Toxicological Profile for Glutaraldehyde, Draft for Public Comment Was Released in December 2015
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
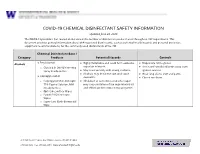
EH&S COVID-19 Chemical Disinfectant Safety Information
COVID-19 CHEMICAL DISINFECTANT SAFETY INFORMATION Updated June 24, 2020 The COVID-19 pandemic has caused an increase in the number of disinfection products used throughout UW departments. This document provides general information about EPA-registered disinfectants, such as potential health hazards and personal protective equipment recommendations, for the commonly used disinfectants at the UW. Chemical Disinfectant Base / Category Products Potential Hazards Controls ● Ethyl alcohol Highly flammable and could form explosive Disposable nitrile gloves Alcohols ● ● vapor/air mixtures. ● Use in well-ventilated areas away from o Clorox 4 in One Disinfecting Spray Ready-to-Use ● May react violently with strong oxidants. ignition sources ● Alcohols may de-fat the skin and cause ● Wear long sleeve shirt and pants ● Isopropyl alcohol dermatitis. ● Closed toe shoes o Isopropyl Alcohol Antiseptic ● Inhalation of concentrated alcohol vapor 75% Topical Solution, MM may cause irritation of the respiratory tract (Ready to Use) and effects on the central nervous system. o Opti-Cide Surface Wipes o Powell PII Disinfectant Wipes o Super Sani Cloth Germicidal Wipe 201 Hall Health Center, Box 354400, Seattle, WA 98195-4400 206.543.7262 ᅵ fax 206.543.3351ᅵ www.ehs.washington.edu ● Formaldehyde Formaldehyde in gas form is extremely Disposable nitrile gloves for Aldehydes ● ● flammable. It forms explosive mixtures with concentrations 10% or less ● Paraformaldehyde air. ● Medium or heavyweight nitrile, neoprene, ● Glutaraldehyde ● It should only be used in well-ventilated natural rubber, or PVC gloves for ● Ortho-phthalaldehyde (OPA) areas. concentrated solutions ● The chemicals are irritating, toxic to humans ● Protective clothing to minimize skin upon contact or inhalation of high contact concentrations. -

Comparison of Effectiveness Disinfection of 2%
ORIGINAL RESEARCH Journal of Dentomaxillofacial Science (J Dentomaxillofac Sci ) December 2018, Volume 3, Number 3: 169-171 P-ISSN.2503-0817, E-ISSN.2503-0825 Comparison of effectiveness disinfection of 2% Original Research glutaraldehyde and 4.8% chloroxylenol on tooth extraction instruments in the Department of Oral CrossMark http://dx.doi.org/10.15562/jdmfs.v3i2.794 Maxillofacial Surgery, Faculty of Dentistry, University of North Sumatera Month: December Ahyar Riza,* Isnandar, Indra B. Siregar, Bernard Volume No.: 3 Abstract Objective: To compare disinfecting effectiveness of 2% glutaraldehyde while the control group was treated with 4.8% chloroxylenol. Each Issue: 2 and 4.8% chloroxylenol on tooth extraction instruments at the instrument was pre-cleaned using a brush, water and soap for both Department of Oral Surgery, Faculty of Dentistry, University of North groups underwent the disinfection process. Sumatera. Results: The results were statistically analyzed using Mann-Whitney Material and Methods: This was an experimental study with post- Test. The comparison between glutaraldehyde and chloroxylenol First page No.: 147 test only control group design approach. Purposive technique is showed a significant difference to the total bacteria count on applied to collect samples which are lower molar extraction forceps. In instrument after disinfection (p=0.014 < 0.05). this study, sample were divided into 2 groups and each consisting of 18 Conclusion: 2% glutaraldehyde was more effective than 4.8% P-ISSN.2503-0817 instruments. The treatment group was treated with 2% glutaraldehyde chloroxylenol at disinfecting lower molar extraction forceps. Keyword: Disinfection, Glutaraldehyde, Chloroxylenol, Forceps E-ISSN.2503-0825 Cite this Article: Riza A, Siregar IB, Isnandar, Bernard. -

United States Patent Office Patiented Jan.5, 1963 2 Evaporation of the Solvent, to Leave Behind a Thin, De 3,073,794 Posited Film of the Polymer
3,073,794 United States Patent Office Patiented Jan.5, 1963 2 evaporation of the solvent, to leave behind a thin, de 3,073,794 posited film of the polymer. Basically, a suitable poly SPRAYABLE, ANHYDROUS SOLUTION OF -V. mer is a “1-vinyl-2-pyrrolidone polymer" and this is the NYL-2-PYRERODONE POLYMER IN CHELOR principal component. However, the term is also defined FLUORO HYDRO CARBON PROPELLANT George G. Stoner, Easton, Pa., assignor to General herewith to include not only the homopolymers but also a Aniline & Film Corporation, New York, N.Y., a corpor wide range of heteropolymers, copolymers, interpolymers, ration of Delaware terpolymers (three-component polymers) and, in general, No Drawing. Fied May 22, 1959, Ser. No. 814,999 polymers in which vinylpyrrollidone is either the sole com 6 (Cais. (CE. 260-33.8) ponent, a major component or a substantial component. O In the latter two instances the vinylpyrrollidone is copolym This invention relates to film-forming compositions, erized with such substances as vinyl acetate, isopropenyl and relates more particularly to sprayable film-forming acetate, vinyl laurate, vinyl stearate, vinyl oleate, vinyl compositions which are non-flammable and non-alcoholic benzoate, and other vinyl and isopropenyl esters; vinyl and which are eminently suitable for therapeutic pur chloride, 2-chloropropene, and other vinyl and isopropenyl poses. 5 halides; methyl vinyl ether, ethyl vinyl ether, isopropyl This application is a continuation-in-part of my ap vinyl ether, isobutyl vinyl ether, 2-ethoxyethyl vinyl ether, plication Serial No. 580,443, filed April 25, 1956 and now phenyl vinyl ether and other vinyl ethers; acrylic acid and abandoned. -
Phenol Health and Safety Guide
C - z_ IPCS INTERNATIONAL._ PROGRAMME ON CHEMICAL SAFETY OD 341 Health and Safety Guide No. 88 .P5 94 Ph c.2 PHENOL HEALTH AND SAFETY GUIDE ' UNITED NATIONS INTERNATIONAL ENVffiONMENTPROG~E LABOUR ORGANISATION WORLD HEALTH ORGANIZATION WORLD HEALTH ORGANIZATION, GENEVA 1994 1 I) 1\ ' ~Ii>cs Other HEALTH AND SAFETY GUIDES available: (continued on inside back cover) Acrolein (No . 67, 1992) Endrin (No. 60, 1991) Acrylamide (No. 45 , 1991) Epichlorohydrin (No. 8, 1987) Acrylonitrile (No. I, 1986) Ethylene oxide (No. 16, 1988) Aldicarb (No. 64, 1991) Fenitrothion (No. 65, 1991) Aldrin and dieldrin (No. 21 , 1988) Fenvalerate (No. 34, 1989) Allethrins (No. 24, 1989) Folpet (No. 72, 1992) Amitrole (No. 85 , 1994) Formaldehyde (No. 57, 1991) Ammonia (No. 37, 1990) Heptachlor (No. 14, 1988) Arsenic compounds, inorganic, other than Hexachlorobutadiene (No. 84, 1993) arsine (No. 70, 1992) Hexachlorocyclohexanes, alpha- and Atrazine (No. 47, 1990) beta- (No. 53, 1991) Barium (No. 46 , 1991) Hexachlorocyclopentadiene (No. 63 , 1991) Benomyl (No. 81, 1993) n-Hexane (No. 59, 1991) Bentazone (No. 48, 1990) Hydrazine (No. 56, 1991) Beryllium (No. 44, 1990) Isobenzan (No. 61 , 1991) !-Butanol (No. 3, 1987) Isobutanol (No. 9, 1987) 2-Butanol (No. 4, 1987) Kelevan (No. 2, 1987) ten-Butanol (No. 7, 1987) Lindane (No. 54 , 1991) Camphechlor (No. 40, 1990) Magnetic fields (No. 27, 1990) Captafol (No. 49, 1990) Methamidophos (No. 79, 1993) Captan (No. 50, 1990) Methyl bromide (Bromomethane) (No. 86, 1994) Carbaryl (No. 78, 1993) Methyl isobutyl ketone (No. 58, 1991) Carbendazim (No. 82, 1993) Methyl parathion (No. 75, 1992) Chlordane (No. 13 , 1988) Methylene chloride (No. -

Chemical Matricectomy with Phenol Versus Aesthetic Reconstruction. a Single Blinded Randomized Clinical Trial
Journal of Clinical Medicine Article The Treatment of Ingrown Nail: Chemical Matricectomy With Phenol Versus Aesthetic Reconstruction. A Single Blinded Randomized Clinical Trial Juan Manuel Muriel-Sánchez 1, Ricardo Becerro-de-Bengoa-Vallejo 2 , Pedro Montaño-Jiménez 1 and Manuel Coheña-Jiménez 1,* 1 Facultad de Enfermería, Fisioterapia y Podología, Universidad de Sevilla, 41009 Sevilla, Spain; [email protected] (J.M.M.-S.); [email protected] (P.M.-J.) 2 Facultad de Enfermería, Fisioterapia y Podología, Universidad Complutense de Madrid, 28040 Madrid, Spain; [email protected] * Correspondence: [email protected] Received: 29 January 2020; Accepted: 18 March 2020; Published: 20 March 2020 Abstract: Background: In onychocryptosis surgery, incisional and non-incisional matricectomy is indicated according to the stage. The chemical matricectomy with 88% phenol solution is the gold standard and a wedge resection is indicated for more advanced stages. The aesthetic reconstruction has the advantages of the incisional procedure without eponychium incisions and an effectiveness similar to the chemical matricectomy with phenol. Objective: To compare the recurrence and the healing time between the chemical matricectomy with phenol and the aesthetic reconstruction. Methods: A comparative, prospective, parallel, randomized, and one-blinded clinical trial was registered with the European Clinical Trials Database (EudraCT) with identification number 2019-001294-80. Thrity-four patients (56 feet) with 112 onychocryptosis were randomized in two groups. Thirty-six were treated with chemical matricectomy with phenol and 76 with aesthetic reconstruction. Each patient was blind to the surgical procedure assigned by the investigator. The primary outcome measurements were healing time and recurrence. The secondary outcome measurements were post-surgical bleeding, pain, inflammation, and infection rate. -

(12) Patent Application Publication (10) Pub. No.: US 2014/0004156A1 Mellstedt Et Al
US 2014.0004156A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2014/0004156A1 Mellstedt et al. (43) Pub. Date: Jan. 2, 2014 (54) BOLOGICAL INHIBITORS OF ROR1 Publication Classification CAPABLE OF INDUCING CELL, DEATH (51) Int. C. (76) Inventors: Hakan Mellstedt, Stockholm (SE): C07K 6/28 (2006.01) Hodjattallah Rabbani, Stockholm (SE); CI2N IS/II3 (2006.01) Ingrid Teige, Lund (SE) (52) U.S. C. CPC ............ C07K 16/28 (2013.01); CI2N 15/1138 (21) Appl. No.: 13/516,925 (2013.01) USPC ...... 424/400; 530/387.9; 536/24.5:536/23.1; (22) PCT Filed: Dec. 10, 2010 435/320.1; 435/325; 435/375; 424/139.1; (86). PCT No.: PCT/EP2010/007524 514/44. A:536/23.53; 435/331 S371 (c)(1), (57) ABSTRACT (2), (4) Date: Mar. 1, 2013 The invention relates to antibodies and siRNA molecules for (30) Foreign Application Priority Data inducing cell death by the specific binding of ROR1, domains thereof of nucleotide molecules encoding ROR1. There are Dec. 18, 2009 (GB) ................................... O922143.3 also provided methods involving and uses of the antibodies Jun. 3, 2010 (GB) ................................... 1OO93O7.8 and siRNA molecules of the invention. Patent Application Publication Jan. 2, 2014 Sheet 1 of 25 US 2014/0004156A1 L/S.*L/SdXL|-WLIXCRIO6] N Patent Application Publication Jan. 2, 2014 Sheet 2 of 25 US 2014/0004156A1 a bi-saw exit-8 ext: xx x: i. s: s x 8. : xxx xx . ex* x8. gri syst {{..} : twic s yxi-xxii. 33. 8 M. : : ised-east x 8. Patent Application Publication Jan. -

Chemical Reviews
Chemical Reviews Volume 84, Number 5 October 1984 Three-Carbon Homologating Agents JOHN C. STOWELL aaperhrsnf of chemlsbj'. ulhraslly 01 Flsw (Maam, Lake Fmt, New mns,LOUL&M 70148 Rscslvad NoVembsr 7, 1983 (Uevk4 MamcrW Receivad Juw, 27. 19W contents I. Introduction 409 11. Nucleophilic Reagents 410 A. Reagents Providing Functknal Chains wlth 410 Saturated a-. 8-. and y-Carbons 1. Ethers and Alcohols 410 2. Amines 41 1 3. Bromldes 41 1 4. Propionaldehyde Homoenolate 413 Equivalents 5. Propionate Homenolate Equivalents 419 E. Reagents Rovidlng the Terminal Acetylene 421 Function C. Reagents Rovldlng a.@-Unsatuated 422 Functionality 1. Allylic Alcohols and Halides 422 2. a,@-UnsaturatedAldehydes 422 3. a,@-UnsaturatedCarboxylic Aclds. 424 John C. Stowel was bom in Passaic. NJ. in 1938. and received Esters, and Lactones hls B.S. degee h chemlsby from Rutgers UnivmW in 1960. Hls D. Reagents Providing a.@-Acetylenk 425 W.D. wee in Qganlc chemistry was granted by Massachusetts Functionality Insmule of Tedrmqly h 1964 where he waked WMDr. Frm 1. a.@-Acatylenk Alcohols 425 D. Greene on freeradical termination reactions and prepared the first diaziridinone. He pined the Central Research division of 3M 2. a,@-AcetylenicAldehydes 426 Company in St. Paul. MN. for 4 years. In 1969 he became a 3. a,@-Acetylenic Carboxylic Aclds and 426 postdoctoral fellow at The Ohio State University with Dr. Leo A. Esters Paquette. He prepared and sWIW various (CH),, and benzo (CH),, E. Reagents providing B.yUnsahmted 426 cwnpounds including Umrmal and sihw-catalyred rearrangements. Functionality In 1970 he jokd the faculty of me University of New Ohms. -
Guidance Document Peroxide-Forming Chemicals
Guidance Document Peroxide-Forming Chemicals Some chemicals can form peroxides under normal storage conditions. Some of the peroxide chemicals are unstable, especially when dried or concentrated, and can explode violently when subjected to heat, light or mechanical shock. In addition, some of the inadvertently formed peroxides can initiate other unexpected violent reactions (e.g. polymerizations) with other chemicals. When possible and practical for your work, purchase chemicals that have inhibitors added by the manufacturer. Label peroxide-forming chemicals with date received and date opened. Store peroxide-formers in airtight opaque containers with screw caps. Consider oxygen exclusion methods such as purging with inert gas or sealing containers with parafilm. Inspect containers for signs of peroxide formation. Do not open a container which has crystals or a visible cloudiness. Call EHS to come remove it. The friction caused by opening a lid can cause an explosion. Liquids can be tested for presence of peroxide. This is especially important prior to distilation. Most explosions of peroxide forming chemicals occur when a material is distilled to dryness. Peroxide test kits are available from chemical vendors. Contact EHS for additional guidance. Classification Table for Peroxide-Forming Chemicals Class I:: Unsaturated materials, especially those of low molecular weight, may polymerize violently and hazardously due to peroxide initiation. These chemicals can spontaneously decompose, becoming explosive after exposure to air with concentration. Discard unopened containers within 3 months. Opened containers should be tested for peroxides every 2 months. Acrylic acid Tetrafluoroethylene Acrylonitrile Vinyl acetate 1,3-Butadiene Vinyl acetylene Chlorobutadiene (chloroprene) Vinyl chloride Chlorotrifluoroethylene Vinyl pyridine Methyl methacrylate Vinylidiene chloride Styrene Class II: The following chemicals are a peroxide hazard upon concentration (distillation/evaporation). -

Partial Nail Avulsion and Chemical Matricectomy: Ingrown Toenails
Partial nail avulsion and chemical matricectomy: Ingrown toenails Intervention Removal (avulsion) of an ingrowing section of toenail and application of a caustic chemical to destroy the nail matrix (matricectomy). Indication Partial nail avulsion and chemical matricectomy relieve symptoms and prevent regrowth of the nail edge or recurrence of the ingrowing toenail. Possible causes of ingrowing toenails include improper Ingrowing toenails are a common problem and occur when the edge of the nail grows trimming of the nail, tearing nail into flesh at the side of the nail, causing a painful injury. The punctured skin can become off, overly curved nail, certain inflamed and infected. Ingrown toenails can be classified into three stages (see Figure 1): activities (eg running) and • mild (or Stage I) wearing constricting footwear. – oedema, erythema and pain • moderate (or Stage II) – inflammation and inflection with or without purulent discharge, in addition to the symptoms of Stage I • severe (or Stage III) – chronic inflammation, epithelialised hypertrophic granulation tissue. Figure 1. Three stages of ingrown toenails Source: Eekhof JA, Van Wijk B, Knuistingh Neven A, van der Wouden JC. Interventions for ingrowing toenails. The Cochrane Database of Systematic Reviews 2012;4:CD001541. Surgical interventions are commonly performed for patients in Stages II and III, and are more effective than non-surgical interventions in preventing the recurrence of an ingrowing toenail. The addition of chemical cauterisation (most commonly with phenol) at Stages II and III, may be more effective in preventing recurrence and regrowth of the ingrowing toenail than surgery alone. Contraindications Diminished vascular supply to the digit is a relative contraindication to nail surgery. -

Hatchery Disinfection Policy and Procedures
MAINE DEPARTMENT OF INLAND FISHERIES & WILDLIFE Chapter 11 Disinfection Policy & Procedures Editors: David C. Rayner, Fish Culture Supervisor, Governor Hill State Fish Hatchery, Augusta, Maine (19XX- Present) & G. Russell Danner MS, DVM, Fish Pathologist, Fish Health Laboratory, Augusta, Maine (1998 – Present) Date: September 24, 1999. “Or if a person touches anything ceremonially unclean-whether the carcasses of unclean wild animals or of unclean livestock or of unclean creatures that move along the ground-even though he is unaware of it, he has become unclean and is guilty” Lev. 5:2 Several factors should be included in an evaluation of a disinfectant. A prerequisite for a disinfectant is its effectiveness against the expected spectrum of pathogens (Table 11- 1, 11-2, and 11-3). A general guideline for effective killing of pathogens by a disinfectant is a 5-log killing of bacteria and a 4-log killing of viruses. In addition to the activity of the disinfectant, its compatibility with devices should be reviewed in detail; this should include a review of data on devices that have been immersed for longer than recommended times. Instruments can be forgotten after immersion, and this mistake should not necessarily result in irreparable damage to the device. Other issues are toxicity, odor, compatibility with other compounds, and residual activity. Various and numerous organisms can cause diseases in fish. Viruses, bacteria, fungi, protozoan and many invertebrate animals are included in this list. No single disinfectant destroys them all. It is up to the applicant to decide what is the pathogen of most concern, and how it is to be reduced or eliminated. -

Chemical Disinfectants | Disinfection & Sterilization Guidelines | Guidelines Library | Infection Control | CDC 3/19/20, 14:52
Chemical Disinfectants | Disinfection & Sterilization Guidelines | Guidelines Library | Infection Control | CDC 3/19/20, 14:52 Infection Control Chemical Disinfectants Guideline for Disinfection and Sterilization in Healthcare Facilities (2008) Alcohol Overview. In the healthcare setting, “alcohol” refers to two water-soluble chemical compounds—ethyl alcohol and isopropyl alcohol —that have generally underrated germicidal characteristics 482. FDA has not cleared any liquid chemical sterilant or high- level disinfectant with alcohol as the main active ingredient. These alcohols are rapidly bactericidal rather than bacteriostatic against vegetative forms of bacteria; they also are tuberculocidal, fungicidal, and virucidal but do not destroy bacterial spores. Their cidal activity drops sharply when diluted below 50% concentration, and the optimum bactericidal concentration is 60%–90% solutions in water (volume/volume) 483, 484. Mode of Action. The most feasible explanation for the antimicrobial action of alcohol is denaturation of proteins. This mechanism is supported by the observation that absolute ethyl alcohol, a dehydrating agent, is less bactericidal than mixtures of alcohol and water because proteins are denatured more quickly in the presence of water 484, 485. Protein denaturation also is consistent with observations that alcohol destroys the dehydrogenases of Escherichia coli 486, and that ethyl alcohol increases the lag phase of Enterobacter aerogenes 487 and that the lag phase e!ect could be reversed by adding certain amino acids. The bacteriostatic action was believed caused by inhibition of the production of metabolites essential for rapid cell division. Microbicidal Activity. Methyl alcohol (methanol) has the weakest bactericidal action of the alcohols and thus seldom is used in healthcare 488. The bactericidal activity of various concentrations of ethyl alcohol (ethanol) was examined against a variety of microorganisms in exposure periods ranging from 10 seconds to 1 hour 483. -

Guideline for Disinfection and Sterilization in Healthcare Facilities, 2008
Guideline for Disinfection and Sterilization in Healthcare Facilities, 2008 Guideline for Disinfection and Sterilization in Healthcare Facilities, 2008 William A. Rutala, Ph.D., M.P.H.1,2, David J. Weber, M.D., M.P.H.1,2, and the Healthcare Infection Control Practices Advisory Committee (HICPAC)3 1Hospital Epidemiology University of North Carolina Health Care System Chapel Hill, NC 27514 2Division of Infectious Diseases University of North Carolina School of Medicine Chapel Hill, NC 27599-7030 1 Guideline for Disinfection and Sterilization in Healthcare Facilities, 2008 3HICPAC Members Robert A. Weinstein, MD (Chair) Cook County Hospital Chicago, IL Jane D. Siegel, MD (Co-Chair) University of Texas Southwestern Medical Center Dallas, TX Michele L. Pearson, MD (Executive Secretary) Centers for Disease Control and Prevention Atlanta, GA Raymond Y.W. Chinn, MD Sharp Memorial Hospital San Diego, CA Alfred DeMaria, Jr, MD Massachusetts Department of Public Health Jamaica Plain, MA James T. Lee, MD, PhD University of Minnesota Minneapolis, MN William A. Rutala, PhD, MPH University of North Carolina Health Care System Chapel Hill, NC William E. Scheckler, MD University of Wisconsin Madison, WI Beth H. Stover, RN Kosair Children’s Hospital Louisville, KY Marjorie A. Underwood, RN, BSN CIC Mt. Diablo Medical Center Concord, CA This guideline discusses use of products by healthcare personnel in healthcare settings such as hospitals, ambulatory care and home care; the recommendations are not intended for consumer use of the products discussed. 2