Oup Hropen Hox015 1..20 ++
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Program Nr: 1 from the 2004 ASHG Annual Meeting Mutations in A
Program Nr: 1 from the 2004 ASHG Annual Meeting Mutations in a novel member of the chromodomain gene family cause CHARGE syndrome. L.E.L.M. Vissers1, C.M.A. van Ravenswaaij1, R. Admiraal2, J.A. Hurst3, B.B.A. de Vries1, I.M. Janssen1, W.A. van der Vliet1, E.H.L.P.G. Huys1, P.J. de Jong4, B.C.J. Hamel1, E.F.P.M. Schoenmakers1, H.G. Brunner1, A. Geurts van Kessel1, J.A. Veltman1. 1) Dept Human Genetics, UMC Nijmegen, Nijmegen, Netherlands; 2) Dept Otorhinolaryngology, UMC Nijmegen, Nijmegen, Netherlands; 3) Dept Clinical Genetics, The Churchill Hospital, Oxford, United Kingdom; 4) Children's Hospital Oakland Research Institute, BACPAC Resources, Oakland, CA. CHARGE association denotes the non-random occurrence of ocular coloboma, heart defects, choanal atresia, retarded growth and development, genital hypoplasia, ear anomalies and deafness (OMIM #214800). Almost all patients with CHARGE association are sporadic and its cause was unknown. We and others hypothesized that CHARGE association is due to a genomic microdeletion or to a mutation in a gene affecting early embryonic development. In this study array- based comparative genomic hybridization (array CGH) was used to screen patients with CHARGE association for submicroscopic DNA copy number alterations. De novo overlapping microdeletions in 8q12 were identified in two patients on a genome-wide 1 Mb resolution BAC array. A 2.3 Mb region of deletion overlap was defined using a tiling resolution chromosome 8 microarray. Sequence analysis of genes residing within this critical region revealed mutations in the CHD7 gene in 10 of the 17 CHARGE patients without microdeletions, including 7 heterozygous stop-codon mutations. -

A Computational Approach for Defining a Signature of Β-Cell Golgi Stress in Diabetes Mellitus
Page 1 of 781 Diabetes A Computational Approach for Defining a Signature of β-Cell Golgi Stress in Diabetes Mellitus Robert N. Bone1,6,7, Olufunmilola Oyebamiji2, Sayali Talware2, Sharmila Selvaraj2, Preethi Krishnan3,6, Farooq Syed1,6,7, Huanmei Wu2, Carmella Evans-Molina 1,3,4,5,6,7,8* Departments of 1Pediatrics, 3Medicine, 4Anatomy, Cell Biology & Physiology, 5Biochemistry & Molecular Biology, the 6Center for Diabetes & Metabolic Diseases, and the 7Herman B. Wells Center for Pediatric Research, Indiana University School of Medicine, Indianapolis, IN 46202; 2Department of BioHealth Informatics, Indiana University-Purdue University Indianapolis, Indianapolis, IN, 46202; 8Roudebush VA Medical Center, Indianapolis, IN 46202. *Corresponding Author(s): Carmella Evans-Molina, MD, PhD ([email protected]) Indiana University School of Medicine, 635 Barnhill Drive, MS 2031A, Indianapolis, IN 46202, Telephone: (317) 274-4145, Fax (317) 274-4107 Running Title: Golgi Stress Response in Diabetes Word Count: 4358 Number of Figures: 6 Keywords: Golgi apparatus stress, Islets, β cell, Type 1 diabetes, Type 2 diabetes 1 Diabetes Publish Ahead of Print, published online August 20, 2020 Diabetes Page 2 of 781 ABSTRACT The Golgi apparatus (GA) is an important site of insulin processing and granule maturation, but whether GA organelle dysfunction and GA stress are present in the diabetic β-cell has not been tested. We utilized an informatics-based approach to develop a transcriptional signature of β-cell GA stress using existing RNA sequencing and microarray datasets generated using human islets from donors with diabetes and islets where type 1(T1D) and type 2 diabetes (T2D) had been modeled ex vivo. To narrow our results to GA-specific genes, we applied a filter set of 1,030 genes accepted as GA associated. -

Identification of a Novel Deletion Mutation in DPY19L2 from An
Li et al. Molecular Cytogenetics (2020) 13:24 https://doi.org/10.1186/s13039-020-00495-1 CASE REPORT Open Access Identification of a novel deletion mutation in DPY19L2 from an infertile patient with globozoospermia: a case report You-zhu Li1†, Rong-feng Wu1†, Xing-shen Zhu2†, Wen-sheng Liu2, Yuan-yuan Ye1, Zhong-xian Lu2* and Na Li3* Abstract Background: Male infertility is an increasing medical concern worldwide. In most cases, genetic factors are considered as the main cause of the disease. Globozoospermia (MIM102530) (also known as round-headed sperm) is a rare and severe malformed spermatospermia caused by acrosome deficiency or severe malformation. A subset of genetic mutations, such as DNAH6, SPATA16, DPY19L2, PICK1, and CCIN related to globozoospermia, have been reported in the past few years. The DPY19L2 mutation is commonly found in patients with globozoospermia. Herein, a 180-kbp homozygote deletion at 12q14.2 (g.63950001–64130000) was identified by copy number variation sequencing (CNVseq) in a patient with a globozoospermia, including the complete deletion of DPY19L2. Case presentation: A 27-year-old patient at the First Affiliated Hospital of Xiamen University was diagnosed with infertility because, despite normal sexual activity for 4 years, his wife did not conceive. The patient was in good health with no obvious discomfort, no history of adverse chemical exposure, and no vices, such as smoking and drinking. The physical examination revealed normal genital development. However, semen tests showed a normal sperm count of 0% and the morphology was the round head. Sperm cytology showed that acrosomal enzyme was lower than normal. -

The Oedipus Hex: Regulating Family After Marriage Equality
Florida State University College of Law Scholarship Repository Scholarly Publications 11-2015 The Oedipus Hex: Regulating Family After Marriage Equality Courtney Megan Cahill Florida State University College of Law Follow this and additional works at: https://ir.law.fsu.edu/articles Part of the Constitutional Law Commons, Family Law Commons, Law and Society Commons, and the Sexuality and the Law Commons Recommended Citation Courtney Megan Cahill, The Oedipus Hex: Regulating Family After Marriage Equality, 49 U.C. DAVIS L. REV. 183 (2015), Available at: https://ir.law.fsu.edu/articles/520 This Article is brought to you for free and open access by Scholarship Repository. It has been accepted for inclusion in Scholarly Publications by an authorized administrator of Scholarship Repository. For more information, please contact [email protected]. The Oedipus Hex: Regulating Family After Marriage Equality ∗ Courtney Megan Cahill Now that national marriage equality for same-sex couples has become the law of the land, commentators are turning their attention from the relationships into which some gays and lesbians enter to the mechanisms on which they — and many others — rely in order to reproduce. Even as one culture war makes way for another, however, there is something that binds them: a desire to establish the family. This Article focuses on a problematic manifestation of that desire: the incest prevention justification. The incest prevention justification posits that the law ought to regulate alternative reproduction in order to minimize the potential for accidental incest between individuals involved in the donor conception process. A leading argument offered by both conservatives and progressives in defense of greater regulation of alternative reproduction, the incest prevention justification hearkens back in troubling ways to a taboo long used in American law to discipline the family. -

Supplementary Materials
Supplementary materials Supplementary Table S1: MGNC compound library Ingredien Molecule Caco- Mol ID MW AlogP OB (%) BBB DL FASA- HL t Name Name 2 shengdi MOL012254 campesterol 400.8 7.63 37.58 1.34 0.98 0.7 0.21 20.2 shengdi MOL000519 coniferin 314.4 3.16 31.11 0.42 -0.2 0.3 0.27 74.6 beta- shengdi MOL000359 414.8 8.08 36.91 1.32 0.99 0.8 0.23 20.2 sitosterol pachymic shengdi MOL000289 528.9 6.54 33.63 0.1 -0.6 0.8 0 9.27 acid Poricoic acid shengdi MOL000291 484.7 5.64 30.52 -0.08 -0.9 0.8 0 8.67 B Chrysanthem shengdi MOL004492 585 8.24 38.72 0.51 -1 0.6 0.3 17.5 axanthin 20- shengdi MOL011455 Hexadecano 418.6 1.91 32.7 -0.24 -0.4 0.7 0.29 104 ylingenol huanglian MOL001454 berberine 336.4 3.45 36.86 1.24 0.57 0.8 0.19 6.57 huanglian MOL013352 Obacunone 454.6 2.68 43.29 0.01 -0.4 0.8 0.31 -13 huanglian MOL002894 berberrubine 322.4 3.2 35.74 1.07 0.17 0.7 0.24 6.46 huanglian MOL002897 epiberberine 336.4 3.45 43.09 1.17 0.4 0.8 0.19 6.1 huanglian MOL002903 (R)-Canadine 339.4 3.4 55.37 1.04 0.57 0.8 0.2 6.41 huanglian MOL002904 Berlambine 351.4 2.49 36.68 0.97 0.17 0.8 0.28 7.33 Corchorosid huanglian MOL002907 404.6 1.34 105 -0.91 -1.3 0.8 0.29 6.68 e A_qt Magnogrand huanglian MOL000622 266.4 1.18 63.71 0.02 -0.2 0.2 0.3 3.17 iolide huanglian MOL000762 Palmidin A 510.5 4.52 35.36 -0.38 -1.5 0.7 0.39 33.2 huanglian MOL000785 palmatine 352.4 3.65 64.6 1.33 0.37 0.7 0.13 2.25 huanglian MOL000098 quercetin 302.3 1.5 46.43 0.05 -0.8 0.3 0.38 14.4 huanglian MOL001458 coptisine 320.3 3.25 30.67 1.21 0.32 0.9 0.26 9.33 huanglian MOL002668 Worenine -

Siblings Conceived by Donor Sperm Are Finding Each Other
Siblings conceived by donor sperm are finding each other By Amy Harmon NEW YORK TIMES NEWS SERVICE Like most anonymous sperm donors, Donor 150 of the California Cryobank probably will never meet any offspring he has fathered through the sperm bank. There are at least four children, according to the bank's records, and perhaps many more, since the dozens of women who have bought Donor 150's sperm are not required to report when they have a baby. The half-siblings – twins Erin and Rebecca Baldwin, 17, (right); Justin Senk, 15, (center); and McKenzie Gibson, 12, and her 18-year-old brother,Tyler – found each other in a registry. Even the mothers know only the code number the bank uses for identification and the fragments of personal information provided in his donor profile that drew them to select Donor 150 over other candidates. But two of his genetic daughters, born to different mothers and living in different states, have been e-mailing and talking on the phone regularly since learning of each other's existence this summer. They plan to meet over Thanksgiving. Danielle Pagano, 16, and JoEllen Marsh, 15, connected through the Donor Sibling Registry, a Web site that is helping to open a new chapter in the oldest form of assisted reproductive technology. The three-year-old site allows parents and offspring to enter their contact information and search for others by sperm bank and donor number. Donors who want to shed their anonymity are especially welcome, but the vast majority of the site's 1,001 matches are between half-siblings. -
Maximizing Autonomy and the Changing View of Donor Conception: the Creation of a National Donor Registry
DePaul Journal of Health Care Law Volume 12 Issue 1 Winter 2009 Article 9 October 2015 Maximizing Autonomy and the Changing View of Donor Conception: The Creation of a National Donor Registry Jean Benward Andrea Mechanick Braverman Bette Galen Follow this and additional works at: https://via.library.depaul.edu/jhcl Recommended Citation Jean Benward, Andrea Mechanick Braverman & Bette Galen, Maximizing Autonomy and the Changing View of Donor Conception: The Creation of a National Donor Registry, 12 DePaul J. Health Care L. 225 (2009) Available at: https://via.library.depaul.edu/jhcl/vol12/iss1/9 This Article is brought to you for free and open access by the College of Law at Via Sapientiae. It has been accepted for inclusion in DePaul Journal of Health Care Law by an authorized editor of Via Sapientiae. For more information, please contact [email protected]. MAXIMIZING AUTONOMY AND THE CHANGING VIEW OF DONOR CONCEPTION: THE CREATION OF A NATIONAL DONOR REGISTRY Jean Benward, L. C.S. W. Andrea Mechanick Braverman,Ph.D. Bette Galen, L. C.S. W. "It has long been an axiom of mine that the little things are infinitely the most important" Sir Arthur Conan Doyle INTRODUCTION AND OVERVIEW We can only estimate the number of donor conceived children in the United States. The frequently cited number of 30,000 births a year from sperm donation comes from a US government sponsored study done in 1987, over 20 years ago.' Although most donor sperm now comes from commercial sperm banks that keep records on donors and sale of sperm, neither physicians, IVF programs, nor parents consistently report pregnancies or births to sperm banks nor do most sperm banks reliably follow up with recipients to track births. -

HARS2 Gene Histidyl-Trna Synthetase 2, Mitochondrial
HARS2 gene histidyl-tRNA synthetase 2, mitochondrial Normal Function The HARS2 gene provides instructions for making an enzyme called mitochondrial histidyl-tRNA synthetase. This enzyme is important in the production (synthesis) of proteins in cellular structures called mitochondria, the energy-producing centers in cells. While most protein synthesis occurs in the fluid surrounding the nucleus (cytoplasm), some proteins are synthesized in the mitochondria. During protein synthesis, in either the mitochondria or the cytoplasm, a type of RNA called transfer RNA (tRNA) helps assemble protein building blocks (amino acids) into a chain that forms the protein. Each tRNA carries a specific amino acid to the growing chain. Enzymes called aminoacyl-tRNA synthetases, including mitochondrial histidyl- tRNA synthetase, attach a particular amino acid to a specific tRNA. Mitochondrial histidyl-tRNA synthetase attaches the amino acid histidine to the correct tRNA, which helps ensure that histidine is added at the proper place in the mitochondrial protein. Health Conditions Related to Genetic Changes Perrault syndrome At least two mutations in the HARS2 gene have been found to cause Perrault syndrome. This rare condition is characterized by hearing loss in males and females with the disorder and abnormalities of the ovaries in affected females. The HARS2 gene mutations involved in Perrault syndrome reduce the activity of mitochondrial histidyl- tRNA synthetase. A shortage of functional mitochondrial histidyl-tRNA synthetase prevents the normal assembly of new proteins within mitochondria. Researchers speculate that impaired protein assembly disrupts mitochondrial energy production. However, it is unclear exactly how HARS2 gene mutations lead to hearing problems and ovarian abnormalities in affected individuals. -
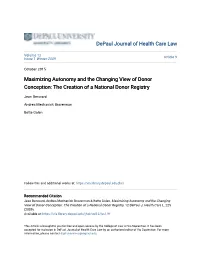
I Was a Donor at California Cryobank Who Was Open to Contact and Still Every Time a Biological Child of Mine Has Reached out They Have Put up Roadblocks
CALIFORNIA CRYOBANK (CCB) Note From Wendy: For those of you who used California Cryobank, and wonder why your donor hasn't yet registered on the DSR, here's a possible reason why: A former California Cryobank donor emailed me about what CCB had just told him about the DSR. He said, "...they were quite strong in their position that I should NOT register [on the DSR] bc there are likely errors with people putting wrong donor id, or even fakes, so that if I register, CBank says there's more than a slim chance I'd be reaching out or opening up to people not really offspring of mine." If you used CCB or are a CCB offspring, I encourage you to let CCB know how you feel about them discouraging donors from posting and connecting on the DSR. This is from the sperm bank who has been known to delete urgent medical information from a donor’s profile? We have been operating since 2000, long before CCB ever thought about having a registry. We spend many thousands of dollars each year to maintain and protect our website and our member's privacy. We have successfully connected more than 19,400 people, with more than 70,000 members. In all that time, and through all those members, we had one single donor impostor, a couple of years ago. I caught him within the first 24 hours. Certainly not worthy of negating our 20 years of hard work and thousands of successful connections! 8/2020 DSR’s Facebook Group I was a donor at California Cryobank who was open to contact and still every time a biological child of mine has reached out they have put up roadblocks. -

A New AURKC Mutation Causing Macrozoospermia
A new AURKC mutation causing macrozoospermia: implications for human spermatogenesis and clinical diagnosis Mariem Ben Khelifa 1 2 3 , Raoudha Zouari 4 , Radu Harbuz 2 1 , Lazhar Halouani 4 , Christophe Arnoult 1 , Joël Lunardi 2 5 , Pierre F. Ray 1 2 * 1 AGIM, AGeing and IMagery, CNRS FRE3405 Université Joseph Fourier - Grenoble I , Ecole Pratique des Hautes Etudes , CNRS : UMR5525 , Faculté de médecine de Grenoble, 38700 La Tronche,FR 2 Laboratoire de biochimie et génétique moléculaire CHU Grenoble , 38043 Grenoble,FR 3 Molecular Investigation of Genetic Orphan Diseases Research Unit Institut Pasteur de Tunis , Research Unit UR04/SP03,TN 4 Clinique de la reproduction les Jasmins Clinique de la reproduction les Jasmins , 23, Av. Louis BRAILLE, 1002 Tunis,TN 5 GIN, Grenoble Institut des Neurosciences INSERM : U836 , CEA , Université Joseph Fourier - Grenoble I , CHU Grenoble , UJF - Site Santé La Tronche BP 170 38042 Grenoble Cedex 9,FR * Correspondence should be addressed to: Pierre Ray <[email protected] > Abstract The presence of close to 100% large-headed multi-tailed spermatozoa in the ejaculate has been described as a rare phenotype of male infertility with a very poor prognosis. We demonstrated previously that most cases were caused by a homozygous mutation (c.144delC) in the Aurora Kinase C gene (AURKC) leading to the absence or the production of a nonfunctional protein. AURKC deficiency in these patients blocked meiosis and resulted in the production of tetraploid spermatozoa unsuitable for fertilization. We describe here the study of two brothers presenting with large-headed spermatozoa. Molecular analysis of the AURKC gene was carried out in two brothers presenting with a typical large headed spermatozoa phenotype. -
Aminoacyl-Trna Synthetase Deficiencies in Search of Common Themes
© American College of Medical Genetics and Genomics ARTICLE Aminoacyl-tRNA synthetase deficiencies in search of common themes Sabine A. Fuchs, MD, PhD1, Imre F. Schene, MD1, Gautam Kok, BSc1, Jurriaan M. Jansen, MSc1, Peter G. J. Nikkels, MD, PhD2, Koen L. I. van Gassen, PhD3, Suzanne W. J. Terheggen-Lagro, MD, PhD4, Saskia N. van der Crabben, MD, PhD5, Sanne E. Hoeks, MD6, Laetitia E. M. Niers, MD, PhD7, Nicole I. Wolf, MD, PhD8, Maaike C. de Vries, MD9, David A. Koolen, MD, PhD10, Roderick H. J. Houwen, MD, PhD11, Margot F. Mulder, MD, PhD12 and Peter M. van Hasselt, MD, PhD1 Purpose: Pathogenic variations in genes encoding aminoacyl- with unreported compound heterozygous pathogenic variations in tRNA synthetases (ARSs) are increasingly associated with human IARS, LARS, KARS, and QARS extended the common phenotype disease. Clinical features of autosomal recessive ARS deficiencies with lung disease, hypoalbuminemia, anemia, and renal tubulo- appear very diverse and without apparent logic. We searched for pathy. common clinical patterns to improve disease recognition, insight Conclusion: We propose a common clinical phenotype for recessive into pathophysiology, and clinical care. ARS deficiencies, resulting from insufficient aminoacylation activity Methods: Symptoms were analyzed in all patients with recessive to meet translational demand in specific organs or periods of life. ARS deficiencies reported in literature, supplemented with Assuming residual ARS activity, adequate protein/amino acid supply unreported patients evaluated in our hospital. seems essential instead of the traditional replacement of protein by Results: In literature, we identified 107 patients with AARS, glucose in patients with metabolic diseases. DARS, GARS, HARS, IARS, KARS, LARS, MARS, RARS, SARS, VARS, YARS, and QARS deficiencies. -

Need for National Regulation of Cryobanks
Citizen Petition January 1, 2017 The undersigned submits this petition under 10.20 and 10.30 of the Federal Food, Drug, and Cosmetic Act or the Public Health Service Act or any other statutory provision for which authority has been delegated to the Commissioner of Food and Drugs to request the Commissioner of Food and Drugs to issue regulations. A. Action Requested Because the FDA currently mandates minimal medical testing of sperm and egg donors (no other regulation exists), we request that the commissioner of the FDA look into the state of affairs surrounding the sperm donation industry, and then develop the appropriate and much needed regulation/oversight. B. Statement of Grounds Challenges Faced by Donor Conceived People and Their Families Show Need for National Regulation of CryobanKs Christina Mickle, Research Assistant for the Donor Sibling Registry with Wendy Kramer, Director and Co-Founder of the Donor Sibling Registry Introduction: Cryobanks give women and couples who were once not able to have a child, the opportunity to conceive - the ability to start or grow their own family. The great majority of sperm bank customers are LGBT people and single women procuring donor* gametes as a way to build their families [3], while a smaller percentage of sperm bank customers are infertile couples. According to the Center of Disease Control, impaired fecundity (the inability to have a child) affects 18% of men who have sought help for fertility (594,000- 846,000 men) [14]. Although not all want or require donor gametes, the need and desire for cryobanks continues to grow, and challenges in the field are becoming more apparent.