A Study of the Anatomical Variations of the Carotid Arterial Tree in Equidae
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Evaluation of Artery Visualizations for Heart Disease Diagnosis
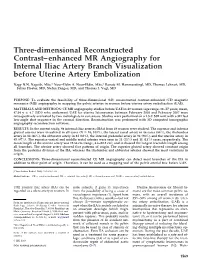
Evaluation of Artery Visualizations for Heart Disease Diagnosis Michelle A. Borkin, Student Member, IEEE, Krzysztof Z. Gajos, Amanda Peters, Dimitrios Mitsouras, Simone Melchionna, Frank J. Rybicki, Charles L. Feldman, and Hanspeter Pfister, Senior Member, IEEE Fig. 1. Left: Traditional 2D projection (A) of a single artery, and 3D representation (C) of a right coronary artery tree with a rainbow color map. Right: 2D tree diagram representation (B) and equivalent 3D representation (D) of a left coronary artery tree with a diverging color map. Abstract—Heart disease is the number one killer in the United States, and finding indicators of the disease at an early stage is critical for treatment and prevention. In this paper we evaluate visualization techniques that enable the diagnosis of coronary artery disease. A key physical quantity of medical interest is endothelial shear stress (ESS). Low ESS has been associated with sites of lesion formation and rapid progression of disease in the coronary arteries. Having effective visualizations of a patient’s ESS data is vital for the quick and thorough non-invasive evaluation by a cardiologist. We present a task taxonomy for hemodynamics based on a formative user study with domain experts. Based on the results of this study we developed HemoVis, an interactive visualization application for heart disease diagnosis that uses a novel 2D tree diagram representation of coronary artery trees. We present the results of a formal quantitative user study with domain experts that evaluates the effect of 2D versus 3D artery representations and of color maps on identifying regions of low ESS. We show statistically significant results demonstrating that our 2D visualizations are more accurate and efficient than 3D representations, and that a perceptually appropriate color map leads to fewer diagnostic mistakes than a rainbow color map. -

Non-Surgical Treatment of Guttural Pouch Empyema with Presence of Chondroids in a Filly
Acta Scientiae Veterinariae, 2020. 48(Suppl 1): 553. CASE REPORT ISSN 1679-9216 Pub. 553 Non-surgical Treatment of Guttural Pouch Empyema with Presence of Chondroids in a Filly Heitor Cestari, Isabella Barros de Sousa Pereira, Letícia Hirata Mendes, Nathalia Cardoso de Souza, Joel Phillipe Costa e Souza, Carlos Alberto Escada Baumam & Marcos Jun Watanabe ABSTRACT Background: Guttural pouch empyema in horses is a disease described by the accumulation of purulent/mucopurulent exudate, which with chronification of the disease can become chondroids, affecting horses of any age and not presenting breed predisposition. The main cause of empyema is upper respiratory infection, associated or not with failure in the de- fense mechanisms, as well as drainage to the guttural pouch of retropharyngeal lymph node abscesses; the main pathogen related to this condition is Streptococcus equi. This paper aims to describes a case of a filly that presented a mucopurulent nasal discharge, five months of evolution, and irresponsive to antibiotic therapy. Case: A 2.5-year-old quarter filly was referred to the veterinary hospital presenting a 5 months evolution mucopurulent nasal discharge, irresponsive to gentamicin and ceftiofur, and later doxycycline, acetylcysteine and clenbuterol that were instituted on the farm. Throw the endoscopic examination of the upper respiratory tract, was observed the presence of mucopurulent content and chondroids inside the right guttural pouch. This material was collected and sent for culture and antibiogram tests. Streptococcus equi was isolated, and was only sensitive to ceftiofur. The treatment included the guttural pouches flushes with warm saline solution (0.9%) associated with Lauryl Dietylene Glycol Ether Sulfate Sodium (28%) and acetylcysteine (10%). In addition to topical treatment, 5 mg/kg of ceftiofur was administered intramuscularly daily for 7 days. -

Guttural Pouch Mycosis in a Donkey (Equus Asinus): a Case Report
Veterinarni Medicina, 55, 2010 (11): 561–565 Case Report Guttural pouch mycosis in a donkey (Equus asinus): a case report F. Laus, E. Paggi, M. Cerquetella, D. Spaziante, A. Spaterna, B. Tesei School of Veterinary Medical Sciences, University of Camerino, Camerino, Italy ABSTRACT: Guttural pouch mycosis is an emergency disease of the upper respiratory tract in equine species. In the present report a case of guttural pouch mycosis in a female, seven year-old pregnant donkey is described. A serious dyspnea which necessitated tracheotomy and preceding epistaxis was the most important clinical fea- ture of guttural pouch mycosis in the donkey. A full and rapid effectiveness of the topical therapy, the protocol for which is described, is the main distinguishing feature with regard to treatment. In the Authors’ knowledge a detailed description of clinical features, treatment and follow up of guttural pouch mycosis in a donkey is not available in the scientific literature. The anatomical and physiological peculiarity of donkeys could explain some of the differences with horses in clinical presentation and therapeutic management. Keywords: donkey; guttural pouches; respiratory disease Guttural pouch mycosis (GPM) is an infrequent bolization techniques are the most frequently used disease of horses reported to be fatal in 50% of cases (Hardy and Leveile, 2003). Conversely, topical and (Cook, 1968; Caron et al., 1987). systemic medical treatment are not considered to Fungal plaques, usually located on the roof of be efficacious (Aisworth and Hackett, 2004). the medial compartment and less frequently on the To the Authors’ knowledge a detailed description dorsolateral wall of the lateral compartment, repre- of clinical features, treatment and follow up of gut- sent the main features of the disease; plaques have tural pouch mycosis in a donkey is not available in a strong association with underlying structures, the scientific literature. -

Guttural Pouch Hemorrhage Associated with Lesions of the Maxillary Artery in Two Horses
CASE REPORT Guttural Pouch Hemorrhage Associated with Lesions of the Maxillary Artery in Two Horses K.M. SMITH AND S.M. BARBER Wetaskiwin Veterinary Hospital, 4808-40th Avenue, Wetaskiwin, Alberta 79A OA2 (Smith) and Department ofAnesthesia, Radiology and Surgery, Western College of Veterinary Medicine, University of Saskatchewan, Saskatoon, Saskatchewan 57N 0 WO (Barber) Summary roughbred hongre et age de deux ans, poches gutturales, occlusion arterielle, A two year old Thoroughbred geld- dont la poche gutturale gauche sai- catheter pneumatique, cheval. ing, presented with guttural pouch gnait abondamment, avait subi la liga- hemorrhage, had the internal and ture des carotides interne et externe external carotid arteries ligated. Gut- correspondantes. Un examen endo- Introduction tural pouch mycosis was detected on scopique de cette poche gutturale Ulceration of vessels on the wall of endoscopic examination. After one permit d'y deceler une infection myco- the guttural pouch commonly occurs month of topical antifungal therapy, sique. En depit d'un traitement anti- with guttural pouch mycosis, and is the horse was returned and euthanized mycosique topique d'une duree d'un characterized by acute, often fatal, because of recurrent epistaxis. A bac- mois, il fallut hospitaliser de nouveau epistaxis (1-6). Approximately 50% of terial infection of the guttural pouch le cheval, a cause d'une epistaxis recur- affected horses die offatal hemorrhage with associated ulceration and hemor- rente, et son proprietaire en demanda (7). Usually several bouts of epistaxis rhage from the maxillary artery was l'enthanasie. La necropsie de l'animal occur before a fatal episode, but there found at necropsy. permit de decouvrir une infection bac- is no predictable pattern (1). -

Arterial Variations of the Subclavian-Axillary Arterial Tree: Its Association with the Supply of the Rotator Cuff Muscles
Int. J. Morphol., 32(4):1436-1443, 2014. Arterial Variations of the Subclavian-Axillary Arterial Tree: Its Association with the Supply of the Rotator Cuff Muscles Variaciones Arteriales del Árbol Arterial Subclavio-Axilar. Su Asociación con la Irrigación del Manguito de los Rotadores N. Naidoo*; L. Lazarus*; B. Z. De Gama*; N. O. Ajayi* & K. S. Satyapal* NAIDOO, N.; LAZARUS, L.; DE GAMA, B. Z.; AJAYI, N. O. & SATYAPAL, K. S. Arterial variations of the subclavian-axillary arterial tree: Its association with the supply of the rotator cuff muscles. Int. J. Morphol., 32(4):1436-1443, 2014. SUMMARY: The subclavian-axillary arterial tree is responsible for the arterial supply to the rotator cuff muscles as well as other shoulder muscles. This study comprised the bilateral dissection of the shoulder and upper arm region in thirty-one adult and nineteen fetal cadaveric specimens. The variable origins and branching patterns of the axillary, subscapular, circumflex scapular, thoracodorsal, posterior circumflex humeral and suprascapular arteries identified in this study corroborated the findings of previous studies. In addition, unique variations that are unreported in the literature were also observed. The precise anatomy of the arterial distribution to the rotator cuff muscles is important to the surgeon and radiologist. It will aid proper interpretation of radiographic images and avoid injury to this area during surgical procedures. KEY WORDS: Subclavian-axillary arterial tree; Variations; Supply; Rotator cuff muscles. INTRODUCTION Standard anatomical textbooks divide the axillary identified by Saralaya et al. (2008) to arise as a large artery into three parts using its relation to the pectoralis minor collateral branch from the first part of the axillary artery muscle (Salopek et al., 2007). -

Journal of Neurology Research Review & Reports
Journal of Neurology Research Review & Reports Case Report Open Access Bilateral Tortuous Upper Limb Arterial Tree and Their Clinical Significance Alka Bhingardeo Department of Anatomy, All India Institute of Medical Sciences, Bibinagar ABSTRACT The detailed knowledge about the possible anatomical variations of upper limb arteries is vital for the reparative surgery of the region. Brachial artery is the main artery of upper limb; it is a continuation of axillary artery from the lower border of teres major muscle. During routine cadaveric dissection, we found bilateral tortuous brachial artery which was superficial as well as tortuous throughout its course. It is called superficial as it was superficial to the median nerve. At the neck of radius, it was divided into two terminal branches radial and ulnar arteries which were also tortuous. Tortuosity of the radial artery was more near the flexor retinaculum. When observed, the continuation of ulnar artery as superficial palmar arch also showed tortuosity throughout, including its branches. Being superficial such brachial artery can be more prone to trauma. Tortuous radial artery is one of the causes of access failure in trans-radial approach of coronary interventions. To the best of our knowledge, this is the first case where entire post axillary upper limb arterial system is tortuous bilaterally. So knowledge of such tortuous upper limb arterial tree is important for cardiologist, radiologist, plastic surgeons and orthopedic surgeons. *Corresponding author Alka Bhingardeo, Assistant Professor, Department of Anatomy, All India Institute of Medical Sciences, Bibinagar, Telangana, India, Mob: 8080096151, Email: [email protected] Received: November 08, 2020; Accepted: November 16, 2020; Published: November 21, 2020 Keywords: Radial Artery, Superficial Brachial Artery, Tortuous, Brachial Artery Ulnar Artery, Upper Limb The brachial artery commenced from the axillary artery at the lower border of teres major muscle. -

Critical Surgical Affections at Pharyngeal Region in Horses 1Mosbah E., 2Rizk A., 3Karrouf G
RE SEARCH ARTICLE Mosbah et al. , IJAVMS, Vol. 6, Issue 6, 2012: 418-423 DOI: 10.5455/ijavms.20130111041833 Critical Surgical Affections at Pharyngeal Region in Horses 1Mosbah E., 2Rizk A., 3Karrouf G. 4Hahn J., 5Abou Alsoud M. and 6Zaghloul A. 1,2,6 Department of Surgery, Anaesthesiology and Radiology, Faculty of Veterinary Medicine, Mansoura University, Mansoura, Egypt; 3King Fahd Medical Research Center, King Abdulaziz University, Jeddah, Saudi Arabia; 4Clinic for Horses, University of Veterinary Medicine, Hannover, Germany; 5Biology Science Department, King Abdulaziz University, Jeddah, Saudi Arabia. Corresponding author email: [email protected] Abstract The present study was performed for diagnosis and surgical management of critical surgical affections at the pharyngeal region in horses. It was carried out on a total number of 10 horses. Radiographical and histopathological examinations were performed to confirm the diagnosis in addition to endoscopic examination for subepiglottic cyst. Surgical and endoscopic interventions were performed. A subepiglottic cyst was diagnosed in a mare as a voluminous mass rostral to the epiglottis through endoscopic examination. A thyroglossal duct cyst was found in a filly foal as a large banana like, cystic fluctuant mass at the left retropharyngeal region. A melanotic melanoma was detected in a mare as a distinct midline cranial ventral cervical mass. Guttural pouch empyema was recorded in 7 horses. It could be concluded that surgical and endoscopic treatments were curative for management of such affections without recurrence. Also, thyroglossal duct cyst should be included as a differential diagnosis when encountering a foal with a fluid filled mass at the lateral retropharyngeal region. Key words: Subepiglottic cyst, thyroglossal duct cyst, melanoma, guttural pouch empyema, horses. -

Collateral Circulation in Spinal Cord Injury: a Comprehensive Review
Published online: 2020-09-29 THIEME Review Article 1 Collateral Circulation in Spinal Cord Injury: A Comprehensive Review Ezequiel Garcia-Ballestas1 B. V. Murlimanju2 Yeider A. Durango-Espinosa1 Andrei F. Joaquim3 Harold E. Vasquez4 Luis Rafael Moscote-Salazar5 Amit Agrawal6 1Faculty of Medicine, Center for Biomedical Research (CIB), Address for correspondence Luis Rafael Moscote-Salazar, MD, University of Cartagena, Cartagena, Colombia Neurosurgeon-Critical Care, Center for Biomedical Research (CIB), 2Department of Anatomy, Kasturba Medical College, Mangalore, Cartagena Neurotrauma Research Group, Faculty of Medicine, Manipal Academy of Higher Education, Manipal, Karnataka, India University of Cartagena, Calle de la Universidad, Cra. 6 #36-100, 3Neurosurgery Division, Cartagena de Indias, Bolivar Department of Cartagena, Bolívar 130001, Columbia Neurology, State University of Campinas, Campinas-Sao Paulo, Brazil (e-mail: [email protected]). 4Universidad del Sinu, Cartagena de Indias, Consejo Latinoamericano de Neurointensivismo (CLaNi), Cartagena de Indias, Colombia 5Neurosurgeon-Critical Care, Center for Biomedical Research (CIB), Cartagena Neurotrauma Research Group, Faculty of Medicine, University of Cartagena, Cartagena, Colombia 6Department of Neurosurgery, All India Institute of Medical Sciences, Bhopal, Madhya Pradesh, India Indian J Neurotrauma:2021;18:1–6 Abstract Surgery is the most common cause of spinal cord ischemia; it is also caused by hemo- dynamic changes, which disrupt the blood flow. Direct ligation of the spinal arteries, especially the Adamkiewicz artery is involved as well. Other causes of spinal cord isch- emia include arteriography procedures, thoracic surgery, epidural and rachianesthesia, foraminal infiltration, arterial dissection, systemic hypotension, emboligenic heart dis- ease, thoracic disc herniation, and compression. Understanding the vascular anatomy of the spinal cord is essential to develop optimal strategies for preventing ischemic injuries to the spinal cord. -

The Suboccipital Cavernous Sinus
The suboccipital cavernous sinus Kenan I. Arnautovic, M.D., Ossama Al-Mefty, M.D., T. Glenn Pait, M.D., Ali F. Krisht, M.D., and Muhammad M. Husain, M.D. Departments of Neurosurgery and Pathology, University of Arkansas for Medical Sciences, and Laboratory Service, Veterans Administration Medical Center, Little Rock, Arkansas The authors studied the microsurgical anatomy of the suboccipital region, concentrating on the third segment (V3) of the vertebral artery (VA), which extends from the transverse foramen of the axis to the dural penetration of the VA, paying particular attention to its loops, branches, supporting fibrous rings, adjacent nerves, and surrounding venous structures. Ten cadaver heads (20 sides) were fixed in formalin, their blood vessels were perfused with colored silicone rubber, and they were dissected under magnification. The authors subdivided the V3 into two parts, the horizontal (V3h) and the vertical (V3v), and studied the anatomical structures topographically, from the superficial to the deep tissues. In two additional specimens, serial histological sections were acquired through the V3 and its encircling elements to elucidate their cross-sectional anatomy. Measurements of surgically and clinically important features were obtained with the aid of an operating microscope. This study reveals an astonishing anatomical resemblance between the suboccipital complex and the cavernous sinus, as follows: venous cushioning; anatomical properties of the V3 and those of the petrouscavernous internal carotid artery (ICA), namely their loops, branches, supporting fibrous rings, and periarterial autonomic neural plexus; adjacent nerves; and skull base locations. Likewise, a review of the literature showed a related embryological development and functional and pathological features, as well as similar transitional patterns in the arterial walls of the V3 and the petrous-cavernous ICA. -

Modelling and Simulation of the Human Arterial Tree - a Combined Lumped-Parameter and Transmission Line Element Approach M
Transactions on Biomedicine and Health vol 2, © 1995 WIT Press, www.witpress.com, ISSN 1743-3525 Modelling and simulation of the human arterial tree - a combined lumped-parameter and transmission line element approach M. Karlsson Applied Thermodynamics and Fluid Mechanics Department of Mechanical Engineering, Linkoping University, Linkoping, Sweden 1 Introduction Computer models of the arterial tree has been a goal in bio-fluid dynamics ever since the advent of the digital computer. Over the years several con- tributions have been made and increasingly more elaborate models of the systemic arterial tree have been developed in order to gain a better insight into the hemodynamics of man. This paper describes a model of the arterial tree with distributed pa- rameters which has been developed in order to quantify hydro-mechanical effects in the arterial system. Any such model must resolve the characteris- tic features of the arterial tree such as distributed resistance and the ability to incorporate local variations in segrnental compliance. The topology of the arterial tree must also be included in order to resolve wave reflections adequately. As the model is intended for non-stationary analysis special attention must be paid to the proximal boundary condition, the heart. Fur- thermore, an effective and robust numerical method is necessary in order to keep the computational time as low as possible. 2 Modelling the cardiovascular system A model of the arterial system consisting of 128 segments, each described by a four-pole equation, has been derived. The geometrical and topological de- scription is based on the geometry presented by Avolio [1]. -
Three-Dimensional Reconstructed Contrast–Enhanced MR Angiography for Internal Iliac Artery Branch Visualization Before Uterine Artery Embolization
Three-dimensional Reconstructed Contrast–enhanced MR Angiography for Internal Iliac Artery Branch Visualization before Uterine Artery Embolization Nagy N.N. Naguib, MSc,* Nour-Eldin A. Nour-Eldin, MSc,* Renate M. Hammerstingl, MD, Thomas Lehnert, MD, Julius Floeter, MD, Stefan Zangos, MD, and Thomas J. Vogl, MD PURPOSE: To evaluate the feasibility of three-dimensional (3D) reconstructed contrast-enhanced (CE) magnetic resonance (MR) angiography in mapping the pelvic arteries in women before uterine artery embolization (UAE). MATERIALS AND METHODS: CE MR angiography studies before UAE in 49 women (age range, 38–57 years; mean, y ؎ 4.7 [SD]) who underwent UAE for uterine leiomyomas between February 2005 and February 2007 were 47.04 retrospectively evaluated by two radiologists in consensus. Studies were performed on a 1.5-T MR unit with a 3D fast low-angle shot sequence in the coronal direction. Reconstruction was performed with 3D computed tomographic angiography reconstruction software. RESULTS: In the current study, 98 internal iliac arteries (IIAs) from 49 women were studied. The superior and inferior the lateral sacral artery in 86 cases (88%), the iliolumbar ,(%100 ;98 ؍ gluteal arteries were visualized in all cases (N artery in 84 (86%), the obturator artery in 81 (83%), the internal pudendal artery in 96 (98%), and the uterine artery in 95 (97%). The superior vesical and middle rectal arteries were seen in 21 (21%) and 11 (11%) cases, respectively. The mean length of the uterine artery was 12.56 cm (range, 4.6–22.2 cm), and it showed the longest traceable length among all branches. The uterine artery showed five patterns of origin. -

Modelling Physiology of Haemodynamic Adaptation in Short
www.nature.com/scientificreports OPEN Modelling physiology of haemodynamic adaptation in short‑term microgravity exposure and orthostatic stress on Earth Parvin Mohammadyari1, Giacomo Gadda2* & Angelo Taibi1 Cardiovascular haemodynamics alters during posture changes and exposure to microgravity. Vascular auto‑remodelling observed in subjects living in space environment causes them orthostatic intolerance when they return on Earth. In this study we modelled the human haemodynamics with focus on head and neck exposed to diferent hydrostatic pressures in supine, upright (head‑up tilt), head‑down tilt position, and microgravity environment by using a well‑developed 1D‑0D haemodynamic model. The model consists of two parts that simulates the arterial (1D) and brain‑ venous (0D) vascular tree. The cardiovascular system is built as a network of hydraulic resistances and capacitances to properly model physiological parameters like total peripheral resistance, and to calculate vascular pressure and the related fow rate at any branch of the tree. The model calculated 30.0 mmHg (30%), 7.1 mmHg (78%), 1.7 mmHg (38%) reduction in mean blood pressure, intracranial pressure and central venous pressure after posture change from supine to upright, respectively. The modelled brain drainage outfow percentage from internal jugular veins is 67% and 26% for supine and upright posture, while for head‑down tilt and microgravity is 65% and 72%, respectively. The model confrmed the role of peripheral veins in regional blood redistribution during posture change from supine to upright and microgravity environment as hypothesized in literature. The model is able to reproduce the known haemodynamic efects of hydraulic pressure change and weightlessness. It also provides a virtual laboratory to examine the consequence of a wide range of orthostatic stresses on human haemodynamics.