Still Mesoendemic Onchocerciasis in Two Cameroonian Community
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Reproductive Strategy of Chrysichthys Nigrodigitatus (Lacepede, 1803) in a Natural Environment in the Nkam River, Littoral Cameroon
Hindawi International Journal of Zoology Volume 2020, Article ID 1378086, 8 pages https://doi.org/10.1155/2020/1378086 Research Article Reproductive Strategy of Chrysichthys nigrodigitatus (Lacepede, 1803) in a Natural Environment in the Nkam River, Littoral Cameroon Claudine Tekounegning Tiogue´ ,1 Boddis Tsiguia Zebaze,2 Paul Zango,3 and Minette Eyango Tomedi-Tabi3 1Laboratory of Applied Ichthyology and Hydrobiology (LAIH), School of Wood, Water and Natural Resources (SWWNR), Faculty of Agronomy and Agricultural Sciences (FAAS), !e University of Dschang, P.O. Box 786, Ebolowa Antenna, Dschang, Cameroon 2Laboratory of Applied Ichthyology and Hydrobiology (LAIH), Department of Animal Productions, Faculty of Agronomy and Agricultural Sciences (FAAS), !e University of Dschang, P.O. Box 222, Dschang, Cameroon 3Laboratory for Aquaculture and Demography of Fisheries Resources (LADFR), Departement of Aquaculture, Institute of Fisheries and Aquatic Sciences of Yabassi (IFAS), !e University of Douala, P.O. Box 2701, Douala, Cameroon Correspondence should be addressed to Claudine Tekounegning Tiogue´; [email protected] Received 30 July 2019; Accepted 20 December 2019; Published 15 February 2020 Academic Editor: Cucco Copyright © 2020 Claudine Tekounegning Tiogue´ et al. (is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. A study on the reproductive strategy of Chrysichthys nigrodigitatus was conducted from October 2015 to August 2016, in the Nkam River in Yabassi, Littoral Region of Cameroon. For this purpose, 154 specimens of C. nigrodigitatus with total mean weight of 829.96 ± 829.58 g and total mean length of 367 ± 156 mm collected from artisanal fishermen were used. -
Page 1 C H a D N I G E R N I G E R I a G a B O N CENTRAL AFRICAN
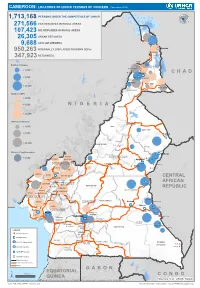
CAMEROON: LOCATIONS OF UNHCR PERSONS OF CONCERN (November 2019) 1,713,168 PERSONS UNDER THE COMPETENCENIGER OF UNHCR 271,566 CAR REFUGEES IN RURAL AREAS 107,423 NIG REFUGEES IN RURAL AREAS 26,305 URBAN REFUGEES 9,688 ASYLUM SEEKERS 950,263 INTERNALLY DISPLACED PERSONS (IDPs) Kousseri LOGONE 347,923 RETURNEES ET CHARI Waza Limani Magdeme Number of refugees EXTRÊME-NORD MAYO SAVA < 3,000 Mora Mokolo Maroua CHAD > 5,000 Minawao DIAMARÉ MAYO TSANAGA MAYO KANI > 20,000 MAYO DANAY MAYO LOUTI Number of IDPs < 2,000 > 5,000 NIGERIA BÉNOUÉ > 20,000 Number of returnees NORD < 2,000 FARO MAYO REY > 5,000 Touboro > 20,000 FARO ET DÉO Beke chantier Ndip Beka VINA Number of asylum seekers Djohong DONGA < 5,000 ADAMAOUA Borgop MENCHUM MANTUNG Meiganga Ngam NORD-OUEST MAYO BANYO DJEREM Alhamdou MBÉRÉ BOYO Gbatoua BUI Kounde MEZAM MANYU MOMO NGO KETUNJIA CENTRAL Bamenda NOUN BAMBOUTOS AFRICAN LEBIALEM OUEST Gado Badzere MIFI MBAM ET KIM MENOUA KOUNG KHI REPUBLIC LOM ET DJEREM KOUPÉ HAUTS PLATEAUX NDIAN MANENGOUBA HAUT NKAM SUD-OUEST NDÉ Timangolo MOUNGO MBAM ET HAUTE SANAGA MEME Bertoua Mbombe Pana INOUBOU CENTRE Batouri NKAM Sandji Mbile Buéa LITTORAL KADEY Douala LEKIÉ MEFOU ET Lolo FAKO AFAMBA YAOUNDE Mbombate Yola SANAGA WOURI NYONG ET MARITIME MFOUMOU MFOUNDI NYONG EST Ngarissingo ET KÉLLÉ MEFOU ET HAUT NYONG AKONO Mboy LEGEND Refugee location NYONG ET SO’O Refugee Camp OCÉAN MVILA UNHCR Representation DJA ET LOBO BOUMBA Bela SUD ET NGOKO Libongo UNHCR Sub-Office VALLÉE DU NTEM UNHCR Field Office UNHCR Field Unit Region boundary Departement boundary Roads GABON EQUATORIAL 100 Km CONGO ± GUINEA The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations Sources: Esri, USGS, NOAA Source: IOM, OCHA, UNHCR – Novembre 2019 Pour plus d’information, veuillez contacter Jean Luc KRAMO ([email protected]). -

Minmap Region Du Littoral Synthese Des Donnees Sur La Base Des Informations Recueillies
MINMAP REGION DU LITTORAL SYNTHESE DES DONNEES SUR LA BASE DES INFORMATIONS RECUEILLIES Nbre de N° Désignation des MO/MOD Montant des Marchés N° page Marchés 1 Communauté Urbaine de de Douala 94 89 179 421 671 3 2 Communité Urbaine d'édéa 5 89 000 000 14 3 Communité Urbaine de Nkongsamba 6 198 774 344 15 4 Services déconcentrés Régionaux 17 718 555 000 16 Département du Moungo 5 Services déconcentrés départementaux 5 145 000 000 18 6 Commune de BARE BAKEM 2 57 000 000 18 7 Commune de BONALEA 3 85 500 000 19 8 Commune de DIBOMBARI 3 105 500 000 19 9 Commune de LOUM 16 445 395 149 19 10 Commune de MANJO 8 132 000 000 21 11 Commune de MBANGA 3 108 000 000 22 12 Commune de MELONG 12 173 500 000 22 13 Commune de NJOMBE PENJA 5 132 000 000 24 14 Commune d'EBONE 12 299 500 000 25 15 Commune de MOMBO 3 77 000 000 26 16 Commune de NKONGSAMBA I 1 27 000 000 26 17 Commune de NKONGSAMBA II 3 59 250 000 27 18 Commune de NKONGSAMBA III 2 87 000 000 27 TOTAL Département 78 1 933 645 149 Département du Nkam 19 Services déconcentrés départementaux 12 232 596 000 28 20 Commune de NKONDJOCK 16 258 623 000 29 21 Commune de YABASSI 14 221 000 000 31 22 Commune de YINGUI 4 53 500 000 33 23 Commune de NDOBIAN 17 345 418 000 33 TOTAL Département 63 1 111 137 000 Département de la Sanaga Maritime 24 Services déconcentrés départementaux 8 90 960 000 36 25 Commune de Dibamba 3 72 000 000 37 26 Commune de Dizangue 5 88 500 000 37 27 Commune de MASSOCK 4 233 230 000 38 28 Commune de MOUANKO 15 582 770 000 38 29 Commune de NDOM 12 339 237 000 40 Nbre de N° Désignation -

GEF Prodoc TRI Cameroon 28 02 18
International Union for the Conservation of Nature Country: Cameroon PROJECT DOCUMENT Project Title: Supporting Landscape Restoration and Sustainable Use of local plant species and tree products (Bambusa ssp, Irvingia spp, etc) for Biodiversity Conservation, Sustainable Livelihoods and Emissions Reduction in Cameroon BRIEF DESCRIPTION OF THE PROJECT The Republic of Cameroon has a diverse ecological landscape, earning her the title “Africa in Miniature”. The southern portions of Cameroon’s forests are part of the Congo Basin forest ecosystem, the second largest remaining contiguous block of rainforest on Earth, after the Amazon. In addition to extensive Mangrove belts, Cameroon also holds significant portions of the Lower Guinea Forest Ecosystems and zones of endemism extending into densely settled portions of the Western Highlands and Montagne forests. The North of the country comprising the Dry Sudano-Sahelian Savannah Zones is rich in wildlife, and home to dense human and livestock populations. Much of the population residing in these areas lives in extreme poverty. This diversity in biomes makes Cameroon one of the most important and unique hotspots for biodiversity in Africa. However, human population growth, migrations, livelihoods strategies, rudimentary technologies and unsustainable land use for agriculture and small-scale forestry, energy and livestock, are contributing to biodiversity loss and landscape degradation in Cameroon. Despite strong institutional frameworks, forest and environmental policies/legislation, and a human resource capital, Cameroon’s network of biomes that include all types of forests, tree-systems, savannahs, agricultural mosaics, drylands, etc., are progresively confronted by various forms of degradation. Degradation, which is progressive loss of ecosystem functions (food sources, water quality and availability, biodversity, soil fertility, etc), now threatens the livelihoods of millions of Cameroonians, especially vulnerable groups like women, children and indigenous populations. -

Dictionnaire Des Villages Du Mbam P
OFFICE DE LA RECHERCHE REPUBliQUE FEDERALE SCIENTIFIQUE ET TECHNIQUE DU OUT,RE·MER CAMEROUN CENTRE OR5TOM DE YAOUNDE DICTIONNAIRE DES _VILLAGES DU MBAM D'après la documentation réunie par ~la Section de Géographie de l'I.R.CAM.3 REPERTQIRE GEOGRAPHIQUE DU CAMEROUN FASCICULE n° 1 1 rR-GAM 8. P. '9J SH. n° 31 YAOUNDÉ Mai 1966 REPERTOIRE GEOGRAPHIQUE DU CAMEROUN Fasc. Tableau de la population du Cameroun, 68 p. Fév. 1965 SH, N° 17 Fasc. 2 Dictionnaire des villages du Dia et Lobo, 89 p. Juin 1965 SH. N° 22 Fasc. 3 Dictionnaire des villages de la Haute-Sanaga, 53 p. Août 1965 SH. N° 23 Fasc. 4 Dictionnaire des villages du Nyong et Mfoumou, 49 p. Octobre 1965 SH. N° 24 Fasc. 5 Dictionnaire des villages du Nyong et Soo 45 p. Novembre 1965 SH. N° 25 Fasc. 6 Dictionnaire des villages du Ntem 126 p. Décembre 1965 SH. N° 26 Fasc. 7 Dictionnaire- des villages de la Mefou 108 p. Janvier 1966 SH. N° 27 Fasc. 8 Dictionnaire des villages du Nyong et Kellé 51 p. Février 1966 SH. N° 28 Fasc. 9 Dictionnaire des villages de la Lékié 71 p. Mars 1966 SH. N° 29 Fasc. 10 Dictionnaire des villages de Kribi P. Mars 1966 SH. N° 30 Fasc. 11 Dictionnaire des villages du Mbam P. 60 Mai 1966 SH. N° 31 Fasc. 12 Dictionnaire des villages de Boumba Ngoko (en préparation) Fasc. 13 ùictionnaire des villages de Lom-et-Diérem (en préparation! omCE DE LA RECHERCHE SCIENTIFIQUE RERJBLlQUE FEDERALE ET TECHNI~E OUmE-MER ID CAMEROUN _ • _cee- -- - CENTRE ORSTOM DE YAOUNDE DICTIONNAIRE ~ VILLAGES DU ...........M B A M MAI 1!66 S.R. -

Centre Region Classifications
Centre Region Classifications Considering the World Bank list of economies (June 2020) OTHM centres have been classified into three separate regions: • Region 1: High income economies; • Region 2: Upper middle income economies; and • Region 3: Lower middle income and low income economies. Centres in the United Kingdom falls into Region 1 along with other high-income economies – (normal fees apply for all Region 1 Centres). Prospective centres and learners should visit www.othm.org.uk to find which region their centre falls into and pay the appropriate fees. Economy Income group Centre class Afghanistan Low income Region 3 Albania Upper middle income Region 2 Algeria Lower middle income Region 3 American Samoa Upper middle income Region 2 Andorra High income Region 1 Angola Lower middle income Region 3 Antigua and Barbuda High income Region 1 Argentina Upper middle income Region 2 Armenia Upper middle income Region 2 Aruba High income Region 1 Australia High income Region 1 Austria High income Region 1 Azerbaijan Upper middle income Region 2 Bahamas, The High income Region 1 Bahrain High income Region 1 Bangladesh Lower middle income Region 3 Barbados High income Region 1 Belarus Upper middle income Region 2 Belgium High income Region 1 Belize Upper middle income Region 2 Benin Lower middle income Region 3 Bermuda High income Region 1 Bhutan Lower middle income Region 3 Bolivia Lower middle income Region 3 Bosnia and Herzegovina Upper middle income Region 2 Botswana Upper middle income Region 2 Brazil Upper middle income Region 2 British -

Dictionnaire Des Villages De La Haute Sanaga a Été Entièrement Remise À Jour Et Corrigée En Fonction Des Derniers Renseignements Que Nous Possédons
OFFICE DE LA RECHERCHE REPUBLIQUE FEDEIlA~ SCIENTIFIQUE ET TECHNIQUE DU OUTRE-MER CAMEROUN CENTRE ORSTOM DE YAOUNDE DICTIONNAIR'E DES VILLAGES DE LA HAUTE SANAGA (2ème Editan) ~aprèS la documentation réunie ~-:-l ~ection de Géographie de l' ORST~ "~fUTOJkGEOGRAPHIQUE DU CAMEROUN FASCICULE N° 3 B. P. 193 SH. n° 50 YAOUNDE Août 1968 REPERTOIRE GEOGRAPHIQUE DU CAMEROUN Fasc. Tableau de la population du Cameroun, 68 p. Fév. 1965 SH. N° 17 Fasc. 2 Dictionnaire des villages du Dia et lobo, 89 p. Juin 1965 SH. N° 22 Fasc. 3 Dictionnaire des villages de la Haute-Sanaga, 44 p. Août 1968 SH. N° 50 (2éme édition) Fasc. 4 Dictionnaire des villages du Nyong et Mfoumou, 49 p. Octobre 1965 SH. N° 24 ~: Fasc. 5 Dictio~riaire des villages du Nyong et Soo 45 p. Novembre 1965 SH. N° 25 Fasc. 6 Dictionnaire des villages du Ntem 102 p. Juin 1968 SH. N° 46 (2ème édition) Fasc. 7 Dictionnaire des villages de la Mefou 108 p. Janvier 1966 SH. N° 27 Fa sc. 8 Dictionnaire des villages du Nyong et Kellé 51 p. Février 1966 SH. N° 28 Fa sc. 9 Dictionnaire des villages de la lékié 71 p. Mars 1966 SH. N° 29 Fasc. 10 Dictionnaire des villages de Kribi P. Mars 1966 SH. N° 30 Fasc. 11 Dictionnaire des villages du Mbam 60 P. Mai 1966 SH. N° 31 Fasc. 12 Dictionnaire des villages de Boumba Ngoko 34 p. Juin 1966 SH. 39 Fasc. 13 Dictionnaire des villages de lom-et-Djérem 35 p. Juillet 1967 SH. 40 Fasc. 14 Dictionnaire des villages de la Kadei 52 p. -
Approved by the Ministry of the Environment and Forests
Project of Independent Observation in Support of Forest Law Enforcement in Cameroon Approved by the Ministry of the Environment and Forests Report No. 027 En Joint Mission: Central Control Unit – Independent Observer ------------------------------- Title: None Location: Central Province Mission date: September 20-21, 2002 Company: GCI Nyanzom, IBC Independent Observer (Global Witness): Mr. Stuart Wilson, Project Director Mr. Owada Jean Cyrille, Technical Assistant Mr. Tangyie Ché Célestine, Driver TABLE OF CONTENTS 1. SUMMARY ............................................................................................................. 1 2. RESOURCES USED ............................................................................................. 2 3. COMPOSITION OF THE MISSION................................................................ 2 4. CONSTRAINTS ..................................................................................................... 2 5. RESULTS OF THE MISSION............................................................................ 2 5.1. Summary of the case ............................................................................................. 2 5.2. Meetings with IBC representatives and various external services representatives 2 5.3. Official hearing of the Ombessa forest law enforcement official ......................... 3 6. CONCLUSIONS AND RECOMMENDATIONS......................................... 4 Appendix ......................................................................................................................... -

MINMAP Région Du Littoral
MINMAP Région du Littoral SYNTHESE DES DONNEES SUR LA BASE DES INFORMATIONS RECUEILLIES Nbre de Montant des N° Désignation des MO/MOD N° Page Marchés Marchés 1 Communauté Urbaine d'Edéa 6 1 747 550 008 3 2 Services déconcentrés Régionaux 10 534 821 000 4 TOTAL 16 2 282 371 008 Département du Wouri 3 Services déconcentrés départementaux 6 246 700 000 5 4 Commune de Douala 1 9 370 778 000 5 5 Commune de Douala 2 9 752 778 000 6 6 Commune de Douala 3 12 273 778 000 8 7 Commune de Douala 4 10 278 778 000 9 8 Commune de Douala 5 10 204 605 268 10 9 Commune de Douala 6 10 243 778 000 11 TOTAL 66 2 371 195 268 Département du Moungo 10 Services déconcentrés départementaux 10 159 560 000 12 11 Commune de Bare Bakem 9 234 893 804 13 12 Commune de Bonalea 11 274 397 840 14 13 Commune de Dibombari 11 267 278 000 15 14 Commune de Loum 12 228 397 903 16 15 Commune de Manjo 8 160 940 286 18 16 Commune de Mbanga 10 228 455 858 19 17 Commune de Melong 17 291 778 000 20 18 Commune de Njombe Penja 17 427 728 000 21 19 Commune d'Ebone 10 190 778 000 23 20 Commune de Mombo 9 163 878 000 24 21 Commune de Nkongsamba I 7 161 000 000 25 22 Commune de Nkongsamba II 6 172 768 640 25 23 Commune de Nkongsamba III 9 195 278 000 26 TOTAL 146 3 157 132 331 Département de la Sanaga Maritime 24 Services déconcentrés départementaux 10 214 167 000 27 25 Commune de Dibamba 14 358 471 384 28 26 Commune de Dizangue 13 252 678 000 29 27 Commune de Massock 16 319 090 512 30 28 Commune de Mouanko 9 251 001 000 31 29 Commune de Ndom 17 340 778 000 31 30 Commune de Ngambe 9 235 -

Impact Assessment on By-Catch Artisanal Fisheries: Sea Turtles And
quac d A ul n tu a r e s e J i o r u e r h n Ayissi and Jiofack, Fish Aquac J 2014, 5:3 s i a F l Fisheries and Aquaculture Journal DOI: 10.4172/ 2150-3508.1000099 ISSN: 2150-3508 Research Article Open Access Impact Assessment on By-catch Artisanal Fisheries: Sea Turtles and Mammals in Cameroon, West Africa Ayissi I1,2,3,4,* and Jiofack TJE5 1University of Abdelmalek Essaâdi, Department of Biology, Faculty of Science, Tetouan 2121, Morocco 2Cameroon Marine Biology Association, Morocco 3Specialized Research Center for Marine Ecosystems in Kribi-Cameroon, Cameroon 4Institute of Fisheries and Aquatic Sciences (ISH) at Yabassi, University of Douala, PO Box 2701, Douala, Cameroon 5 Sub-Regional School and Postdoctoral Water Development and Integrated Management of Forests and Tropical Territories, Kinshasa, RDC, Congo *Corresponding author: Ayissi I, University of Abdelmalek Essaâdi, Department of Biology, Faculty of Science, Tetouan 2121, Morocco, Tel: +237 97350175; E-mail: [email protected] Received date: January 20, 2014; Accepted date: July 09, 2014; Published date: July 16, 2014 Copyright: © 2014 Ayissi I, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract The by-catch assessment has been carried out along Cameroon coastline to map artisanal fishing effort and quantify impact of by-catch on sea turtles and marine mammals during three months from June to September 2011 and specific objectives include: - To interview fishermen in various fishing villages or ports in Cameroon regarding fishing effort and catch. -

CAMEROON Education Environment, Water and Sanitation HIV/AIDS Project Income-Generating Activities
Health Child protection CAMEROON Education Environment, water and sanitation HIV/AIDS project Income-generating activities March 2012 – February 2015 Project overview OBJECTIVE Prevention, comprehensive care and promotion of the rights of the most vulnerable against HIV/AIDS in the health district of Okola, in the Centre Region. Project funded by the Région Ile de France and the city of Paris CONTEXT HIV/AIDS in Cameroon The 2/3 of the HIV positive people in the world live in the Sub-Saharan Africa. In Cameroon, it is estimated that they are 550,000, to which 300,000 HIV orphans must be added. The Centre is one of the most affected Region (out of the 10 Regions composing the country), as it accounts for 20% of the national HIV positive population. The most vulnerable people to the epidemic are : - Women, who for biological and social reasons (less control on their sexuality than men), make up 2/3 of the HIV positive persons in the country, -Young people (amongst the 60,000 affected people each year, half of them is from 15 to 24). The infection level is mainly due to the lack of information about HIV/AIDS. It implies a low condom use in Cameroon, while it is the most effective way to prevent HIV/AIDS. The access to HIV testing is also lacking: in 2004, 80% of women and about 90% of men in the area had never been tested for HIV. The comprehensive care services (therapeutic, psychosocial, economic support, etc.) for people living with HIV are rare, not to say missing in many rural areas. -
Assessment of Prunus Africana Bark Exploitation Methods and Sustainable Exploitation in the South West, North-West and Adamaoua Regions of Cameroon
GCP/RAF/408/EC « MOBILISATION ET RENFORCEMENT DES CAPACITES DES PETITES ET MOYENNES ENTREPRISES IMPLIQUEES DANS LES FILIERES DES PRODUITS FORESTIERS NON LIGNEUX EN AFRIQUE CENTRALE » Assessment of Prunus africana bark exploitation methods and sustainable exploitation in the South west, North-West and Adamaoua regions of Cameroon CIFOR Philip Fonju Nkeng, Verina Ingram, Abdon Awono February 2010 Avec l‟appui financier de la Commission Européenne Contents Acknowledgements .................................................................................................... i ABBREVIATIONS ...................................................................................................... ii Abstract .................................................................................................................. iii 1: INTRODUCTION ................................................................................................... 1 1.1 Background ................................................................................................. 1 1.2 Problem statement ...................................................................................... 2 1.3 Research questions .......................................................................................... 2 1.4 Objectives ....................................................................................................... 3 1.5 Importance of the study ................................................................................... 3 2: Literature Review .................................................................................................