Mapping of Schistosomiasis and Soil- Transmitted Helminths in Yemen, and the Push for Elimination
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Humanitarian Update
YEMEN HUMANITARIAN Covering 12 March – 18 March UPDATE 2018 | Issue 7 DIPHTHERIA VACCination CAMPAIGN targetS 2.7 MILLION CHILDREN National and international partners have completed a large-scale vaccination campaign with the aim to control the spread of diphtheria in Yemen. Targeting nearly 2.7 million children aged six weeks to 15 years in 11 governorates, the campaign focused on locations reporting suspected cases of diphtheria and areas at high risk of spread of the infectious respiratory disease. On the west coast where violence has recently escalated, 835,775 children were targeted in Al Hudaydah, Hajjah, Al Mahwit and Raymah governorates. The campaign, supported by WHO and UNICEF, is part of a larger response plan that includes strengthening surveillance and case detection, enhancing laboratory testing capacity, procuring and distributing diphtheria anti-toxins to health facilities, and training and deploying rapid response teams to trace contacts and provide preventive treatment in communities. Health education and awareness campaigns were conducted to teach people how to protect themselves against diphtheria and other infectious diseases. First reported in October 2017, diphtheria has spread rapidly, infecting more than 1,300 people and killing over 70. Almost 80 per cent of the caseload are children and young adults below 25 years of age. The rapid spread of the disease highlights major gaps in routine vaccination coverage in recent years and signifies a collapsing health system where only half of all health facilities are partially or fully functioning. In November and December 2017, WHO and UNICEF vaccinated almost 450,000 children under 7 years of age against diphtheria in Ibb – the worst affected governorate accounting for nearly 35 per cent of all reported cases. -

CDC Overseas Parasite Guidelines
Guidelines for Overseas Presumptive Treatment of Strongyloidiasis, Schistosomiasis, and Soil-Transmitted Helminth Infections for Refugees Resettling to the United States U.S. Department of Health and Human Services Centers for Disease Control and Prevention National Center for Emerging and Zoonotic Infectious Diseases Division of Global Migration and Quarantine February 6, 2019 Accessible version: https://www.cdc.gov/immigrantrefugeehealth/guidelines/overseas/intestinal- parasites-overseas.html 1 Guidelines for Overseas Presumptive Treatment of Strongyloidiasis, Schistosomiasis, and Soil-Transmitted Helminth Infections for Refugees Resettling to the United States UPDATES--the following are content updates from the previous version of the overseas guidance, which was posted in 2008 • Latin American and Caribbean refugees are now included, in addition to Asian, Middle Eastern, and African refugees. • Recommendations for management of Strongyloides in refugees from Loa loa endemic areas emphasize a screen-and-treat approach and de-emphasize a presumptive high-dose albendazole approach. • Presumptive use of albendazole during any trimester of pregnancy is no longer recommended. • Links to a new table for the Treatment Schedules for Presumptive Parasitic Infections for U.S.-Bound Refugees, administered by IOM. Contents • Summary of Recommendations • Background • Recommendations for overseas presumptive treatment of intestinal parasites o Refugees originating from the Middle East, Asia, North Africa, Latin America, and the Caribbean o Refugees -

World Bank Document
The World Bank Report No: ISR13583 Implementation Status & Results Yemen, Republic of Second Rural Access Project (P085231) Operation Name: Second Rural Access Project (P085231) Project Stage: Implementation Seq.No: 18 Status: ARCHIVED Archive Date: 21-Jun-2014 Country: Yemen, Republic of Approval FY: 2006 Public Disclosure Authorized Product Line:IBRD/IDA Region: MIDDLE EAST AND NORTH AFRICA Lending Instrument: Adaptable Program Loan Implementing Agency(ies): Key Dates Board Approval Date 08-Nov-2005 Original Closing Date 30-Nov-2010 Planned Mid Term Review Date 15-Nov-2008 Last Archived ISR Date 27-Dec-2013 Public Disclosure Copy Effectiveness Date 07-Jun-2006 Revised Closing Date 30-Nov-2015 Actual Mid Term Review Date 26-Oct-2008 Project Development Objectives Project Development Objective (from Project Appraisal Document) The objective of the Rural Access Program (RAP) and of the Second Rural Access Project (RAP2) is to improve year-round access of the rural population to markets and services. Has the Project Development Objective been changed since Board Approval of the Project? ● Yes No Public Disclosure Authorized Component(s) Component Name Component Cost Rural Access Roads 67.20 Institutional Support and Capacity Building 3.45 Road Maintenance 12.33 Overall Ratings Previous Rating Current Rating Progress towards achievement of PDO Moderately Satisfactory Moderately Satisfactory Overall Implementation Progress (IP) Moderately Satisfactory Moderately Satisfactory Public Disclosure Authorized Overall Risk Rating Substantial Substantial Implementation Status Overview The Project team conducted its latest supervision mission in June 2014, and expressed satisfaction with the progress. Most contracts are poised to be awarded and signed by June 30, 2014. -

Download File
Yemen Country Office Humanitarian Situation Report ©UNICEF Yemen/2019/Mahmoud Fadhel Reporting Period: 1 - 31 October 2019 Highlights Situation in Numbers • In October, 3 children were killed, 16 children were injured and 3 12.3 million children in need of boys were recruited by various parties to the conflict. humanitarian assistance • 59,297 suspected Acute Watery Diarrhoea (AWD)/cholera cases were identified and 50 associated deaths were recorded (0.08 case 24.1 million fatality rate) in October. UNICEF treated over 14,000 AWD/cholera people in need suspected cases (one quarter of the national caseload). (OCHA, 2019 Yemen Humanitarian Needs Overview) • Due to fuel crisis, in Ibb, Dhamar and Al Mahwit, home to around 400,000 people, central water systems were forced to shut down 1.71 million completely. children internally displaced • 3.1 million children under five were screened for malnutrition, and (IDPs) 243,728 children with Severe Acute Malnutrition (76 per cent of annual target) admitted for treatment. UNICEF Appeal 2019 UNICEF’s Response and Funding Status US$ 536 million Funding Available* SAM Admission 76% US$ 362 million Funding status 68% Nutrition Measles Rubella Vaccination 91% Health Funding status 77% People with drinking water 100% WASH Funding status 64% People with Mine Risk Education 82% Child Funding status 40% Protection Children with Access to Education 29% Funding status 76% Education People with Social Economic 61% Assistance Policy Social Funding status 38% People reached with C4D efforts 100% *Funds available includes funding received for the current C4D Funding status 98% appeal (emergency and other resources), the carry- forward from the previous year and additional funding Displaced People with RRM Kits 59% which is not emergency specific but will partly contribute towards 2019 HPM results. -

Rapid Screening for Schistosoma Mansoni in Western Coã Te D'ivoire Using a Simple School Questionnaire J
Rapid screening for Schistosoma mansoni in western Coà te d'Ivoire using a simple school questionnaire J. Utzinger,1 E.K. N'Goran,2 Y.A. Ossey,3 M. Booth,4 M. TraoreÂ,5 K.L. Lohourignon,6 A. Allangba,7 L.A. Ahiba,8 M. Tanner,9 &C.Lengeler10 The distribution of schistosomiasis is focal, so if the resources available for control are to be used most effectively, they need to be directed towards the individuals and/or communities at highest risk of morbidity from schistosomiasis. Rapid and inexpensive ways of doing this are needed, such as simple school questionnaires. The present study used such questionnaires in an area of western Coà te d'Ivoire where Schistosoma mansoni is endemic; correctly completed questionnaires were returned from 121 out of 134 schools (90.3%), with 12 227 children interviewed individually. The presence of S. mansoni was verified by microscopic examination in 60 randomly selected schools, where 5047 schoolchildren provided two consecutive stool samples for Kato±Katz thick smears. For all samples it was found that 54.4% of individuals were infected with S. mansoni. Moreover, individuals infected with S. mansoni reported ``bloody diarrhoea'', ``blood in stools'' and ``schistosomiasis'' significantly more often than uninfected children. At the school level, Spearman rank correlation analysis showed that the prevalence of S. mansoni significantly correlated with the prevalence of reported bloody diarrhoea (P = 0.002), reported blood in stools (P = 0.014) and reported schistosomiasis (P = 0.011). Reported bloody diarrhoea and reported blood in stools had the best diagnostic performance (sensitivity: 88.2%, specificity: 57.7%, positive predictive value: 73.2%, negative predictive value: 78.9%). -

HUMANITARIAN UPDATE Covering 7-21 March 2019 | Issue 5
YEMEN HUMANITARIAN UPDATE Covering 7-21 March 2019 | Issue 5 KEY ISSUES: • Suspected cholera and acute watery diarrhea cases increased; 108,889 suspected cases were reported between 1 January and 17 March. • According to local authorities, more than 9,700 families were recently displaced to 18 districts in Hajjah Governorate; most live in open spaces and public buildings. • Yemen’s economic situation continues to disintegrate due to the ongoing conflict; GDP has contracted by an estimated 39 per cent since 2014. • The Protection Cluster reports that more than 4,800 civilian deaths and injuries occurred during 2018, an average of 93 civilian casualties per week. • UNICEF paid incentives to 97,000 out of a target of 136,000 teachers who had not received their salary in two years. INCREASE IN SUSPECTED CHOLERA CASES Two years after Yemen suffered its worst cholera Amanat Al Asimah, Al Hudaydah, Sana’a, Ibb, Amran outbreak, the number of reported suspected cases of and Dhamar—which together account for nearly two cholera and acute watery diarrhoea spiked in recent thirds of reported cases. weeks. Data collected by the Ministry of Public Health and Population with the support of WHO indicates that The recent increase in suspected cholera cases is 108,889 suspected cases and 190 associated deaths possibly linked to early rains, increased awareness were recorded between 1 January and 17 March. among the population and therefore a willingness to About one third of the cases are children under age 5. seek testing and treatment, and enhanced disease surveillance. The situation is exacerbated by poor Cholera is endemic in Yemen. -

Visceral and Cutaneous Larva Migrans PAUL C
Visceral and Cutaneous Larva Migrans PAUL C. BEAVER, Ph.D. AMONG ANIMALS in general there is a In the development of our concepts of larva II. wide variety of parasitic infections in migrans there have been four major steps. The which larval stages migrate through and some¬ first, of course, was the discovery by Kirby- times later reside in the tissues of the host with¬ Smith and his associates some 30 years ago of out developing into fully mature adults. When nematode larvae in the skin of patients with such parasites are found in human hosts, the creeping eruption in Jacksonville, Fla. (6). infection may be referred to as larva migrans This was followed immediately by experi¬ although definition of this term is becoming mental proof by numerous workers that the increasingly difficult. The organisms impli¬ larvae of A. braziliense readily penetrate the cated in infections of this type include certain human skin and produce severe, typical creep¬ species of arthropods, flatworms, and nema¬ ing eruption. todes, but more especially the nematodes. From a practical point of view these demon¬ As generally used, the term larva migrans strations were perhaps too conclusive in that refers particularly to the migration of dog and they encouraged the impression that A. brazil¬ cat hookworm larvae in the human skin (cu¬ iense was the only cause of creeping eruption, taneous larva migrans or creeping eruption) and detracted from equally conclusive demon¬ and the migration of dog and cat ascarids in strations that other species of nematode larvae the viscera (visceral larva migrans). In a still have the ability to produce similarly the pro¬ more restricted sense, the terms cutaneous larva gressive linear lesions characteristic of creep¬ migrans and visceral larva migrans are some¬ ing eruption. -

June 2013 - February 2014
Yemen outbreak June 2013 - February 2014 Desert Locust Information Service FAO, Rome www.fao.org/ag/locusts Keith Cressman (Senior Locust Forecasting Officer) SAUDI ARABIA spring swarm invasion (June) summer breeding area Thamud YEMEN Sayun June 2013 Marib Sanaa swarms Ataq July 2013 groups April and May 2013 rainfall totals adults 25 50 100+ mm Aden hoppers source: IRI RFE JUN-JUL 2013 Several swarms that formed in the spring breeding areas of the interior of Saudi Arabia invaded Yemen in June. Subsequent breeding in the interior due to good rains in April-May led to an outbreak. As control operations were not possible because of insecurity and beekeepers, hopper and adult groups and small hopper bands and adult swarms formed. DLIS Thamud E M P T Y Q U A R T E R summer breeding area SEP Suq Abs Sayun winter Marib Sanaa W. H A D H R A M A U T breeding area Hodeidah Ataq Aug-Sep 2013 swarms SEP bands groups adults Aden breeding area winter hoppers AUG-SEP 2013 Breeding continued in the interior, giving rise to hopper bands and swarms by September. Survey and control operations were limited due to insecurity and beekeeping and only 5,000 ha could be treated. Large areas could not be accessed where bands and swarms were probably forming. Adults and adult groups moved to the winter breeding areas along the Red Sea and Gulf of Aden coasts where early first generation egg-laying and hatching caused small hopper groups and bands to DLIS form. Ground control operations commenced on 27 September. -

Newsletter-2013-Q4 0.977 MB
SOCIAL FUND FOR DEVELOPMENT 16 pages Newsletter – Edition No. 64, October– December 2013 EDITORIAL SFD’s BoD Holds a Meeting Reading the sectoral distribution The Board of Directors (BoD) of the Social Fund for Development (SFD) held of SFD’s 2013 investments a meeting on November 25, 2013 headed by Mohammed Salem Basendwah, Prime Minister and BoD Chairman. The meeting discussed SFD’s draft budget (commitments), one finds that the for 2014 financial year, which amounts to 36.6 billion Yemeni Riyals (equivalent annual share of each of the Cash-for- to $170.4 million)––increasing by 9% compared to 2013 budget. Work (CfW) Program and water has The draft budget is expected to finance the implementation of 1,391 projects nationwide distributed among the sectors of education, water and environment, been steadily increasing since 2011. health, roads, training and institutional support, microfinance, special-need For instance, while the share of SFD’s groups, labor-intensive works program, agriculture & the integrated interventions contribution to the CfW in 2011 was program. 8%, in 2013 it has reached 20.4%. As The meeting praised the successes achieved by the SFD and its vital role in contributing to poverty alleviation through the provision of job opportunities as for water, there has been an increase well as its active developmental role in improving the living conditions of poor from 13% to 18% for the same period. communities by providing basic needs, facilitating access to social services and raising income through creating temporary and permanent employment. This clearly emphasizes the increasing role of SFD in providing safety net to the most vulnerable Yemenis and responding to critical needs in the country. -
USG Yemen Complex Emergency Program
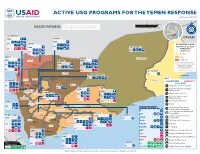
ACTIVE USG PROGRAMS FOR THE YEMEN RESPONSE Last Updated 02/12/20 0 50 100 mi INFORMA Partner activities are contingent upon access to IC TI PH O A N R U G SAUDI ARABIA conict-aected areas and security concerns. 0 50 100 150 km N O I T E G U S A A D ID F /DCHA/O AL HUDAYDAH IOM AMRAN OMAN IOM IPs SA’DAH ESTIMATED FOOD IPs SECURITY LEVELS IOM HADRAMAWT IPs THROUGH IPs MAY 2020 IPs Stressed HAJJAH Crisis SANA’A Hadramawt IOM Sa'dah AL JAWF IOM Emergency An “!” indicates that the phase IOM classification would likely be worse IPs Sa'dah IPs without current or planned IPs humanitarian assistance. IPs Source: FEWS NET Yemen IPs AL MAHRAH Outlook, 02/20 - 05/20 Al Jawf IP AMANAT AL ASIMAH Al Ghaedha IPs KEY Hajjah Amran Al Hazem AL MAHWIT Al Mahrah USAID/OFDA USAID/FFP State/PRM Marib IPs Hajjah Amran MARIB Agriculture and Food Security SHABWAH IPs IBB Camp Coordination and Camp Al Mahwit IOM IPs Sana'a Management Al Mahwit IOM DHAMAR Sana'a IPs Cash Transfers for Food Al IPs IPs Economic Recovery and Market Systems Hudaydah IPs IPs Food Voucher Program RAYMAH IPs Dhamar Health Raymah Al Mukalla IPs Shabwah Ataq Dhamar COUNTRYWIDE Humanitarian Coordination Al Bayda’ and Information Management IP Local, Regional, and International Ibb AD DALI’ Procurement TA’IZZ Al Bayda’ IOM Ibb ABYAN IOM Al BAYDA’ Logistics Support and Relief Ad Dali' OCHA Commodities IOM IOM IP Ta’izz Ad Dali’ Abyan IPs WHO Multipurpose Cash Assistance Ta’izz IPs IPs UNHAS Nutrition Lahij IPs LAHIJ Zinjubar UNICEF Protection IPs IPs WFP Ready-to-Use Therapeutic Food IOM Al-Houta ADEN FAO Refugee and Migrant Assistance IPs Aden IOM UNICEF Risk Management Policy and Practice Shelter and Settlements IPs WFP SOCOTRA DJIBOUTI, ETHIOPIA, U.S. -

Livelihoods Assistance – Active Partners Reporting for January 2021
Partners Monthly Presence (4W Map): Livelihoods Assistance – Active Partners 6 6 6 6 6 6 6 6 1 1 1 1 1 1 1 1 N Amran Reporting for January 2021 <Sadjhg 0 0 0 0 0 0 0 0 E 2 2 2 2 2 2 2 2 r r r r r r r r Saáda 4 partners M e e e e e e e 4 partners Amanat Al asimah 2 partners e Amran A E b b b b b b b b Partners by type & volume of response SFD, UNDP/SFD, WFP/Oxfam 7 partners Y Sana'a m m m m m m m SFD, UNDP/SFD, UNDP/SFD m e e e e e e e WFP/Oxfam e UNDP/SFD, WFP/IRY, WFP/RI Partner Type Volume of Response c c c c c c c c e e e e e e e e 30% INGOs D D D D D D D D FAO/Ghadaq - - - - - - - - NNGOs 4% s s s s s s s s e e e e e e e Hajjah 8 partners e i i i i i i i i t t t t t t t t Amran UN Agencies and partners i i i i i i i i 66% v v v v v v v CARE, HAY, SFD, UNDP/SFD, v i i i i i i i i t t t t t t t WFP/RI t c c c c c c c c Sa'ada a a a a a a a CARE, FAO/RADF a r r r r r r r r e e e e e e e Ale Jawf st st st st st st st st u u u u u u u u l l l l l l l Al Mahwit 5 partners Al Jawf l 2 partners Al Maharah C C C C C C C C CARE, UNDP/SFD, WFP/Care, e e e e e e e SFD, UNDP/SFDe Hadramaut WFP/SDF r r r r r r r r u u u u u u u Hajjah u Amran 9 partners t t t t t t t Amran t Hadramaut l l l l l l l CARE l u u u u u u u u UNDP/SFD, WFP/BCHR, c c c c c c c c i i i i i i i 6 partners i WFP/FMF r r r r r r r Dhamar r Amanat g g g g g g g SFD, UNDP/SFD, g YLDF A A A A A A A A ! WFP/IRY, WFP/SDF Al Asimah . -

Amran, Al Mahwit, Hajjah and Sa'ada
YEMEN - Amran, Al Mahwit, Hajjah and Sa'ada governorates For Humanitarian Use Only The lowest temperatures recorded between December and February (1970-2000) Production date : 04 October 2017 Final District Final District Governorate District Governorate District Priority Priority Al Mahwit Al Khabt Medium Sa'ada Al Dhaher Low or none Al Mahwit Al Mahwait Medium Sa'ada Al Hashwah High Al Mahwit Al Mahwait City Critical Sa'ada As Safra Critical Al Mahwit Ar Rujum Medium Sa'ada Baqim Critical Qatabir Baqim Al Mahwit At Tawilah High Sa'ada Ghamr Medium Al Mahwit Bani Sa'd Critical Sa'ada Haydan Medium Al Mahwit Hufash High Sa'ada Kitaf wa Al Boqe'e Critical Al Mahwit Milhan Medium Sa'ada Majz Critical Al Mahwit Shibam Kawkaban Medium Sa'ada Monabbih Medium Kitaf wa Amran Al Ashah Critical Sa'ada Qatabir Medium As Safra Al Boqe'e Majz Amran Al Madan Critical Sa'ada Razih Medium Monabbih Amran Al Qaflah Critical Sa'ada Sa'adah Critical Amran Amran Critical Sa'ada Sahar Critical Ghamr Amran As Sawd High Sa'ada Saqayn Critical As Safra Sa'ada Amran As Sudah Medium Sa'ada Shada'a Low or none Razih Sa'adah Amran Bani Suraim Medium Amran Dhi Bin Critical Shada'a Saqayn Al Hashwah Amran Habur Zulaymah High Sahar Amran Harf Sufyan Critical Amran Huth Critical Amran Iyal Surayh Critical Amran Jabal Iyal Yazid Critical Al Dhaher Haydan Amran Khamir Critical Amran Kharif Critical Amran Maswar Critical Amran Raydah Critical Bakil Al Mir Harf Amran Shaharah High Sufyan Amran Suwayr Critical Al Ashah Amran Thula High Haradh Qarah Hajjah Abs Critical Hajjah