)
1 Introduction to the Karonga DSS Site (Karonga Continuous Registration System, CRS) The Karonga programme began in 1978 with support from the British Leprosy Relief Association (LEPRA), as a population laboratory for evaluation of tools developed by the IMMLEP (Immunology of Leprosy) component of the WHO/TDR programme (the first skin and serological tests for M. leprae infection and an M. leprae antigen-based vaccine). It was designed initially as a large cohort study for risk factors of leprosy infection and disease, covering the entire district of Karonga (the population was selected because it had the highest burden of leprosy in that part of Africa). It assumed responsibility for tuberculosis diagnosis and treatment in the district in 1984, became the largest vaccine trial ever carried out in Africa in 1986 (comparing one versus two doses of BCG versus a combined BCG plus killed M. leprae vaccine, against both leprosy and tuberculosis) and began studies of HIV in 1987 (since which date an effort has been made to HIV test all leprosy and tuberculosis cases, and appropriate controls). The combined epidemiological and vaccine trial activities became known as the Karonga Prevention Study (KPS), by which name the project is still known. The trial codes were broken in 1995, revealing that BCG had provided appreciable protection against leprosy (50 % one dose; 75 % two doses) but none against tuberculosis.1 The trial results raised a variety of scientific questions, which, in combination with a unique sample archive and body of knowledge about the population, led to two Wellcome Trust supported programmes, first from 01/09/96 to 31/08/01 and the second (current) from 01/09/01 to 31/08/05. -

A Planning Survey of the Northern Region, Malawi
A PLANNING SURVEY OF THE NORTHERN REGION, MALAWI Leo de Haan Jan de Jong Jan Sterkenburg Department of Geography of Developing Countries University of Utrecht, The Netherlands February, 1975 INTRODUCTION This regional planning survey of the Northern Region has been written at the request of the Town Planning Department of the Ministry of Works and Supplies. Initially, it was intended to restrict the sur- vey to the physical aspects of planning, the aspects of settlements, services, service centres and infrastructure in particular. Under an agreement between the Town Planning Department and the University of Utrecht, the authors were assigned the task of surveying the existing pattern of resources of the Northern Region of Malawi with a view to making recommendations for the improved Organisation of physical de- velopment through plans and policies aimed at securing greater co- ordination of development effort, at strengthening and relationalizing infrastructural services, at identifying rural-urban relationships and generally at providing a basic framework for integral planning of the region's land uses. Regional physical planning is, however, closely related to the economie and social development of an area. For the Northern Region agriculture is the basis of the economy and the source of employment for more than 90 % of its population. Consequently, aspects of physi- cal planning cannot be dealt with without paying adequate attention to the agricultural sector, the existing constraints for raising productivity and the attempts of the Malawi government to improve this sector. An expanding agricultural sector earns foreign exchange, provides food for the non-agricultural population, and may increase rural incomes and provide a growing market for manufactured products. -

Languages and Area Spoken for Chitipa
LANGUAGE MAPPING SURVEY FOR NORTHERN MALAWI UNIVERSITY OF MALAWI CENTRE FOR LANGUAGE STUDIES PO BOX 108 ZOMBA MALAWI TEL: +265 01527460 FAX: +265 01525587 EMAIL:[email protected] A REPORT SUBMITTED TO September, 2006 1 Table of Contents Acknowledgements .............................................................................................................. 4 1.1 INTRODUCTION ......................................................................................................... 5 1.2 Objectives ..................................................................................................................... 5 1.3 Methodology .................................................................................................................. 6 1.4 Research Team ............................................................................................................... 6 1.5 Instruments ..................................................................................................................... 7 1.5.1 Individual Questionnaires ....................................................................................... 7 1.5.2 Focused Group Discussions .................................................................................... 7 1.5.3 Key Informant Interviews (KIIs) ............................................................................ 8 1.5.4 Geographical positioning system (GPS) ................................................................. 8 1.6 Demographic Characteristics of Research Sample ....................................................... -

Region District Testing Sites Southern Region Blantyre Blantyre Dream
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any reliance Supplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health Table of COVID-19 Laboratory Testing Sites in Malawi on 31st August 2020 Region District Testing Sites Southern Region Blantyre Blantyre Dream Blantyre Light House College of Medicine Malamulo Adventist Malawi Liverpool Wellcome Trust Queen Elizabeth Central Hospital Mwanza Mwanza District Hospital Mangochi Mangochi District Hospital Zomba Zomba Central Hospital Balaka Balaka Dream Balaka District Hospital Thyolo Thyolo District Hospital Neno Neno District Hospital Phalombe Phalombe District Hospital Chiradzulu Chiradzulu District Hospital Mulanje Mulanje District Hospital Chikwawa Chikwawa District Hospital Nsanje Nsanje District Hospital Machinga Machinga District Hospital Central Region Lilongwe Bwaila Hospital Kamuzu Central Hospital Kamuzu Barracks Lilongwe Light House Partners in Health UNC Project Lilongwe Salima Salima District Hospital Mchinji Mchinji District Hospital Dowa Dowa District Hospital Kasungu Kasungu District Hospital Nkhotakota Nkhotakota District Hospital Dedza Dedza District Hospital Nkhoma Mission Ntcheu Ntcheu District Hospital Ntchisi Ntchisi District Hospital Northern Region Mzimba Mzuzu Central Hospital Mzimba South District Hospital Wezi Medical Centre Nkhata Bay Nkhata Bay District Hospital Karonga Karonga District Hospital Karonga MEIRU Chitipa Chitipa District Hospital Likoma Likoma Rumphi Rumphi District Hospital MEIRU: Malawi Epidemiology and Intervention Research Unit Mzumara GW, et al. BMJ Global Health 2021; 6:e006035. doi: 10.1136/bmjgh-2021-006035.