Malawi Operational Plan COP16 Strategic Direction Summary
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Rp13110rp0v10p06b0afr0rp
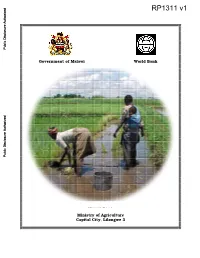
Public Disclosure Authorized Government of Malawi World Bank Irrigation, Rural Livelihoods and Agriculture Development Project Public Disclosure Authorized Public Disclosure Authorized Resettlement Policy Framework Volume 1: Social Impact Assessment Final Report March 2005 Public Disclosure Authorized Ministry of Agriculture Capital City, Lilongwe 3 Irrigation, Rural Livelihoods and Agriculture Development Project Resettlement Policy Framework Volume 1: Social Impact Assessment Final Report Proponent: The Principal Secretary Ministry of Agriculture P.O. Box 30134 Capital City Lilongwe 3 Tel: (265) 1789033 (265) 1789252 Fax: (265) 1789218 (265) 1788738 Consultant: Kempton Consultancy Services Plot No. 4/354D Shire Limited Building P.O. Box 1048 Lilongwe. Malawi. Mobile: (265) 9958136 ii Table of Contents Table of Contents----------------------------------------------------------------------------------------------------------------- iii EXECUTIVE SUMMARY------------------------------------------------------------------------------------------------------- vi ACKNOWLEDGEMENTS ---------------------------------------------------------------------------------------------------- x LIST OF ACRONYMS ----------------------------------------------------------------------------------------------------------xi LIST OF TABLES ---------------------------------------------------------------------------------------------------------------xii 1.0 Introduction ------------------------------------------------------------------------------------------------------------- -

Malawi 2018-19 Draft Financial Statement
Budget Document No. 3 Government of Malawi DRAFT 2018/19 FINANCIAL STATEMENT Ministry of Finance, Economic Planning and Development P.O. Box 30049 Lilongwe ii 2018-19 Financial Statement DRAFT 2018/19 FINANCIAL STATEMENT iii 2018-19 Financial Statement iv 2018-19 Financial Statement Table of Contents Abbreviations and Acronyms .......................................................................................................................... viii 1. INTRODUCTION .......................................................................................................................................... 9 2. THE 2016/17 FISCAL YEAR PERFORMANCE.............................................................................................. 10 2.1 Revenue and Grants ......................................................................................................................... 12 2.1.1 Domestic Revenue ................................................................................................................... 12 2.1.2 Grants ....................................................................................................................................... 13 2.2 Expenditure and Net Lending .......................................................................................................... 14 2.2.1 Recurrent Expenditure ............................................................................................................. 15 2.2.2 Development Expenditures ..................................................................................................... -

Public Expenditure Review of the WASH Sector in Malawi
PUBLIC EXPENDITURE REVIEW OF THE Water, Sanitation, and Hygiene Sector of Malawi February 2020 WATER, SANITATION AND HYGIENE SECTOR MALAWI FEBRUARY 2020 i PUBLIC EXPENDITURE REVIEW © UNICEF/2016/Sebastian Rich © UNICEF/2016/Sebastian ACKNOWLEDGEMENTS Appreciation goes to all individuals and institutions that Muchabaiwa, Patrick Okuni, Nkandu David Chilombo, Alessandro contributed to the development of this PER. The Government Ramella Pezza, Kelvin Tapiwa Mutambirwa and Chimwemwe would like to thank staff from several Ministries, Departments Nyimba for the technical and logistical support. and Agencies (MDAs) who were involved in this PER. Specifically, appreciation goes to staff from the M&E Division under the The Government would also like to deeply thank the Oxford Economic Planning and Development (EP&D) of the Ministry of Policy Management (OPM) consultancy team – comprising of Finance; the Water Supplies Department under the Ministry of Nick Hall (team leader), Zach White (project manager), Tuntufye Agriculture, Irrigation and Water Development (MoAIWD); and Mwalyambwire, and Tim Cammack for providing technical the Environmental Health Department under the Ministry of support that enabled the production of this PER. Also the OPM Health and Population (MoHP). staff that worked in the background to make this exercise a success are appreciated. Sincere gratitude goes to the following Government staff – Sophie Kang’oma, Victoria Geresomo, Richard Jack Kajombo, Gringoster The analysis in this PER draws on scores of interviews with Kajomba and Stevier Kaiyatsa from the EP&D; Emma Mbalame, district staff, with a list of those interviewed or consulted Bibo Charles Yatina and Gertrude Makuti Botomani from the provided in Annex I. The Government is extremely thankful to all MoAIWD; Allone Ganizani, Holystone Kafanikhale, Samuel district for their inputs. -
The Local Governance Performance Index (LGPI) in Malawi: Selected Findings on Health
The Program on Governance and Local Development The Local Governance Performance Index (LGPI) in Malawi: Selected Findings on Health Report November 2016 SERIES 2016:7 Acknowledgements This project reflects fruitful collaboration of researchers at the Christian Michelson Institute, including Ragnhild Muriaas, Lise Rakner and Vibeke Wang; the Institute for Public Opinion and Research, including Asiyati Chiweza, Boniface Dulani, Happy Kayuni, Hannah Swila and Atusaye Zgambo; and the Program on Governance and Local Development, including Adam Harris, Kristen Kao, Ellen Lust, Maria Thorson, Jens Ewald, Petter Holmgren, Pierre Landry and Lindsay Benstead during implementation, and in addition Ruth Carlitz, Sebastian Nickel, Benjamin Akinyemi, Laura Lungu and Tove Wikehult in the process of data cleaning and analysis. We gratefully recognize the hard work of colleagues at the Institute for Public Opinion and Research who lead the survey research teams. These include, Ellasy Chimimba, Grace Gundula, Steve Liwera, Shonduri Manda, Alfred Mangani, Razak Mussa, Bernard Nyirenda, Charles Sisya and Elizabeth Tizola. We also thank Jane Steinberg, who provided excellent and timely editing of this report. Finally, we reserve special recognition for Laura Lungu and Kristen Kao, who led this report. This project has been made possible with the financial support of the Moulay Hicham Foundation, the Carnegie Corporation of New York, The World Bank and Yale University, which funded development of the Local Governance Performance Index, and the Swedish Research Council and the Research Council of Norway, which funded implementation in Norway. We are grateful for their support. Executive Summary Malawi is one of the poorest countries in the world. Gross national income per capita is just $747 U.S.,1 and nearly 51 percent of the population resides below the national poverty line.2 As such, much of the population suffers from health ailments. -

Map District Site Balaka Balaka District Hospital Balaka Balaka Opd
Map District Site Balaka Balaka District Hospital Balaka Balaka Opd Health Centre Balaka Chiendausiku Health Centre Balaka Kalembo Health Centre Balaka Kankao Health Centre Balaka Kwitanda Health Centre Balaka Mbera Health Centre Balaka Namanolo Health Centre Balaka Namdumbo Health Centre Balaka Phalula Health Centre Balaka Phimbi Health Centre Balaka Utale 1 Health Centre Balaka Utale 2 Health Centre Blantyre Bangwe Health Centre Blantyre Blantyre Adventist Hospital Blantyre Blantyre City Assembly Clinic Blantyre Chavala Health Centre Blantyre Chichiri Prison Clinic Blantyre Chikowa Health Centre Blantyre Chileka Health Centre Blantyre Blantyre Chilomoni Health Centre Blantyre Chimembe Health Centre Blantyre Chirimba Health Centre Blantyre Dziwe Health Centre Blantyre Kadidi Health Centre Blantyre Limbe Health Centre Blantyre Lirangwe Health Centre Blantyre Lundu Health Centre Blantyre Macro Blantyre Blantyre Madziabango Health Centre Blantyre Makata Health Centre Lunzu Blantyre Makhetha Clinic Blantyre Masm Medi Clinic Limbe Blantyre Mdeka Health Centre Blantyre Mlambe Mission Hospital Blantyre Mpemba Health Centre Blantyre Ndirande Health Centre Blantyre Queen Elizabeth Central Hospital Blantyre South Lunzu Health Centre Blantyre Zingwangwa Health Centre Chikwawa Chapananga Health Centre Chikwawa Chikwawa District Hospital Chikwawa Chipwaila Health Centre Chikwawa Dolo Health Centre Chikwawa Kakoma Health Centre Map District Site Chikwawa Kalulu Health Centre, Chikwawa Chikwawa Makhwira Health Centre Chikwawa Mapelera Health Centre -

Master Plan Study on Rural Electrification in Malawi Final Report
No. JAPAN INTERNATIONAL COOPERATION AGENCY (JICA) MINISTRY OF NATURAL RESOURCES AND ENVIRONMENTAL AFFAIRS (MONREA) DEPARTMENT OF ENERGY AFFAIRS (DOE) REPUBLIC OF MALAWI MASTER PLAN STUDY ON RURAL ELECTRIFICATION IN MALAWI FINAL REPORT MAIN REPORT MARCH 2003 TOKYO ELECTRIC POWER SERVICES CO., LTD. MPN NOMURA RESEARCH INSTITUTE, LTD. JR 03-023 Contents 0 Executive Summary .................................................................................................................... 1 1 Background and Objectives ........................................................................................................ 4 1.1 Background ......................................................................................................................... 4 1.2 Objectives............................................................................................................................ 8 2 Process of Master Plan................................................................................................................ 9 2.1 Basic guidelines .................................................................................................................. 9 2.2 Identification of electrification sites ................................................................................. 10 2.3 Data and information collection........................................................................................ 10 2.4 Prioritization of electrification sites................................................................................. -
Rapid Epidemiological Mapping Of
7-7 tlp,-n a a RAPID EPIDEMIOLOGICAL MAPPING OF ONCHOCERCTASTS (REMO) rN MALAWI MISSION REPORT (UAY L6 - JUNE 1-5, 1997' FOR WORLD HEALTH ORGANTZATION AFRTCAN PROGRAUME FOR ONCHOCERCIASIS CONTROL (APOC) BY DR. B.E.B. NI{OKE (OVlrCP/cTDl 5O4lAPle7 I O40' STATUS: WHO Temporary Adviser (U197 lOt4329l Professor of Medical/Public Health Parasitology & Entomology School of Biological Sciences Imo State University PMB 2000 Owerri, Nigeria i. ' ., Phoner (234)83-23 05 85 (Home) a Fax: (2341A3-23 18 83 ( it, ') t" rfw JUNE 15, 1997 ,, /.l'^ Fr;r lrr iol nr.;1i :.rr" I .,, ;'1 !r 'y[' ruf II ) SUMMARY Under the sponsorship of the African Programme .for Onchocerciasii Control (APOC), Rapid Epidemiological Mapping of onchocerciasis was conducted in Malawi Uelireen 1,6th May and June l-6th L997. During the course of the exercise-, 4O5 villages were primarily selected to be examined for the prevalence of onchocercal nodules of due to which 48 ( 1f-. 85Ul were not sampled - inaccessibility. Pending the final Atlas GIS analysis of the data, the results showed that: L. O onchocerciasis is apparentty absent from all the 5 Northern Districts of Uafawi: ChitiPa, Karonga, Mzimba, Rurnphi, and NkhatabaY. 2.O In the central Region, onchocerciasis is absent in 7 districts of Kasungu, Nkhotakota, salima, Mchinji, Dowa, Ntchisi and Lilongwe out of the 9 Districts. Ntcheu District has endemic communities on the western border with Mozambique as welI as with the southern border with the Mwanza/Neno area. There is also onchocerciasis at the east-central- part of Dedza district. 3. O The Southern Region is the onchocerciasis zone in Malawi. -

Appeal Coordinating Office
150 route de Ferney, P.O. Box 2100 1211 Geneva 2, Switzerland Tel: 41 22 791 6033 Fax: 41 22 791 6506 e-mail: [email protected] Appeal Coordinating Office Malawi Famine Mitigation Follow-up – AFMW51 Appeal Target: US$ 2,017,307 Geneva, 6 September 2005 Dear Colleagues, Drought-prone Malawi is yet again suffering from food crisis this year following adverse climatic conditions arising from severe drought and erratic rains, inadequate accessibility to farm inputs and the effect of previous food shortage situations. The drop in crop performance, especially for the country's main staple food, maize, have created big food security concerns for many parts of the country including those that are currently on food aid. The immediate household food shortage caused by low expected yields from the current crops is an indicator that most households will have food shortage from August 2005 to April 2006 if no appropriate interventions are put in place. The continued grip of the food shortage, the increased funding of current appeal AFMW41 almost towards the end of the appeal period, the increased number of beneficiaries and the change in nature of implementation prompted the Malawi ACT Forum: Church of Central Africa Presbyterian (CCAP) Development Department of Synod of Livingstonia, Church of Central Africa Presbyterian (CCAP) Blantyre Synod, the Evangelical Lutheran Development Programme (ELDP), Christian Health Association of Malawi (CHAM) and Churches Action in Relief and Development (CARD), to submit this new proposal which will be for a implementation period of six additional months. The AFMW41 appeal will remain the same and will be closed, while this appeal represents new needs identified by the ACT members in Malawi. -

Chapter 7 Solar Power Generation Planning
CHAPTER 7 SOLAR POWER GENERATION PLANNING Chapter 7 Solar Power Generation Planning The electrification method based on the extension of distribution lines is known as on-grid electrification, while the method that utilizes photovoltaic solar power is known as off-grid electrification. In this chapter, results of the survey on the status of electrification by photovoltaic solar power in Malawi and the state of implementation of photovoltaic power projects funded by foreign countries are discussed. 7.1 The state of Solar Power in Malawi At present photovoltaic energy systems are used in Malawi in many rural sites far from the distribution line. PV residential systems are mostly owned by tobacco farmers, and PV systems for public facilities can be found at many hospitals, post offices, telephone exchange offices, etc. Photovoltaic energy in Malawi has enough potential for development with regard to environmental issues and also reflects a satisfactory degree of established technology. If the problem of the expense of photovoltaic could be solved, it is expected that this technology would spread throughout Malawi and contribute to overall electrification. Some specific knowledge is required to maintain PV systems although not as much as other systems. Furthermore, PV systems can generate electricity whenever solar irradiation is available. Most PV systems in Malawi are Solar Home Systems (SHS) as stand-alone type, being installed in areas far from the grid and where electricity generation by other methods (for example mini hydro) is not possible. There are also systems that are only installed temporarily until other electrification methods become available. The main components of a SHS are the Solar Panel, Battery and Battery Charge Controller (Fig. -

The Structure of Sexual Networks and the Spread of HIV in Sub-Saharan Africa: Evidence from Likoma Island (Malawi)
The structure of sexual networks and the spread of HIV in Sub-Saharan Africa: evidence from Likoma island (Malawi) Stéphane Helleringer Hans-Peter Kohler Department of Sociology Population Studies Center University of Pennsylvania It is widely believed that the HIV epidemic in Sub-Saharan Africa (SSA) is driven by transmission during unprotected heterosexual intercourse. In particular, infection with HIV in SSA is thought to be fueled by repeated contacts with sex workers or other highly sexually active group, and subsequently diffused to the general population through links of marriage or other stable types of partnerships. Such a theoretical model of sexual mixing has informed many policy simulations of interventions to stem the spread of the disease (see Oster 2005). However, empirical evidence for this diffusion process (i.e. from a group of highly active individuals to a low activity “periphery”) is somewhat scarce as epidemiological studies have generally reported weaker than expected relations between measures of such sexual behavior and risk/prevalence of HIV infection. At the individual level, differences in the rate of sexual partner acquisition only marginally predict an increased risk of infection for both prevalent (e.g. Gregson et al. 2002) and incident cases (e.g. Quigley et al. 2000). Similarly, at the population level, several comparative studies of the factors of HIV infection have found that differences in the prevalence of risky behaviors (high rate of partner change, contacts with sex workers etc.) could not explain the “uneven spread” of HIV across regions of SSA (Boerma et al. 2003). These discrepancies between indicators of sexual activity and prevalence/risk of HIV have been primarily attributed to two factors: reporting bias and differential mortality of HIV- infected individuals. -

Malawi Country Operational Plan 2017 Strategic Direction Summary
Malawi Country Operational Plan 2017 Strategic Direction Summary April 26, 2017 1 1.0 Goal Statement While there has been significant progress in the fight against HIV, Malawi still has 980,000 people living with HIV (PLHIV), including 350,000 undiagnosed. The Malawi Population-Based HIV Impact Assessment (MPHIA) showed significant progress toward the globally endorsed targets of 90-90-90. The number of new adult infections each year continues to decline (28,000/year in 2016), coinciding with an increase in ART coverage. With the number of annual HIV-related deaths reduced to 27,000/year in 2016, Malawi continues making progress toward epidemic control. However, MPHIA also highlights a disproportionately high HIV incidence among adolescent girls and young women (AGYW) with point estimates for HIV incidence 8 times higher among females aged 15-24 than males. Therefore, the overarching goal of COP17 is to interrupt HIV transmission by reducing incidence among AGYW through testing and treatment of potential sexual partners (men 15-40) and primary prevention (e.g., expansion of DREAMS and AGYW targeted interventions), thereby interrupting the lifecycle of HIV transmission and accelerating progress to epidemic control. The 1st 90 remains the greatest challenge and requires a number of key strategy shifts: Targeting testing and treatment strategies: Increased focus on targeting men and youth with the most efficient testing modalities (e.g., index case testing) and treatment strategies (e.g., same-day ART initiation) to achieve saturation across all age and gender bands in scale-up districts by the end of FY18. Increasing focus in five “acceleration” districts: Per the MPHIA, the epidemic is most intense in population-dense regions of Southern Malawi, especially Blantyre; therefore, PEPFAR will focus on Blantyre and four other high burden, scale up districts (deemed “acceleration” districts) that include 70% of the national gap to saturation. -

Malawi Coverage Survey 2017
Malawi Coverage Survey 2017 Measuring treatment coverage for schistosomiasis and soil transmitted helminths with preventive chemotherapy 1 Contents Contents .................................................................................................................................................. 2 Introduction ............................................................................................................................................ 4 Background to the Coverage Survey ....................................................................................................... 4 Schistosomiasis and STH in Malawi .................................................................................................... 5 Previous mapping ............................................................................................................................... 5 Treatment History ............................................................................................................................... 5 Previous Coverage Surveys ................................................................................................................. 6 2012 ................................................................................................................................................ 6 2014 ................................................................................................................................................ 6 2016 ...............................................................................................................................................