Pentasomy X FTNP
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The National Economic Burden of Rare Disease Study February 2021
Acknowledgements This study was sponsored by the EveryLife Foundation for Rare Diseases and made possible through the collaborative efforts of the national rare disease community and key stakeholders. The EveryLife Foundation thanks all those who shared their expertise and insights to provide invaluable input to the study including: the Lewin Group, the EveryLife Community Congress membership, the Technical Advisory Group for this study, leadership from the National Center for Advancing Translational Sciences (NCATS) at the National Institutes of Health (NIH), the Undiagnosed Diseases Network (UDN), the Little Hercules Foundation, the Rare Disease Legislative Advocates (RDLA) Advisory Committee, SmithSolve, and our study funders. Most especially, we thank the members of our rare disease patient and caregiver community who participated in this effort and have helped to transform their lived experience into quantifiable data. LEWIN GROUP PROJECT STAFF Grace Yang, MPA, MA, Vice President Inna Cintina, PhD, Senior Consultant Matt Zhou, BS, Research Consultant Daniel Emont, MPH, Research Consultant Janice Lin, BS, Consultant Samuel Kallman, BA, BS, Research Consultant EVERYLIFE FOUNDATION PROJECT STAFF Annie Kennedy, BS, Chief of Policy and Advocacy Julia Jenkins, BA, Executive Director Jamie Sullivan, MPH, Director of Policy TECHNICAL ADVISORY GROUP Annie Kennedy, BS, Chief of Policy & Advocacy, EveryLife Foundation for Rare Diseases Anne Pariser, MD, Director, Office of Rare Diseases Research, National Center for Advancing Translational Sciences (NCATS), National Institutes of Health Elisabeth M. Oehrlein, PhD, MS, Senior Director, Research and Programs, National Health Council Christina Hartman, Senior Director of Advocacy, The Assistance Fund Kathleen Stratton, National Academies of Science, Engineering and Medicine (NASEM) Steve Silvestri, Director, Government Affairs, Neurocrine Biosciences Inc. -

Klinefelter Syndrome) at 9 Years of Age
17th SSBP International Research Symposium Developmental trajectories of behavioural phenotypes Programme Book 10–13 October 2014 • New York, USA 2 17th International SSBP Research Symposium The Society for the Study 3 of Behavioural Phenotypes 10th – 13th October 2014 The 17th SSBP International Meeting Developmental Trajectories of Behavioural Phenotypes New York, USA 10th – 13th October 2014, New York, USA Contents Contents Welcome ........................................................................................................................................................................................................9 New York Conference Organiser ..............................................................................................................................................10 Scientific Committee ..........................................................................................................................................................................11 4 The SSBP .......................................................................................................................................................................................................12 The SSBP Executive Committee : ...........................................................................................................................................................................12 Meetings of the SSBP ....................................................................................................................................................................................................13 -

Orphanet Report Series Rare Diseases Collection
Marche des Maladies Rares – Alliance Maladies Rares Orphanet Report Series Rare Diseases collection DecemberOctober 2013 2009 List of rare diseases and synonyms Listed in alphabetical order www.orpha.net 20102206 Rare diseases listed in alphabetical order ORPHA ORPHA ORPHA Disease name Disease name Disease name Number Number Number 289157 1-alpha-hydroxylase deficiency 309127 3-hydroxyacyl-CoA dehydrogenase 228384 5q14.3 microdeletion syndrome deficiency 293948 1p21.3 microdeletion syndrome 314655 5q31.3 microdeletion syndrome 939 3-hydroxyisobutyric aciduria 1606 1p36 deletion syndrome 228415 5q35 microduplication syndrome 2616 3M syndrome 250989 1q21.1 microdeletion syndrome 96125 6p subtelomeric deletion syndrome 2616 3-M syndrome 250994 1q21.1 microduplication syndrome 251046 6p22 microdeletion syndrome 293843 3MC syndrome 250999 1q41q42 microdeletion syndrome 96125 6p25 microdeletion syndrome 6 3-methylcrotonylglycinuria 250999 1q41-q42 microdeletion syndrome 99135 6-phosphogluconate dehydrogenase 67046 3-methylglutaconic aciduria type 1 deficiency 238769 1q44 microdeletion syndrome 111 3-methylglutaconic aciduria type 2 13 6-pyruvoyl-tetrahydropterin synthase 976 2,8 dihydroxyadenine urolithiasis deficiency 67047 3-methylglutaconic aciduria type 3 869 2A syndrome 75857 6q terminal deletion 67048 3-methylglutaconic aciduria type 4 79154 2-aminoadipic 2-oxoadipic aciduria 171829 6q16 deletion syndrome 66634 3-methylglutaconic aciduria type 5 19 2-hydroxyglutaric acidemia 251056 6q25 microdeletion syndrome 352328 3-methylglutaconic -

XXXXX Syndrome
XXXXX Syndrome 49,XXXXX (pentasomy X) is a rare sex chromosome aneu- 2. Craniofacial features ploidy. The birth prevalence of pentasomy X is estimated to be a. Microcephaly 1 in 85,000 females. b. Flattened occiput c. Epicanthus d. Upslanting palpebral fissures GENETICS/BASIC DEFECTS e. Ocular hypertelorism 1. Etiology: Three extra X chromosomes are responsible for f. Uncoordinated eye movements the pentasomy X syndrome. g. Flat broad nose 2. Occurrence of a 49,XXXXX complement: secondary to h. Cleft palate sequential non-disjunctions in meiosis I and meiosis II in i. Low-set ears the mother j. Malformed teeth a. Involves the survival of both X chromosomes in a sin- 3. Skeletal abnormalities gle oocytes through both meiotic divisions a. Short neck i. Once between homologous X chromosomes at b. Lax joints the first meiosis c. Multiple dislocations ii. Twice between sister chromatids in both X chro- i. Shoulders mosomes in the secondary oocytes at the second ii. Elbows meiosis iii. Hips b. Followed by the fertilization by a sperm contributing d. Radioulnar synostosis the 5th chromosome X e. Spinal abnormalities 3. Formation of four Barr bodies f. Clinodactyly of the 5th fingers a. Lyon hypothesis g. Lower leg abnormalities i. Inactivation of all X chromosomes but one i. Genu valgus ii. Account for the viability of the X-chromosome ii. Talipes aneuploidies iii. Metatarsus varus b. Inactivation of four X chromosomes resulting in four h. Delayed bone age Barr bodies 4. Congenital heart defects 4. Effect of supernumerary X chromosomes: a direct rela- a. Ventricular septal defect tionship between the number of supernumerary X chro- b. -
Example Document Medical Genetics Center
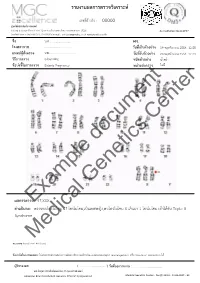
รายงานผลการตรวจววเคราะหย เลขทธรออางอนง : 00000 ศผนยยพวนธธศาสตรยการแพทยย 6/6 หมนม 6 ถนนสสขาภนบาล 5 ซอย 32 แขวงออเงนน เขตสายไหม กรสงเทพมหานคร 10220 Accreditation No.4148/57 โทรศกพทย/โทรสาร 086-8861203, 02-7920726 e-mail : [email protected] www.genetics.co.th ชชชอ น.ส............................. HN. ............. โรงพยาบาล .................................... ววนททชเกกบตววอยยาง 19 พฤศจนกายน 2558 12:55 แพทยยผผผสวชงตรวจ นพ.................................... ววนททชรวบตววอยยาง 20 พฤศจนกายน 2558 12:43 ววธทการตรวจ G-banding ชนวดตววอยยาง นนนาครรนา ขผอบยงชทชในการตรวจ Elderly Pregnancy หนยวยสยงตรวจ ไมมมธ Center document Genetics ผลการตรวจExample: 47,XXX คคาอธวบาย : ตรวจพบโครโมโซม 47 โครโมโซม,เปปนเพศหญนง,พบโครโมโซม X เกนนมา 1 โครโมโซม เขอาไดอกกบ Triple X Syndrome Medical หมายเหตธ: Band level 450 band ขผอจคากวดในการทดสอบ: ไมมสามารถตรวจสอบความผนดปกตนขนาดเลลกชนนด submicroscopic rearrangement หรรอ low-level mosaicism ไดอ ผผผรวบรองผล ( .................................. ) ววนททชออกรายงาน : ....................................... นพ.วทรยธทธ ประพวนธยพจนย,พบ.,วว.กธมารเวชศาสตรย American Board of Medical Genetics (Clinical Cytogenetics) Medical Genetics Center : Fo-QP-19/01 : 16-03-2015 : 02 เรียน อ.นพ...................................... ที่นับถือ ตามที่ผลตรวจโครโมโซมจากน ้าคร่้าของ นส........................ (HN .............., Lab no. ..............) พบ โครโมโซม X เกินมา 1 โครโมโซมนั น ความผิดปกติดังกล่าว เข้าได้กับกลุ่มอาการ trisomy X หรือ triple X syndrome ซึ่งเป็นความผิดปกติของโครโมโซมเพศที่พบได้บ่อยในทารกเพศหญิง โดยความผิดปกติของ โครโมโซมแบบนี -

Inside This Issue
Winter 2014 No. 77 Inside this issue Group News | Fundraising | Members’ Letters | One Family Living with Two Different Chromosome Disorders | Bristol Conference 2014 | Unique Leaflets | Christmas Card Order Form Sophie, Unique’s Chair of Trustees Dear Members, In the past month a few things have reminded me of why it is so important to make connections through Unique but also to draw support from other parents around us. I’ve just returned from Unique’s most recent family conference in Bristol where 150 of us parents and carers had a lovely time in workshops, meals and activities, chatting and watching our children milling around together like one big family since – although we had never met before – we have shared so many experiences in common. However in contrast I have also just met a new mum who has just moved to my area from far away with two toddlers, one with a rare joys of the internet, it is becoming easier to meet others with similar, chromosome disorder, who is starting from scratch with no even very rare, chromosome disorders around the world and to find professional, medical or social support. She reminds me of how yourself talking to them in the middle of the night about some lonely I felt when Max was newly diagnosed, when I knew no one interesting things our children share in common (obsession with with a disabled child let alone anyone with a rare chromosome catalogues, anyone?) And of course we also have an enormous disorder. Elsewhere our latest Unique Facebook group, Unique amount in common with so many parents of children with other Russia, is also just starting up – so far it includes just a small special needs or disabilities around us in our own communities who number of members sharing very different experiences to mine here will often be walking the same path as us. -

Female Polysomy-X and Systemic Lupus Erythematosus
Seminars in Arthritis and Rheumatism 43 (2014) 508–512 Contents lists available at ScienceDirect Seminars in Arthritis and Rheumatism journal homepage: www.elsevier.com/locate/semarthrit Female polysomy-X and systemic lupus erythematosus Mordechai Slae, MDa,n, Merav Heshin-Bekenstein, MDb, Ari Simckes, MDb, Gali Heimer, MDb, Dan Engelhard, MDb, Eli M. Eisenstein, MDc a Department of Pediatrics, University of Alberta Hospital, Edmonton, Alberta, Canada b Department of Pediatrics, Hadassah-Hebrew University Hospital at Ein Kerem, Jerusalem, Israel c Department of Pediatrics, Hadassah-Hebrew University Hospital at Mount-Scopus, Jerusalem, Israel article info abstract Objectives: Systemic lupus erythematosus (SLE) occurs more commonly in females than in males. Recent Keywords: evidence suggests that genetic factors transmitted by the X-chromosome may confer increased risk for Gene dosage autoimmune disease in general, and for SLE in particular. It is therefore possible that X-chromosome Lupus genetics polysomy might confer further increased risk for lupus. In addition to describing the clinical and Polysomy-X immunologic features of a young woman with polysomy-X and SLE, we sought to review all other Sex differences published cases associating female or male polysomy-X with SLE or other forms of autoimmunity. SLE Methods: We report a case of a prepubertal girl with polysomy-X and SLE. We performed a systemic X-chromosome literature review for cases of polysomy-X and SLE and summarize previously published cases. In addition, we reviewed reports concerning the possible association between SLE and other connective tissue diseases and male polysomy-X. Results: An 11-year-old girl with tetrasomy-X (48 XXXX karyotype) presented with prolonged fever. -

Genetic Evaluation of Inpatient Neonatal and Infantile Congenital Heart Defects: New Findings and Review of the Literature
G C A T T A C G G C A T genes Article Genetic Evaluation of Inpatient Neonatal and Infantile Congenital Heart Defects: New Findings and Review of the Literature Benjamin M. Helm 1,2,*, Benjamin J. Landis 3 and Stephanie M. Ware 1,3 1 Department of Medical and Molecular Genetics, Indiana University School of Medicine, Indianapolis, IN 46202, USA; [email protected] 2 Department of Epidemiology, Indiana University Fairbanks School of Public Health, Indianapolis, IN 46202, USA 3 Department of Pediatrics, Indiana University School of Medicine, Indianapolis, IN 46202, USA; [email protected] * Correspondence: [email protected]; Tel.: +1-317-944-3966 Abstract: The use of clinical genetics evaluations and testing for infants with congenital heart defects (CHDs) is subject to practice variation. This single-institution cross-sectional study of all inpatient infants with severe CHDs evaluated 440 patients using a cardiovascular genetics service (2014–2019). In total, 376 (85.5%) had chromosome microarray (CMA), of which 55 (14.6%) were diagnostic in syndromic (N = 35) or isolated (N = 20) presentations. Genetic diagnoses were made in all CHD classes. Diagnostic yield was higher in syndromic appearing infants, but geneticists’ dysmorphology exams lacked complete sensitivity and 6.5% of isolated CHD cases had diagnostic CMA. Interestingly, diagnostic results (15.8%) in left ventricular outflow tract obstruction (LVOTO) defects occurred most Citation: Helm, B.M.; Landis, B.J.; often in patients with isolated CHD. Geneticists’ evaluations were particularly important for second- Ware, S.M. Genetic Evaluation of Inpatient Neonatal and Infantile tier molecular testing (10.5% test-specific yield), bringing the overall genetic testing yield to 17%. -

False Low-Risk Single Nucleotide Polymorphism–Based Noninvasive Prenatal Screening in Pentasomy 49,XXXXY
THIEME e4 Case Report False Low-Risk Single Nucleotide Polymorphism–Based Noninvasive Prenatal Screening in Pentasomy 49,XXXXY Manesha Putra, MD1 Melissa A. Hicks, MS2 Jacques S. Abramowicz, MD3 1 Department of Obstetrics and Gynecology, Detroit Medical Center, Address for correspondence Manesha Putra, MD, Department of Wayne State University, Detroit, Michigan Obstetrics and Gynecology, Detroit Medical Center, Wayne State 2 Detroit Medical Center University Laboratories, Detroit Medical University, 3990 John R, 7-Brush N, Detroit, MI 48201 Center,Detroit,Michigan (e-mail: [email protected]). 3 Department of Obstetrics and Gynecology, University of Chicago, Chicago, Illinois Am J Perinatol Rep 2018;8:e4–e6. Abstract Introduction Pentasomy 49,XXXXY is a sex chromosome anomaly difficult to be diagnosed prenatally. We describe a patient of pentasomy 49,XXXXY with false low-risk Keywords results using a noninvasive prenatal screening (NIPS). A 30-year-old G1P0 woman presented ► sex chromosome at 336/7 weeks, secondary to sonographic fetal anomalies. She had low-risk NIPS at 136/7 aneuploidy weeks. Anatomy survey showed bilateral clubfeet, clinodactyly of the left fifth digit, ► NIPT micropenis, and echogenic bowel. Cytogenetics analysis revealed pentasomy 49,XXXXY ► prenatal diagnosis syndrome. We report third-trimester sonographic features of a fetus with pentasomy ► screening 49,XXXXY and the importance of thorough pre- and posttest counseling for NIPS. The advent of noninvasive prenatal screening (NIPS, some- natal features described in the literature include cystic times abbreviated as NIPT or NIPS) for aneuploidy has made a hygroma, microgenitalia, clubfoot, epignathus, nonimmune substantial impact in maternal–fetal medicine practice by hydrops, and hypoplastic right heart syndrome.5 Confirma- significantly decreasing the number of second-trimester inva- tory prenatal diagnosis relies on amniocentesis and fetal sive diagnostic tests performed.1 Nevertheless, the American chromosomal studies. -

蝪case Report D
å¡ CASE REPORT D Pentasomy X Mosaic in Two Adult Sisters with Diabetes Mellitus Shigeru Nakano, Atsuko Sasame, Sadahide Azukizawa, Toshikazu Kigoshi, Kenzo Uchida, Hiroaki Takahashi* and Shinpei Morimoto Pentasomy X mosaic in two adult sisters with non-insulin dependent diabetes mellitus is described. The younger sister had schizophrenia, and both were mentally retarded, but no apparent somatic abnormalities were found. Chromosome analyses revealed karyotype 45,X/ 46,XX/47,XXX/48,XXXX/49,XXXXX mosaic with a low frequency of aneuploidy on cultured peripheral lymphocytes and 46,XX on cultured skin fibroblasts in both sisters. The low fre quency of X chromosome aberration may be responsible for the lack of somatic abnormalities and the long life in both sisters. The association of pentasomy X mosaicism and diabetes mellitus (Internalhowever Medicineappears to 31: be 1102-1106,coincidental. 1992) Key words: X chromosome aneuploidy, aged siblings, glucose intolerance Intr oduction her behavior was quiet, shy and timid. Intelligence quotient (IQ) obtained from the results of WAIS-R Pentasomy X and its mosaicism, rare X chromosomal tests was 55, verbal IQ 62 and performance IQ 50. Her constitutions, are generally found in young (neonate to height was 143 cm, weight 38 kg and head circumference childhood) females because of concomitant mental 53cm. Her blood pressure was 98/58mmHg; the pulse and somatic abnormalities; mental retardation and rate was 74 beats/min and regular. She had no apparent mongoloid face, congenital heart disease and various somatic abnormalities (Fig. 1). Her fundus oculi showed skeletal anomalies are associated (1-10). However, preproliferative diabetic retinopathy. -

The Frequency of Aneuploidy in Cultured Lymphocytes Is Correlated with Age and Gender but Not with Reproductive History
Am. J. Hum. Genet. 46:1101-11, 1990 The Frequency of Aneuploidy in Cultured Lymphocytes Is Correlated with Age and Gender but Not with Reproductive History Gregory R Nowinski,$* Daniel L. Van Dyke, * Barbara C. Tilley, * Gordon Jacobsen,* V. Ramesh Babu,* Maria J. Worsham,* Golder N. Wilsont and Lester Weiss* * Medical Genetics and Birth Defects Center, and Division of Biostatistics and Research Epidemiology, Henry Ford Hospital, Detroit; and tDepartment of Pediatrics, University of Texas Southwestern Medical Center, Dallas Summary The clinical significance of low numbers of aneuploid cells in routine cytogenetic studies of cultured lym- phocytes is not always clear. We compared the frequencies of chromosome loss and gain among five groups of subjects whose karyotypes were otherwise normal; these groups were (1) subjects studied because of multiple miscarriages, (2) parents of live borns with autosomal trisomy, (3) subjects studied because they had a relative with Down syndrome, (4) an age-matched control group of phenotypically normal adults studied for other reasons (e.g., parent of a dysmorphic child or member of a translocation family), and (5) other mostly younger and phenotypically abnormal subjects who could not be assigned to the first four groups (e.g., individuals with multiple congenital anomalies or mental retardation). No significant age, sex, or group effects were observed for autosomal loss (hypodiploidy) or gain (hyperdiploidy). Au- tosomal loss was inversely correlated with relative chromosome length, but autosomal gain was not. Sex- chromosome gain was significantly more frequent in females than in males, but sex-chromosome loss was not significantly different between the sexes. Significant age effects were observed for both gain and loss of sex chromosomes. -

A New Case of Prenatally Diagnosed Pentasomy X: Review of the Literature
Hindawi Publishing Corporation Case Reports in Obstetrics and Gynecology Volume 2015, Article ID 935202, 5 pages http://dx.doi.org/10.1155/2015/935202 Case Report A New Case of Prenatally Diagnosed Pentasomy X: Review of the Literature Linda Maria Azzurra Pirollo,1 Leila Baghernajad Salehi,2 Simona Sarta,1 Marco Cassone,3 Maria Vittoria Capogna,1 Emilio Piccione,1 Giuseppe Novelli,4 and Adalgisa Pietropolli1 1 Section of Gynecology and Obstetrics, Academic Department of Biomedicine and Prevention and Clinical Department of Surgery, Tor Vergata University Hospital, Viale Oxford 81, 00133 Rome, Italy 2Laboratory of Medical Genetics, Polyclinic of Tor Vergata Foundation, Viale Oxford 81, 00133 Rome, Italy 3Laboratory of Medical Genetics, University of Rome Tor Vergata, Via Montpellier 1, 00133 Rome, Italy 4Genetics Section, Department of Biomedicine and Prevention, University of Rome Tor Vergata, Via Montpellier 1, 00133 Rome, Italy Correspondence should be addressed to Linda Maria Azzurra Pirollo; [email protected] Received 2 December 2014; Revised 13 January 2015; Accepted 14 January 2015 Academic Editor: Olivier Picone Copyright © 2015 Linda Maria Azzurra Pirollo et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Pentasomy X is a rare chromosomal abnormality probably due to a nondisjunction during the meiosis. Only four cases prenatally diagnosed were described until now. Our case is the fifth one prenatally diagnosed at 20 weeks of gestational age in a 39-years- old woman. She underwent invasive prenatal diagnosis for her advanced maternal age without any other known risk factor.