Humanitarian Crisis in Cameroon • Humanitarian Crisis in South Sudan
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

5 – 03/07/2020 Humanitarian Implementation Plan (Hip)
Year: 2020 Version: 5 – 03/07/2020 HUMANITARIAN IMPLEMENTATION PLAN (HIP) CENTRAL AFRICA1 The full implementation of this version of the HIP is conditional upon the necessary appropriation being made available from the 2020 general budget of the European Union AMOUNT: EUR 117 200 000 The present Humanitarian Implementation Plan (HIP) was prepared on the basis of the financing decision ECHO/WWD/BUD/2020/01000 (Worldwide Decision) and the related General Guidelines for Operational Priorities on Humanitarian Aid (Operational Priorities). The purpose of the HIP and its annex is to serve as a communication tool for DG ECHO2's partners and to assist them in the preparation of their proposals. The provisions of the Worldwide Decision and the General Conditions of the Agreement with the European Commission shall take precedence over the provisions in this document. This HIP covers Cameroon, the Central African Republic (CAR), Chad and Nigeria. It may also respond to sudden or slow-onset new emergencies in Gabon, Equatorial Guinea, Sao Tomé and Principe, if important unmet humanitarian needs emerge, given the exposure to risk and vulnerabilities of populations in these countries. 0. MAJOR CHANGES SINCE PREVIOUS VERSION OF THE HIP Fourth modification as of 03/07/2020 The total budget of the HIP is increased by EUR 5 million (Central African Republic: EUR 5 million). The perspectives in the Central African Republic for 2020 are very worrisome and the COVID-19 pandemic will exacerbate needs in all sectors. This additional funding will cover unmet needs. The eligible sectors in CAR are: (i) protection (ii) health and nutrition, (iii) food assistance and livelihoods, (iv) water, sanitation and hygiene, (v) shelter (vi) emergency preparedness and response and (vii) education in emergencies. -
Assessment Report
Needs Assessment for Self-Reliance of CAR refugees in Gado, Borgop, Ngam, Mbile, Lolo and Timangolo Camps, and In Touboro Assessment Report Monitoring & Evaluation department November-December 2017 Page 1 of 30 Contents List of abbreviations ...................................................................................................................................... 3 List of figures ................................................................................................................................................. 4 Key findings/executive summary .................................................................................................................. 5 Operational Context ...................................................................................................................................... 6 Introduction: The CAR situation In Cameroon .............................................................................................. 7 Objectives ..................................................................................................................................................... 8 Methodology ................................................................................................................................................. 9 Study Design ............................................................................................................................................. 9 Qualitative Approach ........................................................................................................................... -

Cholera Outbreak
Emergency appeal final report Cameroon: Cholera outbreak Emergency appeal n° MDRCM011 GLIDE n° EP-2011-000034-CMR 31 October 2012 Period covered by this Final Report: 04 April 2011 to 30 June 2012 Appeal target (current): CHF 1,361,331. Appeal coverage: 21%; <click here to go directly to the final financial report, or here to view the contact details> Appeal history: This Emergency Appeal was initially launched on 04 April 2011 for CHF 1,249,847 for 12 months to assist 87,500 beneficiaries. CHF 150,000 was initially allocated from the Federation’s Disaster Relief Emergency Fund (DREF) to support the national society in responding by delivering assistance. Operations update No 1 was issued on 30 May 2011 to revise the objectives and budget of the operation. Operations update No 2 was issued on 31st May 2011 to provide financial statement against revised budget. Operations update No 3 was issued on 12 October 2011 to summarize the achievements 6 months into the operation. Operations update No 4 was issued on 29 February 2012 to extend the timeframe of the operation from 31st March to 30 June 2012 to cover the funding agreement with the American Embassy in Cameroon. PBR No M1111087 was submitted as final report of this operation to the American Embassy in Cameroon on 03 August 2012. Throughout the operation, Cameroon Red Cross volunteers sensitized the populations on PBR No M1111127 was submitted as final report of this how to avoid cholera. Photo/IFRC operation to the British Red Cross on 14 August 2012. Summary: A serious cholera epidemic affected Cameroon since 2010. -

Central African Republic Situation
CENTRAL AFRICAN REPUBLIC SITUATION UNHCR REGIONAL UPDATE 40 8-21 November 2014 KEY FIGURES HIGHLIGHTS 410,000 IDPs including Central African Republic (CAR): On 20 November, UNHCR was invited by the Representative of President Denis Sassou N'Guesso of the Republic 61,244 of Congo (RoC), and current mediator to the crisis, to participate in a in Bangui meeting held in Bangui to discuss the upcoming elections in the country and the feasibility of ensuring the participation of Central African refugees. The meeting was also attended by the Deputy Special 424,580 Representative of the Secretary-General (DSRSG) and UN Resident Total number of CAR refugees in Coordinator of CAR, Mr. Aurélien Agbenonci, the ambassadors of France, neighbouring countries Cameroon, the Democratic Republic of the Congo (DRC), RoC and China, and representatives of the European Union and USAID. UNHCR 187,300 welcomed the Central African authorities’ willingness to hold inclusive elections and reiterated its readiness to assist in discussions between New CAR refugees in neighbouring authorities in CAR and countries of asylum. countries since Dec. 2013 Cameroon: On 5 November, a suspected case of cholera was reported 8,012 on the site Timangolo. The patient reportedly came from Gado via Gbiti Refugees and asylum seekers in three days before symptoms appeared. UNHCR coordinated an CAR immediate multi-sectoral response with WHO, UNICEF, NGO partners and local authorities, including the mobilization of a WASH task force to carry out communication and raising awareness, ensuring potable water treatment and disinfection. FUNDING USD 255 million Population of concern requested for the situation Funded A total of 834,580 people of concern 38% IDPs in CAR 410,000 Gap 62% Refugees in Cameroon 242,578 PRIORITIES Refugees in Chad 93,120 . -

Cameroon: Evaluation of Bank Group Assistance to the Social Sector 1996
AFRICAN DEVELOPMENT BANK GROUP CAMEROON EVALUATION OF BANK GROUP ASSISTANCE TO THE SOCIAL SECTOR 1996-2004 OPERATIONS EVALUATION DEPARTMENT (OPEV) 19 February 2008 CONTENTS ACRONYMS AND ABBREVIATIONS________________________________________ I EXECUTIVE SUMMARY _________________________________________________ II 1. CONTEXT____________________________________________________________ 1 1.1 Evaluation Objectives________________________________________________ 1 1.2 Scope and Methodology ______________________________________________ 1 1.3 Limits of the Evaluation ______________________________________________ 2 1.4 Socioeconomic Context______________________________________________ 2 1.5 Government's Challenges and Strategies _________________________________ 3 1.6 History of Relations with Bank Group ___________________________________ 4 2. BANK ASSISTANCE TO THE SOCIAL SECTOR__________________________ 5 2.1 Bank Country Policies and Strategies _________________________________ 5 2.1.1 Bank Policies____________________________________________________ 5 2.1.2 Bank Strategies in Cameroon ________________________________________ 6 2.1.3 Relevance of Bank Strategies ________________________________________ 7 2.2 Description of Lending Operations ____________________________________ 9 2.2.1 The 1996-2004 Lending Programme__________________________________ 9 2.2.2 Operations Implementation Performance _____________________________ 10 3. EVALUATION OF SECTORAL ASSISTANCE ___________________________ 11 3.1 Non-lending Assistance Evaluation___________________________________ -

Refugee Health Problems in the Central African Sub- Region: the Role of Traditional Medicine
JOURNAL OF THE CAMEROON ACADEMY OF SCIENCES Vol. 14 No. 3 (JANUARY 2019) Research Article REFUGEE HEALTH PROBLEMS IN THE CENTRAL AFRICAN SUB- REGION: THE ROLE OF TRADITIONAL MEDICINE Justine G Nzweundji and 1*Gabriel A Agbor 1*Centre for Research on Medicinal Plants and Traditional Medicine, Institute of Medical Research and Medicinal Plants Studies, Cameroon P.O. Box: 13033, Yaoundé-Cameroon. Email: [email protected]; Phone: +237 677223674 Email: [email protected]; Phone: +237 93667518 *Corresponding author ABSTRACT This review focuses on the role that African Traditional Medicine can play in addressing the health problems of refugees in the central sub-region with focus on Cameroon. This paper is based on a review of literature on the influx of refugees and their well-being. Over 400 000 refugees live in Cameroon particularly in the Far North (Nigerians) and in the Eastern (Central Africans Refugees) Regions of Cameroon. About 80 per cent of the refugees arriving in Cameroon suffer from serious ailments such as malaria, diarrhea, anemia and respiratory tract infections, while more than 20 per cent of children are severely malnourished. To curb these diseases UNHCR and NGOs provide medications to refugees which often arrive late; some of which at times expire in stock or some different distribution centres run out of stock. An aid could come from Traditional Medicine Practitioners who have been very effective in management of disease conditions in refugee camps in some countries in the world. The Cameroon Traditional Medicine if well-developed will do same to act as first-aid before the arrival of conventional medicine or complement western medicine to manage patients who do not accept western medicine because of cultural believes. -

Field Evaluation of Local Integration of Central African Refugees in Cameroon
FIELD EVALUATION OF LOCAL INTEGRATION OF CENTRAL AFRICAN REFUGEES IN CAMEROON FINAL FIELD VISIT REPORT U.S. DEPARTMENT OF STATE TASK ORDER No. SAWMMA13F2592 Evaluating the Effectiveness of Humanitarian Engagement and Programming in Promoting Local Integration of Refugees in Zambia, Tanzania, and Cameroon September 22, 2014 This document was produced for the Department of State by Development by Training Services, Inc. (dTS). FIELD EVALUATION OF LOCAL INTEGRATION OF CENTRAL AFRICAN REFUGEES IN CAMEROON FINAL FIELD VISIT REPORT Evaluating the Effectiveness of Humanitarian Engagement and Programming in Promoting Local Integration of Refugees in Zambia, Tanzania, and Cameroon Submitted to: Office of Policy and Resource Planning, Bureau of Population, Refugees and Migration (PRM), U.S. Department of State Prepared by: Development and Training Services, Inc. (dTS) TABLE OF CONTENTS ACRONYM LIST ......................................................................................................................................... ii EXECUTIVE SUMMARY ......................................................................................................................... iii CHAPTER I: INTRODUCTION .................................................................................................................. 1 A. SCOPE OF WORK ........................................................................................................................... 1 B. METHODOLOGY ............................................................................................................................. -
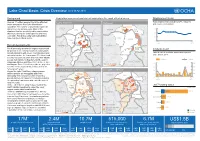
Lac Chad Snapshot 06 Apr 2017 Copy
Lake Chad Basin: Crisis Overview (as of 06 Apr 2017) Background Population movement and violent incidents in the most affected areas Displacement trend Total displacements including IDPs, refugees Around 17 million people live in the affected Latest incidents1 Refugees2 areas across the four Lake Chad basin and returnees (in million) countries. The number of displaced people has Diffa NIGER Lac 3.0 tripled over the last two years. Most of the Diffa NIGER 106.2k displaced families are sheltered by communities 7.8k 2.5 that count among the world’s poorest and most Lac Kukawa vulnerable. Food insecurity and malnutrition 2.0 Borno Yobe have reached critical levels. Borno Yobe Jere Dikwa 1.5 Mar Mar Maiduguri 2016 2017 Konduga Gwoza Recent developments NIGERIA Waza CHAD NIGERIA CHAD Mayo Moskota Far-North Food insecurity across the region is projected 86.3k Incidents trend1 to worsen in the coming months as communities Far-North already struggling with severe food shortages and Total of violent incidents and deaths reported adversity traverse the lean season. The latest food Adamawa since March 2016 Adamawa security assessments show that more than 50,000 people risk famine in Nigeria’s north-eastern Incidents Deaths Adamawa, Borno and Yobe states between June CAMEROON CAMEROON 0,4k 10 15 35 70k 40 400 and August. Some 5.2 million people are projected Incidents to suffer severe food scarcity, a third of them at Diffa 30 300 “emergency” levels. 3 5 Internally Displaced Persons Accessible territories 200 Across the Lake Chad Basin, almost seven 20 million people are struggling with food 10 100 Diffa NIGER Diffa insecurity. -

Sea Level Rise and Implications for Low-Lying Islands, Coasts and Communities
Sea Level Rise and Implications for Low-Lying Islands, SPM4 Coasts and Communities Coordinating Lead Authors: Michael Oppenheimer (USA), Bruce C. Glavovic (New Zealand/South Africa) Lead Authors: Jochen Hinkel (Germany), Roderik van de Wal (Netherlands), Alexandre K. Magnan (France), Amro Abd-Elgawad (Egypt), Rongshuo Cai (China), Miguel Cifuentes-Jara (Costa Rica), Robert M. DeConto (USA), Tuhin Ghosh (India), John Hay (Cook Islands), Federico Isla (Argentina), Ben Marzeion (Germany), Benoit Meyssignac (France), Zita Sebesvari (Hungary/Germany) Contributing Authors: Robbert Biesbroek (Netherlands), Maya K. Buchanan (USA), Ricardo Safra de Campos (UK), Gonéri Le Cozannet (France), Catia Domingues (Australia), Sönke Dangendorf (Germany), Petra Döll (Germany), Virginie K.E. Duvat (France), Tamsin Edwards (UK), Alexey Ekaykin (Russian Federation), Donald Forbes (Canada), James Ford (UK), Miguel D. Fortes (Philippines), Thomas Frederikse (Netherlands), Jean-Pierre Gattuso (France), Robert Kopp (USA), Erwin Lambert (Netherlands), Judy Lawrence (New Zealand), Andrew Mackintosh (New Zealand), Angélique Melet (France), Elizabeth McLeod (USA), Mark Merrifield (USA), Siddharth Narayan (US), Robert J. Nicholls (UK), Fabrice Renaud (UK), Jonathan Simm (UK), AJ Smit (South Africa), Catherine Sutherland (South Africa), Nguyen Minh Tu (Vietnam), Jon Woodruff (USA), Poh Poh Wong (Singapore), Siyuan Xian (USA) Review Editors: Ayako Abe-Ouchi (Japan), Kapil Gupta (India), Joy Pereira (Malaysia) Chapter Scientist: Maya K. Buchanan (USA) This chapter should be cited as: Oppenheimer, M., B.C. Glavovic , J. Hinkel, R. van de Wal, A.K. Magnan, A. Abd-Elgawad, R. Cai, M. Cifuentes-Jara, R.M. DeConto, T. Ghosh, J. Hay, F. Isla, B. Marzeion, B. Meyssignac, and Z. Sebesvari, 2019: Sea Level Rise and Implications for Low-Lying Islands, Coasts and Communities. -

2019 Report World Observatory on Subnational Government Finance
2019 Report World Observatory on Subnational Government Finance and Investment FINANCE AND INVESTMENT AND FINANCE Key findings 2019 REPORT WORLD OBSERVATORY ON SUBNATIONAL GOVERNMENT GOVERNMENT SUBNATIONAL ON OBSERVATORY WORLD REPORT 2019 │ 1 2019 Report World Observatory on Subnational Government Finance and Investment Key Findings Launch version 2 │ General disclaimer This work is published under the responsibility of the Secretary-General of the OECD. The opinions expressed and arguments employed herein do not necessarily reflect the official views of OECD member countries or those of United Cities and Local Government (UCLG). This document and any maps included herein are without prejudice to the status of or sovereignty over any territory, to the delimitation of international frontiers and boundaries and to the name of any territory, city or area. © OECD 2019 You can copy, download or print OECD content for your own use, and you can include excerpts from OECD publications, databases and multimedia products in your own documents, presentations, blogs, websites and teaching materials, provided that suitable acknowledgment of the source and copyright owner is given. All requests for public or commercial use and translation rights should be submitted to [email protected]. Requests for permission to photocopy portions of this material for public or commercial use shall be addressed directly to the Copyright Clearance Center (CCC) at [email protected] or the Centre français d’exploitation du droit de copie (CFC) at [email protected]. Please cite this publication as: OECD/UCLG (2019), 2019 Report of the World Observatory on Subnational Government Finance and Investment – Key Findings │ 3 Acknowledgements The World Observatory of Subnational Government Finance and Investment is a joint endeavour of the OECD Centre for Entrepreneurship, SMEs, Regions and Cities (CFE), led by Lamia Kamal-Chaoui, Director and of United Cities and Local Government (UCLG) under the direction of Emilia Saiz, Secretary General of UCLG. -

Central African Refugees (CAR) and Host Population Living in the East, Adamawa, North Regions of Cameroon
UNHCR & WFP Joint Assessment Mission (JAM) Central African refugees (CAR) and host population living in the East, Adamawa, North Regions of Cameroon - Primary data collected from 21 to 31 January 2019 - Table of Contents ACKNOWLEDGMENTS ______________________________________________________ 4 ACRONYMS ________________________________________________________________ 6 EXECUTIVE SUMMARY _____________________________________________________ 7 1. Introduction ____________________________________________________________ 11 1.1 Background to the Joint Assessment Mission _____________________________________ 12 1.2 Objective of the Joint Assessment Mission ________________________________________ 12 1.3 Overall picture of the refugee situation: origin, population size and demography, sites, surrounding community relations __________________________________________________ 12 1.4 Verification process and coordination ___________________________________________ 13 2. Description of current Assistance to refugees __________________________________ 14 2.1 Current Assistance provided by UNHCR (Protection, NFI, WASH, Safety Net, Livelihood) ______________________________________________________________________________ 14 2.2 Current assistance provided by the WFP _________________________________________ 17 2.2.1 General Food Distributions ___________________________________________________________ 17 2.2.2 Blanket supplementary feeding 6-23 months ______________________________________________ 18 2.2.3 Asset creation for early recovery, community -
The Localization of the Global Agendas How Local Action Is Transforming Territories and Communities
2019 The Localization of the Global Agendas How local action is transforming territories and communities Fifth Global Report on Decentralization and Local Democracy 2 GOLD V REPORT © 2019 UCLG The right of UCLG to be identified as author of the editorial material, and of the individual authors as authors of their contributions, has been asserted by them in accordance with sections 77 and 78 of the Copyright, Designs and Patents Act 1988. All rights reserved. No part of this book may be reprinted or reproduced or utilized in any form or by any electronic, mechanical or other means, now known or hereafter invented, including photocopying and recording, or in any information storage or retrieval system, without permission in writing from the publishers. United Cities and Local Governments Cités et Gouvernements Locaux Unis Ciudades y Gobiernos Locales Unidos Avinyó 15 08002 Barcelona www.uclg.org DISCLAIMERS The terms used concerning the legal status of any country, territory, city or area, or of its authorities, or concerning delimitation of its frontiers or boundaries, or regarding its economic system or degree of development do not necessarily reflect the opinion of United Cities and Local Governments. The analysis, conclusions and recommendations of this report do not necessarily reflect the views of all the members of United Cities and Local Governments. This document has been produced with the financial assistance of the European Union. The contents of this document are the sole responsibility of UCLG and can under no circumstances be regarded as reflecting the position of the European Union. Graphic design and lay-out: www.ggrafic.com Cover photos: A-C-K (t.ly/xP7pw); sunriseOdyssey (bit.ly/2ooZTnM); TEDxLuanda (bit.ly/33eFEIt); Curtis MacNewton (bit.ly/2Vm5Yh1); s1ingshot (t.ly/yWrwV); Chuck Martin (bit.ly/30ReOEz); sunsinger (shutr.bz/33dH85N); Michael Descharles (t.ly/Mz7w3).