Hepatic Porphyrias (6-Aminolevulinate Synthase/Derepression/Induction/Coproporphyria) C
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Noncanonical Coproporphyrin-Dependent Bacterial Heme Biosynthesis Pathway That Does Not Use Protoporphyrin
Noncanonical coproporphyrin-dependent bacterial heme biosynthesis pathway that does not use protoporphyrin Harry A. Daileya,b,c,1, Svetlana Gerdesd, Tamara A. Daileya,b,c, Joseph S. Burcha, and John D. Phillipse aBiomedical and Health Sciences Institute and Departments of bMicrobiology and cBiochemistry and Molecular Biology, University of Georgia, Athens, GA 30602; dMathematics and Computer Science Division, Argonne National Laboratory, Argonne, IL 60439; and eDivision of Hematology, Department of Medicine, University of Utah School of Medicine, Salt Lake City, UT 84132 Edited by J. Clark Lagarias, University of California, Davis, CA, and approved January 12, 2015 (received for review August 25, 2014) It has been generally accepted that biosynthesis of protoheme of a “primitive” pathway in Desulfovibrio vulgaris (13). This path- (heme) uses a common set of core metabolic intermediates that way, named the “alternative heme biosynthesis” path (or ahb), has includes protoporphyrin. Herein, we show that the Actinobacteria now been characterized by Warren and coworkers (15) in sulfate- and Firmicutes (high-GC and low-GC Gram-positive bacteria) are reducing bacteria. In the ahb pathway, siroheme, synthesized unable to synthesize protoporphyrin. Instead, they oxidize copro- from uroporphyrinogen III, can be further metabolized by suc- porphyrinogen to coproporphyrin, insert ferrous iron to make Fe- cessive demethylation and decarboxylation to yield protoheme (14, coproporphyrin (coproheme), and then decarboxylate coproheme 15) (Fig. 1 and Fig. S1). A similar pathway exists for protoheme- to generate protoheme. This pathway is specified by three genes containing archaea (15, 16). named hemY, hemH, and hemQ. The analysis of 982 representa- Current gene annotations suggest that all enzymes for pro- tive prokaryotic genomes is consistent with this pathway being karyotic heme synthetic pathways are now identified. -

Liver Transplantation for the Management of Acute Intermittent
nd Gas y a tro g in lo t o e t s a t i p n Journal of Hepatology and e a l H D f i o s Kappus at al., J Hepatol Gastroint Dis 2017, 3:1 l o a r d ISSN:n 2475-3181 r e u r s o J Gastrointestinal Disorders DOI: 10.4172/2475-3181.1000141 Case Report Open Access Liver Transplantation for the Management of Acute Intermittent Porphyria: A Case Report Matthew R Kappus1, Bryant B Summers2, Jennifer S Byrns2*, Carl L Berg1 and Julius M Wilder1 1Division of Gastroenterology, Duke University School of Medicine, Durham NC, United States 2Department of Pharmacy, Duke University Hospital, Durham NC, United States *Corresponding author: Jennifer S Byrns, Department of Pharmacy, Duke University Hospital, DUMC BOX 3089, Durham, NC 27710, United States, Tel: 919-681-0677; E-mail: [email protected] Received date: December 27, 2016; Accepted date: January 16, 2017; Published date: January 20, 2017 Copyright: © 2017 Kappus MR, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract We report a single patient with acute intermittent porphyria whose porphyria was successfully treated with orthotopic liver transplantation. She had a very poor quality of life as a result of years of frequent acute porphyria symptoms manifesting as abdominal pain crises. After transplantation, clinical signs of porphyria resolved as expected. This case adds to a growing body of literature which is assisting to formulate the indications for, and the timing of, transplantation for AIP. -
Hereditary Corpoporphyria Presenting with Deep Jaundice and Photosensitivity
ANNALS OF GASTROENTEROLOGY 2001, 14(4):319-324 Case report Hereditary corpoporphyria presenting with deep jaundice and photosensitivity D. Kapetanos, P. Xiarhos, E. Kapetis1, A. Avgerinos, A. Ilias, G. Kokozidis, G. Kitis CASE REPORT SUMMARY A 20-year old woman was referred to our department Hereditary coproporphyria is a rare hepatic porphyria with from another hospital in May 2000, due to painless jaun- symptoms similar to acute intermittent porphyria. Photo- dice and pruritus. She reported having dark urine and sensitivity is not described in the latter. We report the case pale stools for two weeks and jaundice for 10 days be- of a young female with deep jaundice, photosensitivity, ane- fore admission. mia, renal failure and no abdominal pain. Hereditary co- proporphyria was diagnosed and the patient was discharged The patient had no past medical history, with no ne- after 111 days in full recovery. She was readmitted after 45 onatal jaundice, had received no medications during the days with abdominal pain and no jaundice or photosensi- previous months and had no alcohol consumption in the tivity. Severe neuropathy developed which caused tetrapare- past. She was on a diet in order to lose weight (her initial sis and deterioration of the respiratory muscle function. weight was 80 kg) and had been using home insecticides Haem arginate was administered with gradual improvement several days before. Her parents reported a family histo- of neuropathy. ry of thalassemia major. Key words: Hereditary corpoporphyria, jaundice, photosen- On admission she was icteric. She had 2-3 blisters on sitivity, neuropathy, haem arginate her face with serous yellow colored fluid. -

The Function of Pufq in the Regulation of Bacteriochlorophyll Biosynthesis in Rhodobacter Capsulatus
The Function of PufQ in the Regulation of Bacteriochlorophyll Biosynthesis in Rhodobacter capsulatus Himani Rajeshwar Utkhede B.Sc. Simon Fraser University, 200 1 THESIS SUBMITTED IN PARTIAL FULFILLMENT OF THE REQUIREMENTS OF THE DEGREE OF MASTER OF SCIENCE in the Department of Molecular Biology and Biochemistry O Himani R. Utkhede 2004 SIMON FRASER UNIVERSITY March, 2004 All rights reserved. This work may not be reproduced in whole or in part, by photocopy or other means, without permission of the author. Approval I Name: Himani R. Utkhede Degree: Master of Science Title of Thesis: The Function of PufQ in the Regulation of Bacteriochlorophyll Synthesis in Rhodobacter capsulatus. Examining Committee: Dr. W.S. Davidson, Chair Dr. William R. Richards, Senior Supervisor Professor Emeritus, Molecular Biology and Biochemistry Simon Fraser University Dr. Michel Leroux, Supervisor Assistzt Prcfessor, ?v!s!ec.dzr Eic!ca.;- - 2~2L3.icche~isty Simon Fraser University Dr. Erika Plettner, Supervisor Assistant Professor, Chemistry Simon Fraser University Dr. Lynne Quarmby, Internal Examiner Assistant Professor, Biology Simon Fraser University Date Approved: Partial Copyright Licence The author, whose copyright is declared on the title page of this work, has granted to Simon Fraser University the right to lend this thesis, project or extended essay to users of the Simon Fraser University Library, and to make partial or single copies only for such users or in response to a request from the library of any other university, or other educational institution, on its own behalf or for one of its users. The author has further agreed that permission for multiple copying of ths work for scholarly purposes may be granted by either the author or the Dean of Graduate Studies. -
Module 01: Classification of Porphyria
MODULE 01 Classification of Porphyria Do not reprint, reproduce, modify or distribute this material without the prior written permission of Alnylam Pharmaceuticals. © 20120199 Alnylam PharmaceuticalsPharmaceuticals,, Inc.Inc. All rights reserved. -USA-00001-092018 1 Porphyria—A Rare Disease of Clinical Consequence • Porphyria is a group of at least 8 metabolic disorders1,2 – Each subtype of porphyria involves a genetic defect in a heme biosynthesis pathway enzyme1,2 – The subtypes of porphyria are associated with distinct signs and symptoms in patient populations that can differ by gender and age1,3 • Prevalence of some subtypes of porphyria may be higher than generally assumed3 Estimated Prevalence of Most Common Subtypes of Porphyria1,4 Estimated Prevalence Based on European Subtype of Porphyria and US Data Porphyria cutanea tarda (PCT) 1/10,000 (EU)1 0.118-1/20,000 (EU)1,4 Acute intermittent porphyria (AIP) 5/100,000 (US)1 Erythropoietic protoporphyria (EPP) 1/50,000-75,000 (EU)1 1. Ramanujam V-MS, Anderson KE. Curr Protoc Hum Genet. 2015;86:17.20.1-17.20.26. 2. Puy H et al. Lancet. 2010;375:924-937. 3. Bissell DM et al. N Engl J Med. 2017;377:862-872. 4. Elder G et al. J Inherit Metab Dis. 2013;36:848-857. Do not reprint, reproduce, modify or distribute this material without the prior written permission of Alnylam Pharmaceuticals. © 2019 Alnylam Pharmaceuticals, Inc. All rights reserved. -USA-00001-092018 2 Classification of Porphyria Porphyria can be classified in 2 major ways1,2: 1 According to major physiological sites: liver or 2 According to major clinical manifestations1,2 bone marrow1,2 • Heme precursors originate in either the liver or Acute Versus Photocutaneous Porphyria bone marrow, which are the tissues most • Major clinical manifestations are either neurovisceral active in heme biosynthesis1,2 symptoms (eg, severe, diffuse abdominal pain) associated with acute exacerbations or cutaneous lesions resulting from phototoxicity1,2 • Acute hepatic porphyria may be somewhat of a misnomer since the clinical features may be prolonged and chronic3 1. -

Advances in Hematology
ADVANCES IN HEMATOLOGY Current Developments in the Management of Hematologic Disorders Hematology Section Editor: Craig M. Kessler, MD What Hematologists Need to Know About Acute Hepatic Porphyria Manisha Balwani, MD, MS Associate Professor Department of Genetics and Genomic Sciences Icahn School of Medicine at Mount Sinai New York, New York H&O What is porphyria? H&O How common is acute hepatic porphyria? MB The porphyrias encompass a group of inherited MB Based on estimates from Western Europe, the metabolic disorders that result from a deficiency of one of combined prevalence of the acute hepatic porphyrias the enzymes in the heme biosynthetic pathway. These are among the white population is approximately 1 in genetic disorders; they can be inherited in an autosomal 200,000. These disorders are more common in certain dominant or recessive X-linked pattern; or they may be parts of the world because of founder mutations. For sporadic, as with porphyria cutanea tarda. example, the carrier frequency of acute intermittent porphyria is much higher in the Scandinavian countries, H&O How many types of porphyria exist? and variegate porphyria is much more common in South Africa.1 MB There are 8 different kinds of porphyria. These may be Even where the incidence is high, symptoms related classified as hepatic or erythropoietic based on the primary to these disorders remain rare. In fact, most patients who site of accumulation of porphyrins, but more commonly inherit a genetic change do not manifest symptoms of the they are classified clinically as acute or cutaneous. The acute disorder—the disease remains latent in a vast majority of hepatic porphyrias include acute intermittent porphyria these patients. -

A Primitive Pathway of Porphyrin Biosynthesis and Enzymology in Desulfovibrio Vulgaris
Proc. Natl. Acad. Sci. USA Vol. 95, pp. 4853–4858, April 1998 Biochemistry A primitive pathway of porphyrin biosynthesis and enzymology in Desulfovibrio vulgaris TETSUO ISHIDA*, LING YU*, HIDEO AKUTSU†,KIYOSHI OZAWA†,SHOSUKE KAWANISHI‡,AKIRA SETO§, i TOSHIRO INUBUSHI¶, AND SEIYO SANO* Departments of *Biochemistry and §Microbiology and ¶Division of Biophysics, Molecular Neurobiology Research Center, Shiga University of Medical Science, Seta, Ohtsu, Shiga 520-21, Japan; †Department of Bioengineering, Faculty of Engineering, Yokohama National University, 156 Tokiwadai, Hodogaya-ku, Yokohama 240, Japan; and ‡Department of Public Health, Graduate School of Medicine, Kyoto University, Sakyou-ku, Kyoto 606, Japan Communicated by Rudi Schmid, University of California, San Francisco, CA, February 23, 1998 (received for review March 15, 1998) ABSTRACT Culture of Desulfovibrio vulgaris in a medium billion years ago (3). Therefore, it is important to establish the supplemented with 5-aminolevulinic acid and L-methionine- biosynthetic pathway of porphyrins in D. vulgaris, not only methyl-d3 resulted in the formation of porphyrins (sirohydro- from the biochemical point of view, but also from the view- chlorin, coproporphyrin III, and protoporphyrin IX) in which point of molecular evolution. In this paper, we describe a the methyl groups at the C-2 and C-7 positions were deuter- sequence of intermediates in the conversion of uroporphy- ated. A previously unknown hexacarboxylic acid was also rinogen III to coproporphyrinogen III and their stepwise isolated, and its structure was determined to be 12,18- enzymic conversion. didecarboxysirohydrochlorin by mass spectrometry and 1H NMR. These results indicate a primitive pathway of heme biosynthesis in D. vulgaris consisting of the following enzy- MATERIALS AND METHODS matic steps: (i) methylation of the C-2 and C-7 positions of Materials. -

A High Urinary Urobilinogen / Serum Total Bilirubin Ratio Reported in Abdominal Pain Patients Can Indicate Acute Hepatic Porphyria
A High Urinary Urobilinogen / Serum Total Bilirubin Ratio Reported in Abdominal Pain Patients Can Indicate Acute Hepatic Porphyria Chengyuan Song Shandong University Qilu Hospital Shaowei Sang Shandong University Qilu Hospital Yuan Liu ( [email protected] ) Shandong University Qilu Hospital https://orcid.org/0000-0003-4991-552X Research Keywords: acute hepatic porphyria, urinary urobilinogen, serum total bilirubin Posted Date: June 14th, 2021 DOI: https://doi.org/10.21203/rs.3.rs-587707/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 1/10 Abstract Background: Due to its variable symptoms and nonspecic laboratory test results during routine examinations, acute hepatic porphyria (AHP) has always been a diagnostic dilemma for physicians. Misdiagnoses, missed diagnoses, and inappropriate treatments are very common. Correct diagnosis mainly depends on the detection of a high urinary porphobilinogen (PBG) level, which is not a routine test performed in the clinic and highly relies on the physician’s awareness of AHP. Therefore, identifying a more convenient indicator for use during routine examinations is required to improve the diagnosis of AHP. Results: In the present study, we retrospectively analyzed laboratory examinations in 12 AHP patients and 100 patients with abdominal pain of other causes as the control groups between 2015 and 2021. Compared with the control groups, AHP patients showed a signicantly higher urinary urobilinogen level during the urinalysis (P < 0.05). However, we showed that the higher urobilinogen level was caused by a false- positive result due to a higher level of urine PBG in the AHP patients. Hence, we used serum total bilirubin, an upstream substance of urinary urobilinogen synthesis, for calibration. -

Acute Intermittent Porphyria: an Overview of Therapy Developments and Future Perspectives Focusing on Stabilisation of HMBS and Proteostasis Regulators
International Journal of Molecular Sciences Review Acute Intermittent Porphyria: An Overview of Therapy Developments and Future Perspectives Focusing on Stabilisation of HMBS and Proteostasis Regulators Helene J. Bustad 1 , Juha P. Kallio 1 , Marta Vorland 2, Valeria Fiorentino 3 , Sverre Sandberg 2,4, Caroline Schmitt 3,5, Aasne K. Aarsand 2,4,* and Aurora Martinez 1,* 1 Department of Biomedicine, University of Bergen, 5020 Bergen, Norway; [email protected] (H.J.B.); [email protected] (J.P.K.) 2 Norwegian Porphyria Centre (NAPOS), Department for Medical Biochemistry and Pharmacology, Haukeland University Hospital, 5021 Bergen, Norway; [email protected] (M.V.); [email protected] (S.S.) 3 INSERM U1149, Center for Research on Inflammation (CRI), Université de Paris, 75018 Paris, France; valeria.fi[email protected] (V.F.); [email protected] (C.S.) 4 Norwegian Organization for Quality Improvement of Laboratory Examinations (Noklus), Haraldsplass Deaconess Hospital, 5009 Bergen, Norway 5 Assistance Publique Hôpitaux de Paris (AP-HP), Centre Français des Porphyries, Hôpital Louis Mourier, 92700 Colombes, France * Correspondence: [email protected] (A.K.A.); [email protected] (A.M.) Abstract: Acute intermittent porphyria (AIP) is an autosomal dominant inherited disease with low clinical penetrance, caused by mutations in the hydroxymethylbilane synthase (HMBS) gene, which encodes the third enzyme in the haem biosynthesis pathway. In susceptible HMBS mutation carriers, triggering factors such as hormonal changes and commonly used drugs induce an overproduction Citation: Bustad, H.J.; Kallio, J.P.; and accumulation of toxic haem precursors in the liver. Clinically, this presents as acute attacks Vorland, M.; Fiorentino, V.; Sandberg, characterised by severe abdominal pain and a wide array of neurological and psychiatric symptoms, S.; Schmitt, C.; Aarsand, A.K.; and, in the long-term setting, the development of primary liver cancer, hypertension and kidney Martinez, A. -

Intrinsic Fluorescence of Protoporphyrin IX from Blood Samples Can Yield Information on the Growth of Prostate Tumours
J Fluoresc (2010) 20:1159–1165 DOI 10.1007/s10895-010-0662-9 ORIGINAL PAPER Intrinsic Fluorescence of Protoporphyrin IX from Blood Samples Can Yield Information on the Growth of Prostate Tumours Flávia Rodrigues de Oliveira Silva & Maria Helena Bellini & Vivian Regina Tristão & Nestor Schor & Nilson Dias Vieira Jr. & Lilia Coronato Courrol Received: 12 November 2009 /Accepted: 30 March 2010 /Published online: 24 April 2010 # Springer Science+Business Media, LLC 2010 Abstract Prostate cancer is one of the most common types in those with prostate cancer induced by inoculation of of cancer in men, and unfortunately many prostate tumours DU145 cells. A significant contrast between the blood of remain asymptomatic until they reach advanced stages. normal and cancer subjects could be established. Blood Diagnosis is typically performed through Prostate-Specific porphyrin fluorophore showed an enhancement on the Antigen (PSA) quantification, Digital Rectal Examination fluorescence band around 632 nm following tumour (DRE) and Transrectal Ultrasonography (TU). The antigen growth. Fluorescence detection has advantages over other (PSA) is secreted by all prostatic epithelial cells and not light-based investigation methods: high sensitivity, high exclusively by cancerous ones, so its concentration also speed and safety. However it does carry the drawback of increases in the presence of other prostatic diseases. DRE low specificity of detection. The extraction of blood and TU are not reliable for early detection, when porphyrin using acetone can solve this problem, since histological analysis of prostate tissue obtained from a optical excitation of further molecular species can be biopsy is necessary. In this context, fluorescence techniques excluded, and light scattering from blood samples is are very important for the diagnosis of cancer. -

Nomenclature of Tetrapyrroles
Pure & Appi. Chem. Vol.51, pp.2251—2304. 0033-4545/79/1101—2251 $02.00/0 Pergamon Press Ltd. 1979. Printed in Great Britain. PROVISIONAL INTERNATIONAL UNION OF PURE AND APPLIED CHEMISTRY and INTERNATIONAL UNION OF BIOCHEMISTRY JOINT COMMISSION ON BIOCHEMICAL NOMENCLATURE*t NOMENCLATURE OF TETRAPYRROLES (Recommendations, 1978) Prepared for publication by J. E. MERRITT and K. L. LOENING Comments on these proposals should be sent within 8 months of publication to the Secretary of the Commission: Dr. H. B. F. DIXON, Department of Biochemistry, University of Cambridge, Tennis Court Road, Cambridge CB2 1QW, UK. Comments from the viewpoint of languages other than English are encouraged. These may have special significance regarding the eventual publication in various countries of translations of the nomenclature finally approved by IUPAC-IUB. PROVISIONAL IUPAC—ITJB Joint Commission on Biochemical Nomenclature (JCBN), NOMENCLATUREOF TETRAPYRROLES (Recommendations 1978) CONTENTS Preface 2253 Introduction 2254 TP—O General considerations 2256 TP—l Fundamental Porphyrin Systems 1.1 Porphyrin ring system 1.2 Numbering 2257 1.3 Additional fused rings 1.4 Skeletal replacement 2258 1.5 Skeletal replacement of nitrogen atoms 2259 1.6Fused porphyrin replacement analogs 2260 1.7Systematic names for substituted porphyrins 2261 TP—2 Trivial names and locants for certain substituted porphyrins 2263 2.1 Trivial names and locants 2.2 Roman numeral type notation 2265 TP—3 Semisystematic porphyrin names 2266 3.1 Semisystematic names in substituted porphyrins 3.2 Subtractive nomenclature 2269 3.3 Combinations of substitutive and subtractive operations 3.4 Additional ring formation 2270 3.5 Skeletal replacement of substituted porphyrins 2271 TP—4 Reduced porphyrins including chlorins 4.1 Unsubstituted reduced porphyrins 4.2 Substituted reduced porphyrins. -
And Formation
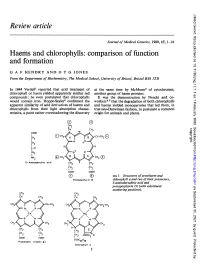
J Med Genet: first published as 10.1136/jmg.17.1.1 on 1 February 1980. Downloaded from Review article Journal of Medical Genetics, 1980, 17, 1-14 Haems and chlorophylls: comparison of function and formation G A F HENDRY AND 0 T G JONES From the Department ofBiochemistry, The Medical School, University ofBristol, Bristol BS8 ITD In 1844 Verdeill reported that acid treatment of at the same time by McMunn3 of cytochromes, chlorophyll or haem yielded apparently similar red another group of haem proteins. compounds; he even postulated that chlorophylls It was the demonstration by Nencki and co- would contain iron. Hoppe-Seyler2 confirmed the workers 45 that the degradation of both chlorophylls apparent similarity of acid derivatives of haems and and haems yielded monopyrroles that led them, in chlorophylls from their light absorption charac- true neo-Darwinian fashion, to postulate a common teristics, a point rather overshadowing the discovery origin for animals and plants. 0 0-'I CH2 II copyright. CH CH3 COOH CIH2 CH2 C-O CH2 http://jmg.bmj.com/ NH2 ( CH3' 'CH3 ® 5- Aminolaevulinic acid a CH2 2 1 12 2 CH2 )H COOH CD FIG 1 Structures ofprotohaem and Protoporphyrin IX chlorophyll a and two of their precursors, acid and 5-aminolaevulinic on September 30, 2021 by guest. Protected protoporphyrin IX (with substituent numbering positions). CH2 CH CH.--,j CH2 CH2 COOCH3 Protohoem (haem- b) CooC20H39 Chlorophyll a 1 J Med Genet: first published as 10.1136/jmg.17.1.1 on 1 February 1980. Downloaded from 2 G A F Hendry and 0 T G Jones Following the work ofWillstatter6 and Fischer and particularly those of avian egg shells, have no Stern,7 the structure of most natural and many central complexed metal.