1. Introduction
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
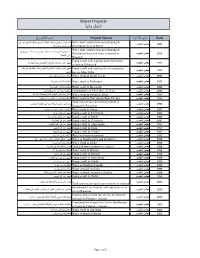
Water Projects ﻣﺎﺋﯾﺔ أﺷﻐﺎل
Water Projects أشغال مائية Date إٍسم اﻹدارة Project Name إسم المشروع & Water tank construction and pumping بناء خزان ارضي وتمديد شبكات توزيع وخطوط دفع وجر في 1997 مجلس الجنوب distribution lines in Dweir قرى الدوير وجوارها Water tank construction and pumping & بناء خزان علوي وتمديد خطوط دفع وجر وشبكات توزيع في 1995 مجلس الجنوب distribution lines and water networks in وادي النبطية Nabatieh Equip a well with a pump and chlorination 1997 مجلس الجنوب تجهيز البئر بمعدات الضخ والتعقيم في بلدة الهبارية system in Hebariyeh Equip a well and construction of a pumping تجهيز البئر بمعدات الضخ والتعقيم وانشاء خط دفع في بلدة 1997 مجلس الجنوب line in Jabin Town الجبين 1995 مجلس الجنوب Water work in Majdl Selem اشغال مائية في مجدل سلم 1995 مجلس الجنوب Water work in Mahrouna اشغال مائية في محرونة 1995 مجلس الجنوب Water work in Baysarieh اشغال مائية في البيسارية 1995 مجلس الجنوب Continuation of Fakherdine Velley's استكمال مياه آبار وادي فخرالين 1995 مجلس الجنوب Water work in Nabatieh Tahta اشغال مائية في النبطية التحتا )محدلة الدباغة( 1996 مجلس الجنوب Water work in Deir Anoun Rass EL Ain اشغال مائية في دير قانون رأس العين Tank construction and water network in 1996 مجلس الجنوب بناء قصر مائي وشبكة مائية في قعقعية الصنوبر Qaaqayieh Sanawbar 1997 مجلس الجنوب Water work in Dweir اشغال مائية في الدوير وجوارها 1997 مجلس الجنوب Equip a well in Teir Harfa تجهيز بئر طير حرفا 1997 مجلس الجنوب Equip a well in Debel تجهيز بئر وخط دفع في دبل 1997 مجلس الجنوب Equip a well in Hebariyeh تجهيز بئر في الهبارية 1997 مجلس الجنوب Equip a well in Alma shaab تجهيز بئر في علما -

Swiss Solidar Needs Assessment Report Nabatieh
Swiss Solidar Needs Assessment Report Nabatieh and Jezzine Districts, Southern Lebanon 12 – 16 August 2013 Photo: Meeting with a group of refugees in Doueir municipality, Nabatieh District A – Methodology Swiss Solidar undertook a multi-sectoral needs assessment in August 2013 to assess the humanitarian needs of Syrian refugees residing in Nabatieh and Jezzine Districts in Southern Lebanon.1 Prior to undertaking its field assessment, Solidar undertook a detailed documentation review, including other recent needs assessment reports, strategy documents, NGO position papers and relevant standards. Based on feedback we received from other agencies, UNHCR and government sources, Solidar identified potential gaps in the provision of Shelter, WASH, Protection and Non Food Item (particularly winterisation) assistance in Nabatieh and Jezzine governorates in South Lebanon. A reconnaissance visit to Nabatieh to meet with the Head of the Union of Municipalities and two Heads of Municipalities was then undertaken on 25 July 2013 to confirm the need for Solidar to extend its operations to these locations. Feedback from these meetings demonstrated that there were indeed significant gaps in the assistance being provided to refugees, and Solidar made plans for a more detailed needs assessment. The assessment was undertaken over 5 days from 12-16 August 2013. In addition to Nabatieh, Solidar also included Jezzine District in the assessment as, although there were lower numbers of refugees, the extent of formal assistance was very low. The purpose of the assessment was to assess the situation of Syrian refugees in relation to shelter, livelihoods, WASH, winterisation and protection. Three teams from the local area were recruited and trained for the assessment, overseen by an Assessment Coordinator. -

Expanded Programme of Immunization Study
Expanded Programme on Immunization 2016 Expanded Programme on Immunization District-Based Immunization Coverage Cluster Survey 1 Expanded Programme on Immunization 2016 Acknowledgment Special acknowledgment goes to the Director General of the Ministry of Public Health, Dr. Walid Ammar for his guidance, and Dr Randa Hamadeh, head of the Primary Health Care department for facilitating the process of the study. Particular thanks goes to Dr. Gabriele Riedner, WHO Representative in Lebanon Country Office, for her unconditional support and Dr. Alissar Rady for her technical guidance all through the design and implementation process, and the country office team as well as the team at WHO Regional Office. The Expanded Programme on Immunization, district-based immunization coverage cluster survey, would not have been possible without the generous financial support of Bill & Melinda Gates Foundation through the World Health Organization. This EPI cluster survey was conducted by the Connecting Research to Development center, contracted by and under the guidance of WHO and with the overall supervision of the MOPH team. 2 Expanded Programme on Immunization 2016 TABLE OF CONTENTS Acronyms and Abbreviations .......................................................................................................... 5 List of Tables ........................................................................................................................................... 6 List of Figures......................................................................................................................................... -
D D D L'8:L D
Submission Form To The Lebanon Recovery Fund Steering Committee To be completed by the UN Resident Coordinator's Office (RCO) Meeting No: Date of Meeting: Item No: Programme/project: (To be completed by the Participating UN Organisation and endorsed by SC) To: Lebanon Recovery Fund Steering Date of Submission: 29 November 2011 Committee From: Lebanese Family Planning Contact: Toufic Osseiran, Honorary President, Association I UN Women Rania Tarazi, Assistant Regional Program Director Through: Project Advisory Group (PAG) Contact: Toufic Osseiran, tel 961 1 311978, email: [email protected] D Endorsement Rania Tarazi, tel. +962 6 5200060 ext. 1008, email: D Comments [email protected] Proposed submission, if approved would Proposed submission resulted from: result in: D National Authorities initiative within national D Continuation of existing priorities programme/project D UN Agency initiative within national priorities l'8:l New programme/project l'8:] Other (explain): Joint initiative between LFPA D Other (explain) and UN Women within national priorities Project title: Local Development through Women Empowerment- in Nabatieh Villages Amount of funds requested for proposed programme/project: $ 698,340 Estimated number of beneficiaries: direct 6,604 indirect approximately 90,000 people and 35 organizations Percentage and amount of indirect costs requested: 7% Background The project was jointly developed by UN Women and the Lebanese Family Planning Association (LFPA). UN Women, an non-resident agency in Lebanon, conducted a gender needs assessment in April 2011 to identify entry points for its technical support to national organizations within its mandate of gender equality. In addition to identifying potential partners, the gender needs assessment has shown that women have not been systematically included in the recovery and reconstruction efforts in Lebanon. -
Lebanon National Operations Room Daily Report on COVID-19
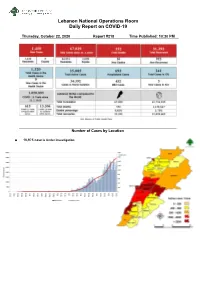
Lebanon National Operations Room Daily Report on COVID-19 Thursday, October 22, 2020 Report #218 Time Published: 10:30 PM Number of Cases by Location • 10,975 case is Under investigation Beirut 60 Chouf 43 Kesrwen 98 Matn 151 Ashrafieh 9 Anout 1 Ashkout 1 Ein Alaq 1 Ein Al Mreisseh 1 Barja 6 Ajaltoun 2 Ein Aar 1 Basta Al Fawka 1 Barouk 1 Oqaybeh 1 Antelias 3 Borj Abi Haidar 2 Baqaata 1 Aramoun 1 Baabdat 3 Hamra 1 Chhim 6 Adra & Ether 1 Bouchrieh 1 Mar Elias 3 Damour 1 Adma 1 Beit Shabab 2 Mazraa 3 Jiyyeh 2 Adonis 3 Beit Mery 1 Mseitbeh 2 Ketermaya 2 Aintoura 1 Bekfaya 2 Raouche 1 Naameh 5 Ballouneh 3 Borj Hammoud 9 Ras Beirut 1 Niha 3 Fatqa 1 Bqennaya 1 Sanayeh 2 Wady Al Zayne 1 Bouar 2 Broummana 2 Tallet El Drouz 1 Werdanieh 1 Ghazir 3 Bsalim 1 Tallet Al Khayat 1 Rmeileh 1 Ghbaleh 1 Bteghrine 1 Tariq Jdeedeh 4 Saadiyat 1 Ghodras 2 Byaqout 1 Zarif 1 Sibline 1 Ghosta 3 Dbayyeh 3 Others 27 Zaarourieh 1 Hrajel 1 Dekwene 12 Baabda 101 Others 9 Ghadir 2 Dhour Shweir 1 Ein El Rimmaneh 8 Hasbaya 6 Haret Sakher 6 Deek Al Mahdy 2 Baabda 4 Hasbaya 1 Kaslik 3 Fanar 4 Bir Hassan 1 Others 5 Sahel Alma 7 Horch Tabet 1 Borj Al Brajneh 17 Byblos 25 Sarba 5 Jal El Dib 3 Botchay 1 Blat 1 Kfardebian 1 Jdeidet El Metn 2 Chiah 6 Halat 1 Kfarhbab 1 Mansourieh 2 Forn Al Shebbak 3 Jeddayel 1 Kfour 3 Aoukar 3 Ghobeiry 3 Monsef 1 Qlei'aat 1 Mazraet Yashouh 3 Hadat 12 Ras Osta 1 Raasheen 2 Monteverde 2 Haret Hreik 5 Others 20 Safra 2 Mteileb 3 Hazmieh 4 Jezzine 12 Sehaileh 1 Nabay 1 Loueizy 1 Baysour 1 Tabarja 6 Naqqash 3 Jnah 2 Ein Majdoleen 1 Zouk Michael 1 Qanbt -

Syria Refugee Response
SYRIA REFUGEE RESPONSE Distribution of MoPH network and UNHCR Health Brochure Selected PHC as of 6 October, 2016 Akkar Governorate, Akkar District - Number of syrian refugees : 99,048 Legend !( Moph Network Moph Network !< and UNHCR Dayret Nahr Health El-Kabir 1,439 Brochure ") UNHCR Health Brochure Machta Hammoud Non under 2,246 MoPH network 30221 ! or under 30123 35516_31_001 35249_31_001 IMC No partner Wadi Khaled health center UNHCR Health Al Aaboudiyeh Governmental center !< AAridet Sammaqiye !( 713 Aaouaainat Khalsa Brochure Cheikh Hokr Hokr Dibbabiye Aakkar 1 30216 Zennad Jouret Janine Ed-Dahri 67 Kfar 6 35512_31_001 6 Srar 13 !( Aamayer Kharnoubet Noun No partner 13,361 Barcha Khirbet Er Aakkar 8 Alaaransa charity center Most Vulnerable Massaaoudiye 7 Aarme Mounjez Remmane 386 Noura ! 29 25 13 Qachlaq Et-Tahta 35512-40-01 Localities Tall Chir 28 17 Hmayra No partner Cheikh Kneisset Hmairine Aamaret Fraydes ! 105 1,317 Srar Aakkar Cheikhlar Wadi Khaled SDC Qarha Zennad Aakkar Tall El-Baykat 108 7 Rmah 62 Aandqet !< Aakkar 257 Mighraq 33 Bire 462 Most Mzeihme Ouadi 49 401 17 44 Aakkar 11 El-Haour Kouachra 168 Baghdadi Vulnerable Haytla 636 1,780 Qsair Hnaider 30226 !( Darine 10 Aamriyet Aakkar 1,002 35229_31_001 124 Aakkar 35 Mazraat 2nd Most No partner Tall Aabbas Saadine Alkaram charity center - Massoudieh Ech-Charqi 566 En-Nahriye Kneisset Tleil Barde 958 878 Hnaider Vulnerable !< 798 35416-40-01 4 Ghazayle 1,502 30122 38 No partner ! 35231_31_001 Bire Qleiaat Aain Ez-Zeit Kafr Khirbet ")!( IMC Aain 3rd Most Aakkar Hayssa Saidnaya -

Lebanon National Operations Room Daily Report on COVID-19
Lebanon National Operations Room Daily Report on COVID-19 Monday, October 05, 2020 Report #201 Time Published: 11:30 PM New: 9 isolation centers that have been equipped in various Lebanese regions host 99 positive cases. More information about the locations of isolation centers and their occupancy rate is available on the link http://bit.ly/DRM-IsolationCentersProfiles Number of Cases by Location • 8,387 case is Under investigation Beirut 98 Chouf 48 Kesrwen 81 Matn 185 Ein El Mreisseh 2 Damour 2 Kaslik 2 Borj Hammoud 14 Ras Beirut 3 Mazboud 1 Zouk Michael 12 Nabaa 2 Qreitem 3 Ketermaya 1 Nahr El Kalb 1 Sin El Fil 10 Raouche 4 Siblin 1 Haret El Meer 1 Horsh Tabet 3 Hamra 12 Barja 6 Ghadir 6 Jesr El Basha 1 Mseitbeh 5 Ein El Hor 1 Zouk Mosbeh 7 Jdeidet El Metn 9 Wata El Mseitbeh 1 Jiyyeh 1 Adonis 7 Bouchrieh 3 Mar Elias 2 Wady El Zayneh 2 Haret Sakher 3 Dora 7 Zarif 2 Deir El Qamar 1 Sahel Alma 3 Rawda 1 Mazraa 8 Semqanieh 4 Kfar Yassine 1 Sabtieh 8 Borj Abi Haidar 3 Maaser Beit El Deen 1 Tabarja 4 Dekwene 18 Basta Fawka 3 Warhanieh 3 Adma & Dafneh 1 Antelias 10 Tariq Jdideh 13 Freidees 2 Safra 3 Jal El Dib 9 Ras El Nabee 10 Baaqleen 6 Oqaybeh 2 Naqqash 2 Basta Tahta 1 Jahlieh 1 Ajaltoun 3 Zalka 5 Mar Mkhael El Nahr 3 Botmeh 1 Ballouneh 1 Byaqout 5 Rmeil 1 Baqaata 2 Sehaileh 2 Dbayyeh 3 Ashrafieh 17 Niha 1 Darayya 1 Mansouriyye 3 Others 5 Khreibeh 1 Ein EL Rihaneh 1 Dayshouniyeh 1 Baabda 127 Bater 1 Ghazir 2 Fanar 9 Chiah 10 Others 9 Kfar Hbab 2 Ein Saadeh 14 Jnah 1 Aley 48 Bayader BorjFtouh 1 Bsalim 4 Ouzai 2 El Amroussieh 2 Chnaniir -
Lebanon National Operations Room Daily Report on COVID-19
Lebanon National Operations Room Daily Report on COVID-19 Wednesday, October 07, 2020 Report #203 Time Published: 11:30 PM New in the report: - Recommendations issued by the meeting of the Committee for Follow-up of Preventive Measures and Procedures to Confront the Coronavirus on 7/10/2020 Number of Cases by Location • 8,812 case is Under investigation Beirut 96 Kesrwen 72 Akkar 33 Matn 188 Ras Beirut 2 Sarba 3 Halba 2 Borj Hammoud 14 Manara 1 Kaslik 1 Majdel Akkar 1 Nabaa 1 Qreitem 1 Zouk Michael 8 Menyara 2 Sin El Fil 8 Raouche 2 Ghadir 6 Zouk Al Habalsa 2 Horch Tabet 2 Hamra 8 Zouk Mosbeh 5 Bayno 1 Jdeidet El Metn 13 Mseitbeh 7 Adonis 3 Akkar Al Atika 2 Bouchrieh 5 Mar Elias 7 Haret Sakher 1 Ballanet Al Haysa 1 Dora 4 Sanayeh 1 Sahel Alma 2 Masoudieh 1 Rawda 6 Zarif 3 Tabarja 3 Bebnin 2 Sabtieh 6 Qantary 1 Adma & Dafneh 1 Khan Al Hayat 1 Deir Roukoz 1 Mazraa 6 Safra 3 Qebeet 1 Dekweneh 17 Malaab Baladi 1 Bouar 1 Beit Ayyoub 1 Mkalles 1 Tariq Jdeedeh 11 Oqaybeh 2 Jdeidet Al Qaytaa 1 Antelias 18 Ras Nabaa 2 Ajaltoun 2 Meshmesh 2 Jal El Dib 5 Basta Tahta 1 Ballouneh 1 Fneidek 5 Naqqash 9 Gemmayzeh 2 Sehaileh 3 Majdala 2 Zalka 6 Jeitawy 2 Jeita 2 Rahbe 1 Byaqout 2 Mar Michael Al Nahr 1 Ghazir 1 Beereh 1 Dbayyeh 8 Rmeil 2 Ghosta 1 Tleel 1 Mazraet Aoukar 1 Ashrafieh 21 Maarab 2 Qbayyat 1 Mansourieh 8 Forn Al Hayek 1 Maaysra 1 Qobayyat 1 Fanar 7 Others 13 Reifoun 2 Others 1 Ein Saadeh 1 Baabda 162 Qleiaat 3 Zahle 166 Bqannaya 1 Chiah 16 Ashkout 3 Maydan 1 Bsalim 4 Jnah 3 Feitroun 1 Rassieh 2 Mteileb 2 Medwar 1 Kfardebian 2 Maallaqa 3 Rabieh -
IMPLEMENTATION COMPLETION REPORT (ICR) Lebanon
Document of The World Bank Public Disclosure Authorized Report No: ICR00001141 IMPLEMENTATION COMPLETION AND RESULTS REPORT (IBRD-70260 LE) ON A Public Disclosure Authorized LOAN IN THE AMOUNT OF US$80.00 MILLION TO THE LEBANESE REPUBLIC FOR A FIRST MUNICIPAL INFRASTRUCTURE PROJECT Public Disclosure Authorized June 1, 2009 Sustainable Development Department Public Disclosure Authorized Middle East Country Department Middle East and North Africa Region CURRENCY EQUIVALENTS (Exchange Rate Effective June 1, 2009) Currency Unit = LP LP 1,500 = US$1 FISCAL YEAR ABBREVIATIONS AND ACRONYMS Vice President: Daniela Gressani Country Director: Hedi Larbi Sector Manager: Anna M. Bjerde Project Team Leader: Robert Maurer ICR Team Leader: Robert Maurer Lebanon First Municipal Infrastructure Project CONTENTS Data Sheet A. Basic Information ……………………………………………………….…….………i B. Key Dates …..………………………………………………………………..………..i C. Ratings Summary ……………………………………………………………….…….i D. Sector and Theme Codes ……………...………………………………………….….ii E. Bank Staff ………………………………….…………………………………..……..ii F. Results Framework Analysis………..………………………….………………….….ii G. Ratings of Project Performance in ISRs .………………………………………….….v H. Restructuring …………………………………………………………………….v I. Disbursement Graph ………………………………………………………...….vi 1. Project Context, Development Objectives and Design ……………………………… 1 2. Key Factors Affecting Implementation and Outcomes……………………………… 4 3. Assessment of Outcomes ..…………………………………………………..……… .8 4. Assessment of Risk to Development Outcome …………………………………. 11 5. Assessment of -
Development of Mapping of Living in Lebanon 1995-2004 UNDP
Republic of Lebanon Ministry of Social Affairs Development of Mapping Of Living in Lebanon 1995 2004 A Comparison with the Results of "Mapping of Living Conditions in Lebanon, 1998" Development of Mapping of Living Conditions in Lebanon, 1995‐2004: A Comparison with the Results of "Mapping of Living Conditions in Lebanon, 1998" Cover and book design: Penguin Cube Email: [email protected] Printed by: Dar Al‐Kotob Email: [email protected] Copyright and publishing rights 2007 All rights reserved for the "Capacity Building for Poverty Reduction” joint project between MOSA and UNDP Table of Contents Introduction ....................................................................................................................................... 10 Acknowledgements ............................................................................................................................ 12 Foreword ............................................................................................................................................ 13 1‐ Methodological Introduction ......................................................................................................... 10 2‐ Development of Living Conditions at the National Level .............................................................. 19 A‐ Development of the national deprivation percentage according to the Living Conditions Index ................................................................................................................................................. 19 -

South Lebanon Livelihoods & Social Stability Sectors Working Group Meeting
South Lebanon Livelihoods & Social Stability Sectors Working Group Meeting - Minutes MEETING Name Social Stability WG / Meeting date April 25 2018 Coordination Meeting Meeting location UNDP South Meeting time 10:30 a.m. Chair person Yousra Taleb / UNDP Meeting 1.00 hr Elie Chaaya and Lynn duration Yu/UNHCR Minutes prepared by UNDP Participants UNICEF, UNDP, PU-AMI, UNIFIL (Civil affairs and CIMIC), CESVI, ACTED, Human Appeal, Isalmic Relief, UNHCR, Hilfswerk Austria International, Solidar Swiss, SHEILD, NRC, OXFAM and Action Against Hunger 1. Welcome & Introduction; Meeting Agenda 2. Presentation of the quarterly Tension Mapping results 3. Activity Info reporting – current status 4. Central Level Update: Our colleagues from the coordination team will be sharing central level sector updates 5. AOB Summary of Discussion Points A. Deviations from original agenda • None 1. Welcome & Introduction • UNDP welcomed the participants on behalf of the co-chairs • The agenda was briefly presented and validated by partners. 2. Presentation of the quarterly Tension Mapping results The tension mapping task force meeting took place on April 19th 2018 at UNDP Tyre office with participation from UNHCR, SHEILD, IRC, UNIFIL, UNDP and UNSCOL. The members followed the same methodology of going through the districts and the previously highlighted villages to see if they are still fall under the same categorization and whether new villages should be added depending on the general status of the village and recorded incidents. The following are the results of the meeting: • Bint Jbeil district o Rmeich (high level): Although no recent incidents took place, the area continues to be a hotspot to keep watching. -

LABOUR FORCE and HOUSEHOLD LIVING CONDITIONS SURVEY 2018-2019 in NABATIEH
LABOUR FORCE and HOUSEHOLD LIVING CONDITIONS SURVEY 2018-2019 in NABATIEH Labour Force and Household Living Conditions Survey (LFHLCS) 2018-2019 in Nabatieh Suggested citation: "Labour Force and Household Living Conditions Survey 2018-2019 in Nabatieh", Central Administration of Statistics, 2020 Copyright © Lebanese Republic Central Administration of Statistics 2020 Acknowledgments Acronyms and Abbreviations This report comes as one of a series of reports launched by the Central Administration of CAS Central Administration of Statistics Statistics, covering the twenty-six districts of Lebanon. Producing these reports was a GER The Gross Enrolment Ratio collaborative endeavor between the Central Administration of Statistics (CAS) and the ILO International Labour Organization United Nations Development Programme (UNDP). LFHLCS Labour Force and Households’ Living Conditions Survey NEET Not in Education, Employment or Training Official statistics presented in this report are drawn from the findings of the national Labour NER The Net Enrolment Rate Force and Households Living Conditions Survey (LFHLCS) that was carried out by CAS NSSF National Social Security Fund between 2018 and 2019 with funding from the Delegation of the European Union to Lebanon and the technical cooperation of the Regional Office for Arab States of the SMAM Singulate Mean Age at Marriage International Labour Organization (ILO). UNDP United Nations Development Programme CAS acknowledges the professional input and contribution of all the partners, experts, and staff who have been particularly active and supportive along the production process in the elaboration, preparation and drafting of the final series of district statistics. CAS would like to express its sincere appreciation to Celine Moyroud and the UNDP core team for all of their technical and administrative support.