Obesity in Young Europeans: Genetic and Environmental In¯Uences
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Federation to Hold Super Sunday on August 29 by Reporter Staff Contact the Federation Campaign
August 13-26, 2021 Published by the Jewish Federation of Greater Binghamton Volume L, Number 17 BINGHAMTON, NEW YORK Federation to hold Super Sunday on August 29 By Reporter staff contact the Federation Campaign. When the The Jewish Federation of Greater Bing- at [email protected] community pledges hamton will hold Super Sunday on Sunday, or 724-2332. Marilyn early, the allocation August 29, at 10 am, at the Jewish Commu- Bell is the chairwom- process is much eas- nity Center, 500 Clubhouse Rd., Vestal. It an of Campaign 2022. ier. We also want the will feature a brunch, comedy by comedian “We are hoping snow birds to have Josh Wallenstein and a showing of the film to get community an opportunity to “Fiddler: A Miracle of Miracles” about the members to pledge gather before they Broadway musical “Fiddler on the Roof.” early again this year,” leave for sunnier Larry Kassan, who has directed productions said Shelley Hubal, climates this fall.” of the musical, will facilitate the film discus- executive director of Bell noted how im- sion. The cost of the brunch and film is $15 the Federation. “We started the 2021 Cam- portant the Campaign is to the community. and reservations are requested by Sunday, paign with almost 25 percent of the pledges “As I begin my fourth year as Campaign August 22. To make reservations, visit already made. That helped to cut back on chair, I know – and I know that you know the Federation website, www.jfgb.org/, or the manpower we needed to get through the – how essential our local organizations are to the Jewish community,” she said. -

Transcontinental Trade and Economic Growth
M. SHATZMILLER: TRANSCONTINENTAL TRADE AND ECONOMIC GROWTH Transcontinental Trade and Economic Growth in the Early Islamic Empire: The Red Sea Corridor in the 8th-10th Centuries Maya Shatzmiller The question of why and how sustained economic growth the long term, it surely qualifies as a ‘trend’ or a ‘cycle’ occurs in historical societies is most frequently studied in in historical economic growth.7 Several long-term fac- relation to the European model, otherwise known as the tors brought about a series of changes in the key econom- ‘Rise of the West’, the only model to have been studied ic components of the empire: an increase in monetary in detail so far.1 The debate continues over why western supply and circulation; the development and elaboration Europe forged ahead and remained so consistently, while of state fiscal institutions with an efficient system of tax other societies, including eastern Europe, were unable to collection; the creation of legal institutions to uphold stage their own ‘rise’ through intensive growth, maintain property rights; demographic growth resulting from both it consistently once it occurred, or indeed successfully internal population growth and the importing of slaves; emulate the European model. On the other hand, there is a increased output in the manufacturing sector as a result mounting feeling of dissatisfaction with the notion of ex- of increased division of labour; and finally, an increased clusiveness and uniqueness which accompanies the debate volume of trade, efficient markets, commercial techniques about ‘The Rise of the West/Europe’.2 Those who study and development of credit tools. It is the trade component non-Western societies suggest that alternative interpreta- that will concern us here, since it presents us with an ele- tions and comparative studies of economic growth do exist ment that is variable in a comparative context – the ele- and should be looked at, rather than simply accepting the ment being the role of intercontinental trade in economic European model at its face value. -
Did Comet HEINRICH-Swift-Tuttle Terminate Roman and Global Civilization? [ROME’S POPULATION CATASTROPHE: G
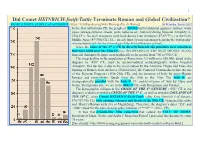
1 Did Comet HEINRICH-Swift-Tuttle Terminate Roman and Global Civilization? [ROME’S POPULATION CATASTROPHE: https://it.wikipedia.org/wiki/Demografia_di_Roma] G. Heinsohn, January 2021 In the first millennium CE, the people of ROME built residential quarters, latrines, water pipes, sewage systems, streets, ports, bakeries etc., but only during Imperial Antiquity (1- 230s CE). No such structures were built during Late Antiquity (4th-6th/7th c.) or the Early Middle Ages (8th-930s CE). [See already https://q-mag.org/gunnar-heinsohn-the-stratigraphy- of-rome-benchmark-for-the-chronology-of-the-first-millennium-ce.html] Since the ruins of the 3rd c. CE lie directly beneath the primitive new structures that were built after the 930s CE (i.e., BEGINNING OF THE HIGH MIDDLE AGES), Imperial Antiquity belongs stratigraphically to the period from 700 to 930s CE. The steep decline in the population of Rome from 1.5 million to 650,000, dated in the diagram to "450" CE, must be accommodated archaeologically within Imperial Antiquity. This decline is due to the crisis caused by the Antonine Plague and Fires, the burning of Rome's State Archives (Tabularium), the Comet of Commodus before the rise of the Severan Emperors (190s-230s CE), and the invasion of Italy by proto-Hunnic Iazyges and proto-Gothic Quadi from the 160s to the 190s. The 160s ff. are stratigraphically parallel with the 450s ff. CE and its invasion of Italy by Huns and Goths. Stratigraphically, we are in the 860s ff. CE, with Hungarians and Vikings. The demographic collapse in the CRISIS OF THE 6th CENTURY (“553” CE in the diagram) is identical with the CRISIS OF THE 3rd C., as well as with the COLLAPSE OF THE 10th C., when Comet HEINRICH-Swift-Tuttle (after King Heinrich I of Saxony; 876/919-936 CE) with ensuing volcanos and floods of the 930s CE ) damaged the globe and Henry’s Roman style city of Magdeburg). -

1 Making a Difference in Tenth-Century Politics: King
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by St Andrews Research Repository 1 Making a Difference in Tenth-Century Politics: King Athelstan’s Sisters and Frankish Queenship Simon MacLean (University of St Andrews) ‘The holy laws of kinship have purposed to take root among monarchs for this reason: that their tranquil spirit may bring the peace which peoples long for.’ Thus in the year 507 wrote Theoderic, king of the Ostrogoths, to Clovis, king of the Franks.1 His appeal to the ideals of peace between kin was designed to avert hostilities between the Franks and the Visigoths, and drew meaning from the web of marital ties which bound together the royal dynasties of the early-sixth-century west. Theoderic himself sat at the centre of this web: he was married to Clovis’s sister, and his daughter was married to Alaric, king of the Visigoths.2 The present article is concerned with a much later period of European history, but the Ostrogothic ruler’s words nevertheless serve to introduce us to one of its central themes, namely the significance of marital alliances between dynasties. Unfortunately the tenth-century west, our present concern, had no Cassiodorus (the recorder of the king’s letter) to methodically enlighten the intricacies of its politics, but Theoderic’s sentiments were doubtless not unlike those that crossed the minds of the Anglo-Saxon and Frankish elite families who engineered an equally striking series of marital relationships among themselves just over 400 years later. In the early years of the tenth century several Anglo-Saxon royal women, all daughters of King Edward the Elder of Wessex (899-924) and sisters (or half-sisters) of his son King Athelstan (924-39), were despatched across the Channel as brides for Frankish and Saxon rulers and aristocrats. -

ATCO Electric Ltd
Decision 2013-332 ATCO Electric Ltd. Beartrap Transmission Project August 30, 2013 The Alberta Utilities Commission Decision 2013-332: ATCO Electric Ltd. Beartrap Transmission Project Application No. 1609059 Proceeding ID No. 2196 August 30, 2013 Published by The Alberta Utilities Commission Fifth Avenue Place, Fourth Floor, 425 First Street S.W. Calgary, Alberta T2P 3L8 Telephone: 403-592-8845 Fax: 403-592-4406 Website: www.auc.ab.ca Contents 1 Introduction ........................................................................................................................... 1 2 Background ........................................................................................................................... 1 2.1 The approval process for new transmission development in Alberta ............................ 1 2.2 Beartrap 940S substation needs identification document approval ............................... 2 2.3 ATCO’s facility application ........................................................................................... 2 2.4 Beartrap 940S substation................................................................................................ 3 2.5 Interventions ................................................................................................................... 3 2.6 Hearing ........................................................................................................................... 4 3 Issues ..................................................................................................................................... -

Welsh Kings at Anglo-Saxon Royal Assemblies (928–55) Simon Keynes
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Apollo Keynes The Henry Loyn Memorial Lecture for 2008 Welsh kings at Anglo-Saxon royal assemblies (928–55) Simon Keynes A volume containing the collected papers of Henry Loyn was published in 1992, five years after his retirement in 1987.1 A memoir of his academic career, written by Nicholas Brooks, was published by the British Academy in 2003.2 When reminded in this way of a contribution to Anglo-Saxon and Anglo-Norman studies sustained over a period of 50 years, and on learning at the same time of Henry’s outstanding service to the academic communities in Cardiff, London, and elsewhere, one can but stand back in awe. I was never taught by Henry, but encountered him at critical moments—first as the external examiner of my PhD thesis, in 1977, and then at conferences or meetings for twenty years thereafter. Henry was renowned not only for the authority and crystal clarity of his published works, but also as the kind of speaker who could always be relied upon to bring a semblance of order and direction to any proceedings—whether introducing a conference, setting out the issues in a way which made one feel that it all mattered, and that we stood together at the cutting edge of intellectual endeavour; or concluding a conference, artfully drawing together the scattered threads and making it appear as if we’d been following a plan, and might even have reached a conclusion. First place at a conference in the 1970s and 1980s was known as the ‘Henry Loyn slot’, and was normally occupied by Henry Loyn himself; but once, at the British Museum, he was for some reason not able to do it, and I was prevailed upon to do it in his place. -

Resolution No.___A Resolution of the City of Sapulpa, Oklahoma and the Sapulpa Municipal Trust Authority Amending
RESOLUTION NO._____________ A RESOLUTION OF THE CITY OF SAPULPA, OKLAHOMA AND THE SAPULPA MUNICIPAL TRUST AUTHORITY AMENDING THE FY 2020-2021 ANNUAL BUDGET BY INCREASING REVENUES BY $7,181,750.00 AND INCREASING APPROPRIATIONS BY $3,495,250.00 IN VARIOUS FUNDS FOR THE PURPOSE OF MAKING ADJUSTMENTS BASED ON CURRENT REVENUE. WHEREAS, several transfers between funds and payments are based on actual revenue and the revenue is now estimated to be more than budget resulting in an increase in the transfers or expenditures, NOW, THEREFORE BE IT RESOLVED, by the City Council of the City of Sapulpa, Oklahoma, and the Sapulpa Municipal Authority, Sapulpa, Oklahoma, that the following budget amendments be made: GENERAL FUND (Increase) 10-4003 Sales Tax - First Penny $ 900,000.00 (Increase) 10-4003.01 Sales Tax – 2nd & 3rd Penny 1,800,000.00 (Increase) 10-4003.02 Sales Tax – ½ Penny 450,000.00 (Increase) 10-4003.03 Sales Tax – ½ Penny 450,000.00 (Increase) 10-4026 Resident Constr Park/Rec Fee 4,000.00 (Increase) 10-4920S Tsfr In: SMA-Sales Tax ___720,000.00 Total Revenue Increase $ 4,324,000.00 (Increase) 10-590-920S Tsfr Out: SMA $ 720,000.00 (Increase) 10-590-931S Tsfr Out: Cemetery 45,000.00 (Increase) 10-590-934S Tsfr Out: Library 45,000.00 (Increase) 10-590-935S Tsfr Out: Park & Rec 90,000.00 (Increase) 10-590-937 Tsfr Out: Park & Rec Capital 4,000.00 (Increase) 10-590-940S Tsfr Out: Fire Cash 45,000.00 (Increase) 10-590-941S Tsfr Out: Police Cash 45,000.00 (Increase) 10-590-944S Tsfr Out: Major Thorofare 90,000.00 (Increase) 10-590-945S Tsfr -

The Origins of the English Kingdom
ENGLISH KINGDOM The Origins of the English KINGDOMGeorge Molyneaux explores how the realm of the English was formed and asks why it eclipsed an earlier kingship of Britain. UKE WILLIAM of Normandy defeated King King Harold is Old English ones a rice – both words can be translated as Harold at Hastings in 1066 and conquered the killed. Detail ‘kingdom’. The second is that both in 1016 and in 1066 the from the Bayeux English kingdom. This was the second time in 50 Tapestry, late 11th kingdom continued as a political unit, despite the change years that the realm had succumbed to external century. in ruling dynasty. It did not fragment, lose its identity, or Dattack, the first being the Danish king Cnut’s conquest of become subsumed into the other territories of its conquer- 1016. Two points about these conquests are as important as ors. These observations prompt questions. What did this they are easily overlooked. The first is that contemporaries 11th-century English kingdom comprise? How had it come regarded Cnut and William as conquerors not merely of an into being? And how had it become sufficiently robust and expanse of land, but of what Latin texts call a regnum and coherent that it could endure repeated conquest? FEBRUARY 2016 HISTORY TODAY 41 ENGLISH KINGDOM Writers of the 11th century referred to the English kingdom in Latin as the regnum of ‘Anglia’, or, in the vernacular, as the rice of ‘Englaland’. It is clear that these words denoted a territory of broadly similar size and shape to what we think of as ‘England’, distinct from Wales and stretching from the Channel to somewhere north of York. -

Arts of Asia Lecture Series Spring 2015 Masterpieces and Iconic Artworks of the Asian Art Museum Sponsored by the Society for Asian Art
Arts of Asia Lecture Series Spring 2015 Masterpieces and Iconic Artworks of the Asian Art Museum Sponsored by The Society for Asian Art The Divine Royal Couple: Shiva and Parvati From Angkor February 20, 2015 Forrest McGill The Hindu deities Shiva and Parvati approx. 1000-1100 (or approx. 975-1075) Cambodia, former kingdom of Angkor Sandstone; The Avery Brundage Collection, B66S2 Angkor Kingdom Cambodia approx. 800-1450 also parts of Thailand and Vietnam Some art styles of the Angkor period (named for the primary monuments of the periods) (all dates approximate) founding of Angkor 802 Bakheng style 890s-920s Koh Ker style 920s-940s Pre Rup style 940s-960s Banteay Srei style 960s-1000s Khleang style 960s-1010s Baphuon style 1010s–1080s Angkor Wat style 1100s–1170s Bayon style 1180s–1220s Ayutthaya invasion 1431 Further reading Baptiste, Pierre, and Thierry Zéphir. 2008. L’art khmer dans les collections du musée Guimet. Paris: Réunion des musées nationaux. Dalsheimer, Nadine. 2001. Les collections du Musée national de Phnom Penh: l'art du Cambodge ancien. Paris: École française d’Extrême-Orient. Chandler, David. 2000. A History of Cambodia. Boulder, CO: Westview Press. Freeman, Michael and Claude Jacques. 1999. Ancient Angkor. Bangkok: River Books. Jessup, Helen Ibbitson. 2004. Art and Architecture of Cambodia. London; New York: Thames and Hudson. Jessup, Helen Ibbitson and Thierry Zéphir, eds. 1997. Sculpture of Angkor and Ancient Cambodia: Millennium of Glory. London: Thames and Hudson. Kramrisch, Stella. 1981. Manifestations of Shiva. Philadelphia: Philadelphia Museum of Art. Mabbett, Ian and David Chandler. 1996. The Khmers. Bangkok: Silkworm Books. [The following article, proposing a complete reordering of the later monuments and styles of Angkor, is said by its author to be “neither complete nor conclusive,” and remains highly controversial. -

Byzantine Military Tactics in Syria and Mesopotamia in the Tenth Century
Byzantine Military Tactics in Syria and Mesopotamia in the Tenth Century 5908_Theotokis.indd i 14/09/18 11:38 AM 5908_Theotokis.indd ii 14/09/18 11:38 AM BYZANTINE MILITARY TACTICS IN SYRIA AND MESOPOTAMIA IN THE TENTH CENTURY A Comparative Study Georgios Theotokis 5908_Theotokis.indd iii 14/09/18 11:38 AM Edinburgh University Press is one of the leading university presses in the UK. We publish academic books and journals in our selected subject areas across the humanities and social sciences, combining cutting-edge scholarship with high editorial and production values to produce academic works of lasting importance. For more information visit our website: edinburghuniversitypress.com © Georgios Theotokis, 2018 Edinburgh University Press Ltd The Tun – Holyrood Road 12 (2f) Jackson’s Entry Edinburgh EH8 8PJ Typeset in 11/ 13 JaghbUni Regular by IDSUK (DataConnection) Ltd, and printed and bound in Great Britain A CIP record for this book is available from the British Library ISBN 978 1 4744 3103 3 (hardback) ISBN 978 1 4744 3105 7 (webready PDF) ISBN 978 1 4744 3106 4 (epub) The right of Georgios Theotokis to be identifi ed as author of this work has been asserted in accordance with the Copyright, Designs and Patents Act 1988 and the Copyright and Related Rights Regulations 2003 (SI No. 2498). 5908_Theotokis.indd iv 14/09/18 11:38 AM Contents Acknowledgements vi List of Rulers vii Map 1 Anatolia and Upper Mesopotamia viii Map 2 Armenian Themes and Pri ncipalities ix Introduction 1 1 The ‘Grand Strategy’ of the Byzantine Empire 23 2 Byzantine and Arab Strategies and Campaigning Tactics in Cilicia and Anatolia (Eighth–Tenth Centuries) 52 3 The Empire’s Foreign Policy in the East and the Key Role of Armenia (c. -

In the Writings of Rómulo Lachatañéré and Arthur Ramos
OLÍVIA M.G. CunHA Travel, Ethnography, and Nation in the Writings of RÓmulo LachataÑÉRÉ and Arthur Ramos In 928-929 the Brazilian writer Mário de Andrade began publishing in a local newspaper the material he had collected during his travels to the inte- rior of Brazil. The journal entries, personal itineraries, essays, poetry frag- ments, and photographs he had amassed over two long journeys through the northern and northeast regions composed a unique ethnography, which Andrade entitled O turista aprendiz (976, The apprentice tourist). The idea of the scholar abandoning the “center” and, therefore, displacing urban culture and written language, a notion inherent in his own experi- ence, made him view travel as an experience of interpretation rather than merely observation. Through what was an attempt at producing an eth- nography, Andrade not only generated information, but created a unique encounter inspired by the idea of apprenticeship. Instead of conceiving of himself as an ethnographer, Andrade preferred to think of himself as a special kind of tourist, there not only to observe, but also to learn. The intriguing connections between anthropology, modernism, and nationalism in the work of Mário de Andrade invite comparisons with other Latin American texts from the same period (Guicharnaud-Tollis 982, Kutzinski 993, Masiello 993). However, in this essay, the modality of travel described in O turista aprendiz will be used not as a paradigm, but as an inspiring starting point to explore an issue which has been examined . The first version of this essay was presented at the Center for Latin American Studies Seminar at the University of Michigan, on March 27, 2000. -

Plavinski the Main Tendencies in the Development of Tenth To13th
VIII.ARMAMENTS AND DEFENSIVE SYSTEMS THE MAIN TENDENCIES IN THE DEVELOPMENT The Main Tendenciesin the Development to 13th CenturyofWeapons Tenth Blade in Belarus OF TENTH TO 13TH CENTURY BLADE WEAPONS IN BELARUS MIKALAI PLAVINSKI MIKALAI PLAVINSKI Abstract The article is devoted to the history of tenth to 13th-century blade weapons in Belarus. The main tendencies in the evolution of blade weapons and the most important directions in military-technical contacts of the population of Belarus are defined. Key words: blade weapons, sword, sword chape, sabre, Belarus, Medieval Period. Introduction H swords originate from the hoard found on Bryleus- kae field, from Vitebsk and from its neighborhood (see In the tenth century the largest part of the territory of catalogue 1, № 1–3). There is a blade inscription on the Belarus was already populated by Slavs. The Baltic sword from Vitebsk that can be read as VLFBERH+. population, bearers of East Lithuanian Barrow Culture Type V swords were found in Polatsk and in barrow and Jatvingians lived just in the northwest, in the basin cemeteries Garadzilava and Gurkovichy (see catalogue of the middle Nioman��������������������������������Nemunas����������������������� river. Slavs and Balts 1, № 4–6). The Polatsk sword has the inscription ULF- had different military-technical traditions that are in BERHT on the blade. The possibility of the use of type a certain way revealed in the types of blade weapons V swords is indirectly proven by graffiti on fragments they were using during the tenth to 13th centuries. of dirhams from Kazjankauski (940s) and Garaulianski The period can be divided into two sub-periods, which 2 (the middle of the 11th century) hoards (Dobrovol- coincide with large epochs in the region’s history.