The WHO Application of ICD-10 to Deaths During the Perinatal Period: ICD-PM WHO Library Cataloguing-In-Publication Data
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Meconium Peritonitis
ISSN: 2377-9004 Agrawal et al. Obstet Gynecol Cases Rev 2020, 7:180 DOI: 10.23937/2377-9004/1410180 Volume 6 | Issue 5 Obstetrics and Open Access Gynaecology Cases - Reviews CASE REPORT Meconium Peritonitis: In Utero Diagnosis of a Rare Clinical Entity and Postnatal Outcome Sarita Agrawal, MD, FICOG, FIAMS, FCGP1, Arpana Verma, MS2*, Sarita Rajbhar, MS3, Pushpawati Thakur, MD4, Loukya Kodumuri, MBBS5 and Swati Kumari, MS, FNB6 1Professor and Head of Department, Department of Obstetrics and Gynaecology, All India Institute of Medical Sciences, Raipur, Chhattisgarh, India 2Senior Resident, Department of Obstetrics and Gynaecology, All India Institute of Medical Sciences, Raipur, Chhattisgarh, India 3Assistant Professor, Department of Obstetrics and Gynaecology, All India Institute of Medical Sciences, Raipur, Chhattisgarh, India 4 Check for Associate Professor, Department of Obstetrics and Gynaecology, All India Institute of Medical Sciences, updates Raipur, Chhattisgarh, India 5Post Graduate Student, Department of Obstetrics and Gynaecology, All India Institute of Medical Sciences, Raipur, Chhattisgarh, India 6Sonologist and Fetal Medicine Expert, Shivam Fetomed and Spine Centre, Raipur, Chhattisgarh, India *Corresponding author: Arpana Verma, MS, Senior Resident, Department of Obstetrics and Gynaecology, All India Institute of Medical Sciences, V.V-18, Parthivi Province, Near Salasar Greens, Sarona, Raipur, Chhattisgarh - 492099, India, Tel: 9741412716; 6260334337 Abstract done for immune and non-immune hydrops and was found to be negative. One week later, a repeat ultrasound was done Objective: To present an unusual case of meconium peri- which showed moderate fetal ascites with few areas of calci- tonitis diagnosed during prenatal period and its postnatal fication in the bowel loops and prominent inferior vena cava, outcome. -

Lung Pathology: Embryologic Abnormalities
Chapter2C Lung Pathology: Embryologic Abnormalities Content and Objectives Pulmonary Sequestration 2C-3 Chest X-ray Findings in Arteriovenous Malformation of the Great Vein of Galen 2C-7 Situs Inversus Totalis 2C-10 Congenital Cystic Adenomatoid Malformation of the Lung 2C-14 VATER Association 2C-20 Extralobar Sequestration with Congenital Diaphragmatic Hernia: A Complicated Case Study 2C-24 Congenital Chylothorax: A Case Study 2C-37 Continuing Nursing Education Test CNE-1 Objectives: 1. Explain how the diagnosis of pulmonary sequestration is made. 2. Discuss the types of imaging studies used to diagnose AVM of the great vein of Galen. 3. Describe how imaging studies are used to treat AVM. 4. Explain how situs inversus totalis is diagnosed. 5. Discuss the differential diagnosis of congenital cystic adenomatoid malformation. (continued) Neonatal Radiology Basics Lung Pathology: Embryologic Abnormalities 2C-1 6. Describe the diagnosis work-up for VATER association. 7. Explain the three classifications of pulmonary sequestration. 8. Discuss the diagnostic procedures for congenital chylothorax. 2C-2 Lung Pathology: Embryologic Abnormalities Neonatal Radiology Basics Chapter2C Lung Pathology: Embryologic Abnormalities EDITOR Carol Trotter, PhD, RN, NNP-BC Pulmonary Sequestration pulmonary sequestrations is cited as the 1902 theory of Eppinger and Schauenstein.4 The two postulated an accessory he clinician frequently cares for infants who present foregut tracheobronchia budding distal to the normal buds, Twith respiratory distress and/or abnormal chest x-ray with caudal migration giving rise to the sequestered tissue. The findings of undetermined etiology. One of the essential com- type of sequestration, intralobar or extralobar, would depend ponents in the process of patient evaluation is consideration on the timing of the accessory foregut budding (Figure 2C-1). -

Hypocalcemia Associated with Subcutaneous Fat Necrosis of the Newborn: Case Report and Literature Review Alphonsus N
case report Oman Medical Journal [2017], Vol. 32, No. 6: Hypocalcemia Associated with Subcutaneous Fat Necrosis of the Newborn: Case Report and Literature Review Alphonsus N. Onyiriuka 1* and Theodora E. Utomi2 1Endocrine and Metabolic Unit, Department of Child Health, University of Benin Teaching Hospital, Benin City, Nigeria 2Special Care Baby Unit, Department of Nursing Services, St Philomena Catholic Hospital, Benin City, Nigeria ARTICLE INFO ABSTRACT Article history: Subcutaneous fat necrosis of the newborn (SCFNN) is a rare benign inflammatory Received: 4 November 2015 disorder of the adipose tissue but may be complicated by hypercalcemia or less frequently, Accepted: 21 October 2016 hypocalcemia, resulting in morbidity and mortality. Here we report the case of a neonate Online: with subcutaneous fat necrosis who surprisingly developed hypocalcemia instead DOI 10.5001/omj.2017.99 of hypercalcemia. A full-term female neonate was delivered by emergency cesarean section for fetal distress and was subsequently admitted to the Special Care Baby Keywords: Hypocalcemia; Infant, Unit. The mother’s pregnancy was uncomplicated up to delivery. Her anthropometric Newborn; Subcutaneous Fat measurements were birth weight 4.1 kg (95th percentile), length 50 cm (50th percentile), Necrosis; Perinatal Stress. and head circumference 34.5 cm (50th percentile). The Apgar scores were 2, 3, and 8 at 1, 5, 10 minutes, respectively. There was no abnormal facies and she was fed with breast milk only. On the seventh day of life, the infant was found to have multiple nodules located in the neck, upper back, and right arm. The nodules were firm, well circumscribed with no evidence of tenderness. -

Maternal and Foetal Mortality in Placenta Praevia"
J Obs Gyn Brit Emp 1962 V-69 MATERNAL AND FOETAL MORTALITY IN PLACENTA PRAEVIA" BY C. H. G. MACAFEE,C.B.E., D.Sc., F.R.C.S., F.R.C.O.G. Professor of Obstetrics and Gynaecology, The Queen's Universiiy of Belfast W. GORDONMILLAR, F.R.F.P.S., F.R.C.S., M.R.C.O.G. Consultant Obstetrician and Gynaecologist, Royal Injirmary, Perth; formerly Lecturer in Department qf Obstetrics and Gynaecology, The Queen's University of Belfast AND GRAHAMHARLEY, M.D., M.R.C.O.G. Lecturer, Department of Obstetrics and Gynaecology, The Queen's University of Belfast IN the 95 years between 1844-1939 the foetal During the first eight-year period 206 patients mortality from placenta praevia remained at were dealt with and in the second period the between 54 per cent and 60 per cent, while the number was 219. These two figures correspond maternal mortality fell from 30 per cent to 5 so closely that they permit a good statistical per cent. comparison to be made between the two eight- year periods. TABLE I Maternal Foetal Expectant Treatment Author Date Mortality Mortality In recent years the value of this treatment has been recognized and is becoming more 01,'O % SimDson . .. 1844 30 60 widely accepted even though it entails the Berkeley . 1936 7 59 occupation of antenatal beds sometimes for Browne . 1939 5 54 weeks. It is obvious that the nearer the preg- Belfast series . 1945-52 nil 14.9 nancy can be carried to full term the more 1953-60 0.9 11.1 favourable the outlook for the baby. -

Hypotonia and Lethargy in a Two-Day-Old Male Infant Adrienne H
Hypotonia and Lethargy in a Two-Day-Old Male Infant Adrienne H. Long, MD, PhD,a,b Jennifer G. Fiore, MD,a,b Riaz Gillani, MD,a,b Laurie M. Douglass, MD,c Alan M. Fujii, MD,d Jodi D. Hoffman, MDe A 2-day old term male infant was found to be hypotonic and minimally abstract reactive during routine nursing care in the newborn nursery. At 40 hours of life, he was hypoglycemic and had intermittent desaturations to 70%. His mother had an unremarkable pregnancy and spontaneous vaginal delivery. The mother’s prenatal serology results were negative for infectious risk factors. Apgar scores were 9 at 1 and 5 minutes of life. On day 1 of life, he fed, stooled, and voided well. Our expert panel discusses the differential diagnosis of hypotonia in a neonate, offers diagnostic and management recommendations, and discusses the final diagnosis. DRS LONG, FIORE, AND GILLANI, birth weight was 3.4 kg (56th PEDIATRIC RESIDENTS percentile), length was 52 cm (87th aDepartment of Medicine, Boston Children’s Hospital, d e percentile), and head circumference Boston, Massachusetts; and Neonatology Section, Medical A 2-day old male infant born at Genetics Section, cDivision of Child Neurology, and 38 weeks and 4 days was found to be was 33 cm (12th percentile). His bDepartment of Pediatrics, Boston Medical Center, Boston, limp and minimally reactive during physical examination at birth was Massachusetts routine care in the newborn nursery. normal for gestational age, with Drs Long, Fiore, and Gillani conceptualized, drafted, Just 5 hours before, he had an appropriate neurologic, cardiac, and and edited the manuscript; Drs Douglass, Fujii, and appropriate neurologic status when respiratory components. -

N35.12 Postinfective Urethral Stricture, NEC, Female N35.811 Other
N35.12 Postinfective urethral stricture, NEC, female N35.811 Other urethral stricture, male, meatal N35.812 Other urethral bulbous stricture, male N35.813 Other membranous urethral stricture, male N35.814 Other anterior urethral stricture, male, anterior N35.816 Other urethral stricture, male, overlapping sites N35.819 Other urethral stricture, male, unspecified site N35.82 Other urethral stricture, female N35.911 Unspecified urethral stricture, male, meatal N35.912 Unspecified bulbous urethral stricture, male N35.913 Unspecified membranous urethral stricture, male N35.914 Unspecified anterior urethral stricture, male N35.916 Unspecified urethral stricture, male, overlapping sites N35.919 Unspecified urethral stricture, male, unspecified site N35.92 Unspecified urethral stricture, female N36.0 Urethral fistula N36.1 Urethral diverticulum N36.2 Urethral caruncle N36.41 Hypermobility of urethra N36.42 Intrinsic sphincter deficiency (ISD) N36.43 Combined hypermobility of urethra and intrns sphincter defic N36.44 Muscular disorders of urethra N36.5 Urethral false passage N36.8 Other specified disorders of urethra N36.9 Urethral disorder, unspecified N37 Urethral disorders in diseases classified elsewhere N39.0 Urinary tract infection, site not specified N39.3 Stress incontinence (female) (male) N39.41 Urge incontinence N39.42 Incontinence without sensory awareness N39.43 Post-void dribbling N39.44 Nocturnal enuresis N39.45 Continuous leakage N39.46 Mixed incontinence N39.490 Overflow incontinence N39.491 Coital incontinence N39.492 Postural -

Caesarean Section for Placenta Praevia (Consent Advice No
Royal College of Obstetricians and Gynaecologists Consent Advice No. 12 December 2010 CAESAREAN SECTION FOR PLACENTA PRAEVIA This is the first edition of this guidance. This paper provides additional advice for clinicians in obtaining consent of a woman to undergo caesarean section in the specific circumstance of current pregnancy with placenta praevia with or without previous caesarean section. It is designed to be used in conjunction with Consent Advice No. 7: Caesarean section.1 The aim of this paper is to highlight the additional and specific consequences of caesarean section performed in the presence of placenta praevia. The information should, where possible, be provided during the antenatal period in the form of an information sheet to allow the woman to understand the situation and to provide ample opportunities for her to ask any questions she may have and to antenatally meet providers of additional services that may become necessary, such as interventional radiologists. Depending on local clinical governance arrangements, an additional consent form may be used with the addition- al risks highlighted, or the additional risks may be incorporated in a specific consent form for the whole procedure. CONSENT FORM 1. Name of proposed procedure or course of treatment Caesarean section for placenta praevia. 2. The proposed procedure Describe the nature of caesarean section and emphasise how a procedure in the presence of placenta praevia varies in comparison with one performed in the presence of a normally sited placenta. Explain the procedure as described in the patient information. 3. Intended benefits The aim of the procedure is to secure the safest route of delivery to avoid the anticipated risks to the mother and/or baby of the heavy bleeding that would occur during labour and attempted vaginal delivery owing to the position of the placenta. -

Hypotonia Surestep Product Catalog Page 29 in Step with Pediatric Hypotonia
SPECIAL EDUCATIONAL SERIES DIAGNOSTIC INSIGHTS ANALYZING GAIT CHANGES GROSS MOTOR SKILLS ORTHOTIC MANAGEMENT CLI N I CAL CASE STUDIES Sponsored by an educational grant from: In Step With Pediatric Hypotonia SureStep Product Catalog Page 29 In Step With Pediatric Hypotonia Contents VIEWPOINT FROM THE EDITOR: An Unexpected Path, Mobility and More an Invaluable Perspective At the most basic level, mobility is about get- PAGE 3 ting from point A to point B. But, for many children with hypotonia, it’s about so much 4 more. FEATURES It’s about independence. It’s about con- fidence. It’s about maintaining strength, fit- ness, and healthy bones. It’s about not being Understanding Hypotonia excluded from activities enjoyed by their PAGE 4 typically developing peers. And improved mobility may have even Gait: The Cornerstone more benefits in those children whose hy- potonia is associated with social and behav- of Intervention ioral developmental delays. New research PAGE 8 has identified an association between motor skills and sociobehavioral milestones in chil- 8 The Importance of Gross dren with autism spectrum disorder, who often present with hypotonia (see “The Im- Motor Skills portance of Gross Motor Skills,” page 12). PAGE 12 This suggests that early intervention to improve gross motor skills—including or- thotic devices and physical therapy—may Orthotic Solutions for also help certain children interact more Children with Hypotonia comfortably with others. That won’t come as PAGE 16 a surprise to the clinicians and parents who 12 have personally seen it happen. This special issue is filled with evidence- Orthotic Success Stories: based information and personal success sto- Four Cases in a Series ries illustrating how effective interventions can enhance mobility in children with hy- PAGE 20 potonia. -

Prenatal Diagnosis of Frequently Seen Fetal Syndromes (AZ)
Prenatal diagnosis of frequently seen fetal syndromes (A-Z) Ibrahim Bildirici,MD Professor of OBGYN ACIBADEM University SOM Attending Perinatologist ACIBADEM MASLAK Hospital Amniotic band sequence: Amniotic band sequence refers to a highly variable spectrum of congenital anomalies that occur in association with amniotic bands The estimated incidence of ABS ranges from 1:1200 to 1:15,000 in live births, and 1:70 in stillbirths Anomalies include: Craniofacial abnormalities — eg, encephalocele, exencephaly, clefts, which are often in unusual locations; anencephaly. Body wall defects (especially if not in the midline), abdominal or thoracic contents may herniate through a body wall defect and into the amniotic cavity. Limb defects — constriction rings, amputation, syndactyly, clubfoot, hand deformities, lymphedema distal to a constriction ring. Visceral defects — eg, lung hypoplasia. Other — Autotransplanted tissue on skin tags, spinal defects, scoliosis, ambiguous genitalia, short umbilical cord due to restricted motion of the fetus Arthrogryposis •Multiple congenital joint contractures/ankyloses involving two or more body areas •Pena Shokeir phenotype micrognathia, multiple contractures, camptodactyly (persistent finger flexion), polyhydramnios *many are AR *Lethal due to pulmonary hypoplasia • Distal arthrogryposis Subset of non-progressive contractures w/o associated primary neurologic or muscle disease Beckwith Wiedemannn Syndrome Macrosomia Hemihyperplasia Macroglossia Ventral wall defects Predisposition to embryonal tumors Neonatal hypoglycemia Variable developmental delay 85% sporadic with normal karyotype 10-15% autosomal dominant inheritance 10-20% with paternal uniparental disomy (Both copies of 11p15 derived from father) ***Imprinting related disorder 1/13 000. Binder Phenotype a flat profile and depressed nasal bridge. Short nose, short columella, flat naso-labial angle and perialar flattening Isolated Binder Phenotype transmission would be autosomal dominant Binder Phenotype can also be an important sign of chondrodysplasia punctata (CDDP) 1. -

Nonimmune Hydrops Foetalis: Value of Perinatal Autopsy and Placental Examination in Determining Aetiology
International Journal of Research in Medical Sciences Ramya T et al. Int J Res Med Sci. 2018 Oct;6(10):3327-3334 www.msjonline.org pISSN 2320-6071 | eISSN 2320-6012 DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20184041 Original Research Article Nonimmune hydrops foetalis: value of perinatal autopsy and placental examination in determining aetiology Ramya T.1, Umamaheswari G2*, Chaitra V.2 1Department of Obstetrics and Gynaecology, 2Department of Pathology, PSG Institute of Medical Sciences and Research, Coimbatore, Tamil Nadu, India Received: 29 July 2018 Accepted: 29 August 2018 *Correspondence: Dr. Umamaheswari G., E-mail: [email protected] Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Background: Authors sought to determine the possible factors in the causation of nonimmune hydrops foetalis by perinatal autopsy with placental examination and to reduce the number of cases in which the cause remains elusive. Methods: Twenty five cases of nonimmune hydrops foetalis were identified in about 200 consecutive perinatal autopsies (including placental examination) performed during a 11 year period. The results were correlated with clinical, laboratory and imaging characteristics in an attempt to establish the aetiology. Results: Perinatal autopsy and placental examination confirmed the following aetiologies: cardiovascular causes (8) [isolated (4), syndromic (3) and associated chromosomal (1)], placental causes (5), chromosomal (4) [isolated(3) and associated cardiovascular disease (1)], intrathoracic (3), genitourinary causes (3), infections(1),gastrointestinal lesions (1) and idiopathic causes (1). -

CASE REPORT CASE CASE R Imaging Findings of Meconium
CASE REPORT CASE REPORT Imaging findings of meconium peritonitis Logeshini Naidoo, MB ChB, FCRad (Diag) SA Helen Joseph and Coronation Hospitals, Johannesburg Introduction Meconium peritonitis results from intrauterine gastrointestinal perfora- tion, and can occur as early as the second trimester.1 Meconium extrudes into the peritoneal cavity, inciting an intense fibroplastic reaction that results in intra-abdominal calcifications.2 It is a rare condition occurring in 1 in 35 000 pregnant women.3 The clinical and radiological manifestations depend on whether the bowel perforation seals off in utero in the neonatal period or remains patent.3 Accordingly, the radiological spectra range from the incidental demonstration of diffuse intra-abdominal calcifications to meconium ascites (free meconium in the peritoneal cavity), meconium pseudocysts (walled-off meconium concentrations), and meconium hydrocoeles. Meconium has also been reported in the thoracic cavity (via diaphrag- matic hernias) and in the pelvic soft tissues.4 Antenatal ultrasound allows early detection of the condition, demonstrating free fluid, hydrocoeles and echogenic foci representing intraperitoneal calcifications.5 In the newborn, plain abdominal radiographs demonstrating calcifications and/or ascites are sufficient for diagnosis.1 Postnatal ultrasound is reserved for atypical presentations and can exclude intra-abdominal masses.1 Although computed tomography (CT) was used as an ancillary tool in the case report described below, it is unnecessary, thus negating the need for radiation exposure and expenditure of time. Fig. 1. Supine abdominal X-ray revealing a massively distended abdomen with poor lung capacities. The bulging flanks and central The imaging findings in a newborn with an ongoing bowel perfora- floating bowel loops indicate ascites. -
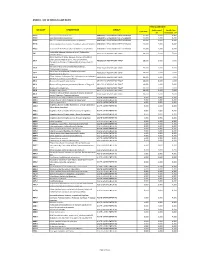
Annex 1: List of Medical Case Rates
ANNEX 1. LIST OF MEDICAL CASE RATES FIRST CASE RATE ICD CODE DESCRIPTION GROUP Professional Health Care Case Rate Fee Institution Fee P91.3 Neonatal cerebral irritability ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 P91.4 Neonatal cerebral depression ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 P91.6 Hypoxic ischemic encephalopathy of newborn ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 P91.8 Other specified disturbances of cerebral status of newborn ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 P91.9 Disturbance of cerebral status of newborn, unspecified ABNORMAL SENSORIUM IN THE NEWBORN 12,000 3,600 8,400 Peritonsillar abscess; Abscess of tonsil; Peritonsillar J36 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 cellulitis; Quinsy Other diseases of larynx; Abscess of larynx; Cellulitis of larynx; Disease NOS of larynx; Necrosis of larynx; J38.7 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 Pachyderma of larynx; Perichondritis of larynx; Ulcer of larynx Retropharyngeal and parapharyngeal abscess; J39.0 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 Peripharyngeal abscess Other abscess of pharynx; Cellulitis of pharynx; J39.1 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 Nasopharyngeal abscess Other diseases of pharynx; Cyst of pharynx or nasopharynx; J39.2 ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 Oedema of pharynx or nasopharynx J85.1 Abscess of lung with pneumonia ABSCESS OF RESPIRATORY TRACT 10,000 3,000 7,000 J85.2 Abscess of lung without pneumonia; Abscess of lung NOS ABSCESS OF RESPIRATORY