WADA 2018 Prohibited List
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
WADA Technical Letter – TL07 ANDARINE
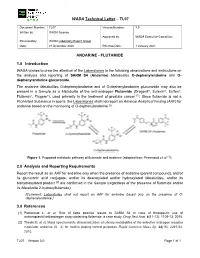
WADA Technical Letter – TL07 Document Number: TL07 Version Number: 3.0 Written by: WADA Science Approved by: WADA Executive Committee Reviewed by: WADA Laboratory Expert Group Date: 21 December 2020 Effective Date: 1 January 2021 ANDARINE - FLUTAMIDE 1.0 Introduction WADA wishes to draw the attention of the Laboratories to the following observations and instructions on the analysis and reporting of SARM S4 (Andarine) Metabolites O-dephenylandarine and O- dephenylandarine glucuronide. The andarine Metabolites O-dephenylandarine and of O-dephenylandarine glucuronide may also be present in a Sample as a Metabolite of the anti-androgen Flutamide (Drogenil®, Eulexin®, Euflex®, Flutamin®, Flugere®), used primarily in the treatment of prostate cancer [1]. Since flutamide is not a Prohibited Substance in sports, the Laboratories shall not report an Adverse Analytical Finding (AAF) for andarine based on the monitoring of O-dephenylandarine [2]. Figure 1. Proposed metabolic pathway of flutamide and andarine (adapted from Perrenoud et al. [1]). 2.0 Analysis and Reporting Requirements Report the result as an AAF for andarine only when the presence of andarine (parent compound), and/or its glucuronic acid conjugate, and/or its deacetylated and/or hydroxylated Metabolites, and/or its bishydroxylated product [2] are confirmed in the Sample (regardless of the presence of flutamide and/or its Metabolite 2-hydroxyflutamide); [Comment: Laboratories shall not report an AAF for andarine based only on the presence of O- dephenylandarine.] 3.0 References [1] Perrenoud L. et al. Risk of false positive results to SARM S4 in case of therapeutic use of antineoplastic/antiandrogen drug containing flutamide: a case study. -

Benfluorex: What Use? a SECOND LOOK POOR ASSESSMENT FILE
New products necessitating blood transfusions 3- “Paclitaxel” Prescr Intern 1994; 3 (14): 164-165. Literature 4- Rowisky EK et al. “Phase I and pharmacolog- occurred in 37% of patients (9). ic study of topotecan: a novel topoisomerase I The most frequent non haematologi- Our literature search was based on systematic inhibitor” J Clin Oncol 1992; 10: 647-656. cal side effects were nausea (68.1% of scrutiny of contents listings of the main inter- 5- Verweij L et al. “Phase I and pharmacokinet- ics study of topotecan, a new topoisomerase I patients, severe in 6.1% of patients), national journals and Current Contents at inhibitor” Ann Oncol 1993; 4: 673-678. vomiting (44.3%, severe in 4.5%), hair the Prescrire library, and on reference texts 6- Saltz L et al. “Phase I clinical and pharmacol- in clinical pharmacology (Martindale The ogy study of topotecan given daily for 5 consecu- loss (56.9%), fatigue (44.5%, severe in Extra Pharmacopoeia 31st ed., etc.). We also tive days to patients with advanced solid tumors, 6%), diarrhoea (26.1%, severe in 3.4%), consulted CD-ROM versions of Medline (1981- with attempt at dose intensification using recom- and stomatitis (20.2%, severe in 2%) (9). March 1998), Embase Drugs and binant granulocyte colony-stimulating factor” J Pharmacology (1991-January 1998), Cochrane Natl Cancer Inst 1993; 85 (18): 1499-1507. Paclitaxel solution contains a solvent, 7- Kudelka AP et al. “Phase II study of intravenous Cremophor EL°, that is incompatible with (1998, issue 1), Medidoc (1991-1994) and topotecan as a 5-day infusion for refractory epithe- Reactions (1983-June 1997), and the Minitel lial ovarian carcinoma” J Clin Oncol 1996; 14: the use of PVC infusion devices and war- version of the Pascal database up to 1552-1557. -

Compositions Comprising Drospirenone Molecularly
(19) & (11) EP 1 748 756 B1 (12) EUROPEAN PATENT SPECIFICATION (45) Date of publication and mention (51) Int Cl.: of the grant of the patent: A61K 9/00 (2006.01) A61K 9/107 (2006.01) 29.04.2009 Bulletin 2009/18 A61K 9/48 (2006.01) A61K 9/16 (2006.01) A61K 9/20 (2006.01) A61K 9/14 (2006.01) (2006.01) (2006.01) (21) Application number: 05708751.2 A61K 9/70 A61K 31/565 (22) Date of filing: 10.03.2005 (86) International application number: PCT/IB2005/000665 (87) International publication number: WO 2005/087194 (22.09.2005 Gazette 2005/38) (54) COMPOSITIONS COMPRISING DROSPIRENONE MOLECULARLY DISPERSED ZUSAMMENSETZUNGEN AUS DROSPIRENON IN MOLEKULARER DISPERSION DES COMPOSITIONS CONTENANT DROSPIRENONE A DISPERSION MOLECULAIRE (84) Designated Contracting States: (72) Inventors: AT BE BG CH CY CZ DE DK EE ES FI FR GB GR • FUNKE, Adrian HU IE IS IT LI LT LU MC NL PL PT RO SE SI SK TR D-14055 Berlin (DE) Designated Extension States: • WAGNER, Torsten AL BA HR MK YU 13127 Berlin (DE) (30) Priority: 10.03.2004 EP 04075713 (74) Representative: Wagner, Kim 10.03.2004 US 551355 P Plougmann & Vingtoft a/s Sundkrogsgade 9 (43) Date of publication of application: P.O. Box 831 07.02.2007 Bulletin 2007/06 2100 Copenhagen Ø (DK) (60) Divisional application: (56) References cited: 08011577.7 / 1 980 242 EP-A- 1 260 225 EP-A- 1 380 301 WO-A-01/52857 WO-A-20/04022065 (73) Proprietor: Bayer Schering Pharma WO-A-20/04041289 US-A- 5 569 652 Aktiengesellschaft US-A- 5 656 622 US-A- 5 789 442 13353 Berlin (DE) Note: Within nine months of the publication of the mention of the grant of the European patent in the European Patent Bulletin, any person may give notice to the European Patent Office of opposition to that patent, in accordance with the Implementing Regulations. -

AO-Klasifikácia Faktúr →Zlomeniny
AO-klasifikácia faktúr →zlomeniny. AOP-syndróm – skr. syndroma adipositas–oligomenorrhoea–parotis. aorta – [g. aorté srdcovnica] srdcovnica. Začína sa z ľavej komory a vystupuje kraniálne aţ do výšky 2. pravého sternokostálneho kĺbu ako aorta ascendens, pokračovaním je oblúk arcus aortae, aorta descendens, aorta thoracia a aorta abdominalis. Aorta ascendens – začína sa v ľavej komore nad polmesiačikovitými chlopňami a skoro celá sa nachádza v perikarde. Je dlhá asi 4 – 5 cm, jej priemer je 22 – 30 mm. Ihneď nad chlop-ňami je následkom spätných nárazov krvi mierne vydutá do tzv. sinus aortae, výraznejšie u starších osôb. Oddiely a. obsahujúce sinus aortae sa nazývajú bulbus aortae. U starších osôb býva následkom nárazov krvi širší aj koncový úsek vzostupnej a. pred jej prechodom do oblúka, tzv. sinus maximus (quartus) aortae. Tu býva u starších osôb a. často rozširená. A. ascendens, ako aj začiatok arcus aortae majú špeciálne vasa vasorum pochádzajúce z vencovitých tepien (aa. cardiaortales). Tento úsek osobitne patogeneticky rizikový. Začiatok aorta ascendens je ešte obalený vo vagina serosa arteriarum, kt. tvorí na ventrálnom obvode a. priečnu krkvu podloţenú subseróznym tukovým väzivom (Concatova-Bacceli tuková krkva). Vnútri vagina arteriarum je aorta ascendens a začiatrok a. pulmonalis spojené tuhým väzivom (vincula aortae Rindfleischi). Výstup aorta ascendens kryje spredu začiatok a. pulmonalis, ventrálne a vpravo je auricula dextra, dorzálne je uloţený r. dexter a. pulmonalis. Kraniálne vpravo od a. je v. cava superior, vľavo kmeň a. pulmonalis. Z ventrálneho a ľavého sinus aortae sa začína a. coronaria cordis dextra et sinistra. Aorta ascendens a arcus aortae Arcus aortae – je dlhý asi 6 cm, začína sa za sternom vo výške úponu 2. -

Download Product Insert (PDF)
Product Information Boldenone Cypionate Item No. 15158 CAS Registry No.: 106505-90-2 O Formal Name: 17β-hydroxy-androsta-1,4-dien-3-one O cyclopentanepropionate MF: C27H38O3 FW: 410.6 H Purity: ≥95% Stability: ≥2 years at -20°C H H Supplied as: A crystalline solid λ O UV/Vis.: max: 244 nm Laboratory Procedures For long term storage, we suggest that boldenone cypionate be stored as supplied at -20°C. It should be stable for at least two years. Boldenone cypionate is supplied as a crystalline solid. A stock solution may be made by dissolving the boldenone cypionate in the solvent of choice. Boldenone cypionate is soluble in organic solvents such as ethanol, DMSO, and dimethyl formamide, which should be purged with an inert gas. The solubility of boldenone cypionate in these solvents is approximately 15, 5, and 25 mg/ml, respectively. Boldenone cypionate is sparingly soluble in aqueous buffers. For maximum solubility in aqueous buffers, boldenone cypionate should first be dissolved in ethanol and then diluted with the aqueous buffer of choice. Boldenone cypionate has a solubility of approximately 0.3 mg/ml in a 1:2 solution of ethanol:PBS (pH 7.2) using this method. We do not recommend storing the aqueous solution for more than one day. Boldenone is an anabolic androgenic steroid and synthetic derivative of testosterone that was originally developed for veterinary use.1 It can increase nitrogen retention, protein synthesis, and appetite, and also stimulates the release of erythropoietin in the kidneys.1 Boldenone cypionate was synthesized as an ester of boldenone in an attempt to alter boldenone’s very long half-life.2 Anabolic androgenic steroid compounds such as boldenone cypionate have been used illicitly by bodybuilders and other athletes.3 This compound is intended for forensic and research purposes only. -

Prohibited Substances Shall Be Considered As “Specified Substances” Except Substances in Classes S1, S2, S.4.4, S.4.5, S6.A, and Prohibited Methods M1, M2 and M3
BGBl. III - Ausgegeben am 27. Dezember 2019 - Nr. 237 1 von 8 THE 2020 PROHIBITED LIST - WORLD ANTI-DOPING CODE DATE OF ENTRY INTO FORCE: 1 JANUARY 2020 SUBSTANCES AND METHODS PROHIBITED AT ALL TIMES (IN- AND OUT-OF-COMPETITION) IN ACCORDANCE WITH ARTICLE 4.2.2 OF THE WORLD ANTI-DOPING CODE, ALL PROHIBITED SUBSTANCES SHALL BE CONSIDERED AS “SPECIFIED SUBSTANCES” EXCEPT SUBSTANCES IN CLASSES S1, S2, S.4.4, S.4.5, S6.A, AND PROHIBITED METHODS M1, M2 AND M3. PROHIBITED SUBSTANCES Androstenediol (androst-5-ene-3β,17β-diol); Androstenedione (androst-4-ene-3,17-dione); S0. NON-APPROVED SUBSTANCES Bolasterone; Boldenone; Any pharmacological substance which is not Boldione (androsta-1,4-diene-3,17-dione); addressed by any of the subsequent sections of Calusterone; the List and with no current approval by any Clostebol; governmental regulatory health authority for Danazol ([1,2]oxazolo[4',5':2,3]pregna-4-en- human therapeutic use (e.g. drugs under pre- 20-yn-17α-ol); clinical or clinical development or discontinued, Dehydrochlormethyltestosterone (4-chloro- designer drugs, substances approved only for 17β-hydroxy-17α-methylandrosta-1,4-dien-3- veterinary use) is prohibited at all times. one); Desoxymethyltestosterone (17α-methyl-5α- S1. ANABOLIC AGENTS androst-2-en-17β-ol); Drostanolone; Anabolic agents are prohibited. Epiandrosterone (3β-hydroxy-5α-androstan- …………………………………………………… 17-one); 1. ANABOLIC ANDROGENIC STEROIDS Epi-dihydrotestosterone (17β-hydroxy-5β- (AAS) androstan-3one); Epitestosterone; when administered exogenously, including but -

UFC PROHIBITED LIST Effective June 1, 2021 the UFC PROHIBITED LIST
UFC PROHIBITED LIST Effective June 1, 2021 THE UFC PROHIBITED LIST UFC PROHIBITED LIST Effective June 1, 2021 PART 1. Except as provided otherwise in PART 2 below, the UFC Prohibited List shall incorporate the most current Prohibited List published by WADA, as well as any WADA Technical Documents establishing decision limits or reporting levels, and, unless otherwise modified by the UFC Prohibited List or the UFC Anti-Doping Policy, Prohibited Substances, Prohibited Methods, Specified or Non-Specified Substances and Specified or Non-Specified Methods shall be as identified as such on the WADA Prohibited List or WADA Technical Documents. PART 2. Notwithstanding the WADA Prohibited List and any otherwise applicable WADA Technical Documents, the following modifications shall be in full force and effect: 1. Decision Concentration Levels. Adverse Analytical Findings reported at a concentration below the following Decision Concentration Levels shall be managed by USADA as Atypical Findings. • Cannabinoids: natural or synthetic delta-9-tetrahydrocannabinol (THC) or Cannabimimetics (e.g., “Spice,” JWH-018, JWH-073, HU-210): any level • Clomiphene: 0.1 ng/mL1 • Dehydrochloromethyltestosterone (DHCMT) long-term metabolite (M3): 0.1 ng/mL • Selective Androgen Receptor Modulators (SARMs): 0.1 ng/mL2 • GW-1516 (GW-501516) metabolites: 0.1 ng/mL • Epitrenbolone (Trenbolone metabolite): 0.2 ng/mL 2. SARMs/GW-1516: Adverse Analytical Findings reported at a concentration at or above the applicable Decision Concentration Level but under 1 ng/mL shall be managed by USADA as Specified Substances. 3. Higenamine: Higenamine shall be a Prohibited Substance under the UFC Anti-Doping Policy only In-Competition (and not Out-of- Competition). -

)&F1y3x PHARMACEUTICAL APPENDIX to THE
)&f1y3X PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE )&f1y3X PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 3 Table 1. This table enumerates products described by International Non-proprietary Names (INN) which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service (CAS) registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known. Product CAS No. Product CAS No. ABAMECTIN 65195-55-3 ACTODIGIN 36983-69-4 ABANOQUIL 90402-40-7 ADAFENOXATE 82168-26-1 ABCIXIMAB 143653-53-6 ADAMEXINE 54785-02-3 ABECARNIL 111841-85-1 ADAPALENE 106685-40-9 ABITESARTAN 137882-98-5 ADAPROLOL 101479-70-3 ABLUKAST 96566-25-5 ADATANSERIN 127266-56-2 ABUNIDAZOLE 91017-58-2 ADEFOVIR 106941-25-7 ACADESINE 2627-69-2 ADELMIDROL 1675-66-7 ACAMPROSATE 77337-76-9 ADEMETIONINE 17176-17-9 ACAPRAZINE 55485-20-6 ADENOSINE PHOSPHATE 61-19-8 ACARBOSE 56180-94-0 ADIBENDAN 100510-33-6 ACEBROCHOL 514-50-1 ADICILLIN 525-94-0 ACEBURIC ACID 26976-72-7 ADIMOLOL 78459-19-5 ACEBUTOLOL 37517-30-9 ADINAZOLAM 37115-32-5 ACECAINIDE 32795-44-1 ADIPHENINE 64-95-9 ACECARBROMAL 77-66-7 ADIPIODONE 606-17-7 ACECLIDINE 827-61-2 ADITEREN 56066-19-4 ACECLOFENAC 89796-99-6 ADITOPRIM 56066-63-8 ACEDAPSONE 77-46-3 ADOSOPINE 88124-26-9 ACEDIASULFONE SODIUM 127-60-6 ADOZELESIN 110314-48-2 ACEDOBEN 556-08-1 ADRAFINIL 63547-13-7 ACEFLURANOL 80595-73-9 ADRENALONE -

Us Anti-Doping Agency
2019U.S. ANTI-DOPING AGENCY WALLET CARDEXAMPLES OF PROHIBITED AND PERMITTED SUBSTANCES AND METHODS Effective Jan. 1 – Dec. 31, 2019 CATEGORIES OF SUBSTANCES PROHIBITED AT ALL TIMES (IN AND OUT-OF-COMPETITION) • Non-Approved Substances: investigational drugs and pharmaceuticals with no approval by a governmental regulatory health authority for human therapeutic use. • Anabolic Agents: androstenediol, androstenedione, bolasterone, boldenone, clenbuterol, danazol, desoxymethyltestosterone (madol), dehydrochlormethyltestosterone (DHCMT), Prasterone (dehydroepiandrosterone, DHEA , Intrarosa) and its prohormones, drostanolone, epitestosterone, methasterone, methyl-1-testosterone, methyltestosterone (Covaryx, EEMT, Est Estrogens-methyltest DS, Methitest), nandrolone, oxandrolone, prostanozol, Selective Androgen Receptor Modulators (enobosarm, (ostarine, MK-2866), andarine, LGD-4033, RAD-140). stanozolol, testosterone and its metabolites or isomers (Androgel), THG, tibolone, trenbolone, zeranol, zilpaterol, and similar substances. • Beta-2 Agonists: All selective and non-selective beta-2 agonists, including all optical isomers, are prohibited. Most inhaled beta-2 agonists are prohibited, including arformoterol (Brovana), fenoterol, higenamine (norcoclaurine, Tinospora crispa), indacaterol (Arcapta), levalbuterol (Xopenex), metaproternol (Alupent), orciprenaline, olodaterol (Striverdi), pirbuterol (Maxair), terbutaline (Brethaire), vilanterol (Breo). The only exceptions are albuterol, formoterol, and salmeterol by a metered-dose inhaler when used -

Obesity Drugs: Too Much Harm, for Far Too Long
Obesity drugs: too much harm, for far too long In 2016, a British team studied the causes for the market withdrawals of weight-loss drugs. They identified 25 drugs that had been withdrawn from markets around the world between 1964 and 2009. The mechanism of 22 of these drugs involved monoamine neurotransmitters (dopamine, noradrenaline or serotonin); examples include benfluorex, fenfluramine, phentermine (combined with topiramate in the United States) and sibutramine. One drug, rimonabant, was a cannabinoid EDITORIAL derivative, and the two others acted on the thyroid (1). 80% of the market withdrawals were based on data from spontaneous reports, involving cardiac disorders for 8 drugs, psychiatric disorders for 7 drugs, and abuse or dependence for 13 drugs. Drug-attributed deaths had occurred with 7 of the drugs. The median time between market introduction and the first report of a serious adverse effect was 10 years; and the median time between the first report of a serious adverse effect and the first market withdrawal anywhere in the world was 11 years. Fenfluramine was marketed for 24 years before its worldwide withdrawal in 1997 for heart valve disease. Benfluorex was marketed in France for 33 years before its withdrawal in 2009 for cardiotoxicity; yet the heart valve disorders resembled those caused by fenfluramine and the chemical structures of these two drugs are very similar (2). In France, phentermine was marketed from 1962 to 1988. Sibutramine was withdrawn in Europe in 2010, about 9 years after authorisation; and rimonabant was withdrawn in Europe in 2009, about 2 years after authorisation (1,3,4). -

Part I Biopharmaceuticals
1 Part I Biopharmaceuticals Translational Medicine: Molecular Pharmacology and Drug Discovery First Edition. Edited by Robert A. Meyers. © 2018 Wiley-VCH Verlag GmbH & Co. KGaA. Published 2018 by Wiley-VCH Verlag GmbH & Co. KGaA. 3 1 Analogs and Antagonists of Male Sex Hormones Robert W. Brueggemeier The Ohio State University, Division of Medicinal Chemistry and Pharmacognosy, College of Pharmacy, Columbus, Ohio 43210, USA 1Introduction6 2 Historical 6 3 Endogenous Male Sex Hormones 7 3.1 Occurrence and Physiological Roles 7 3.2 Biosynthesis 8 3.3 Absorption and Distribution 12 3.4 Metabolism 13 3.4.1 Reductive Metabolism 14 3.4.2 Oxidative Metabolism 17 3.5 Mechanism of Action 19 4 Synthetic Androgens 24 4.1 Current Drugs on the Market 24 4.2 Therapeutic Uses and Bioassays 25 4.3 Structure–Activity Relationships for Steroidal Androgens 26 4.3.1 Early Modifications 26 4.3.2 Methylated Derivatives 26 4.3.3 Ester Derivatives 27 4.3.4 Halo Derivatives 27 4.3.5 Other Androgen Derivatives 28 4.3.6 Summary of Structure–Activity Relationships of Steroidal Androgens 28 4.4 Nonsteroidal Androgens, Selective Androgen Receptor Modulators (SARMs) 30 4.5 Absorption, Distribution, and Metabolism 31 4.6 Toxicities 32 Translational Medicine: Molecular Pharmacology and Drug Discovery First Edition. Edited by Robert A. Meyers. © 2018 Wiley-VCH Verlag GmbH & Co. KGaA. Published 2018 by Wiley-VCH Verlag GmbH & Co. KGaA. 4 Analogs and Antagonists of Male Sex Hormones 5 Anabolic Agents 32 5.1 Current Drugs on the Market 32 5.2 Therapeutic Uses and Bioassays -

A10 Anabolic Steroids Hardcore Info
CONTENTS GENERAL INFORMATION 3 Anabolic steroids – What are they? 4 How do they Work? – Aromatisation 5 More molecules – More problems 6 The side effects of anabolic steroids 7 Women and anabolic steroids 8 Injecting steroids 9 Abscesses – Needle Exchanges 10 Intramuscular injection 11 Injection sites 12 Oral steroids – Cycles – Stacking 13 Diet 14 Where do steroids come from? Spotting a counterfeit 15 Drug Information – Drug dosage STEROIDS 16 Anadrol – Andriol 17 Anavar – Deca-Durabolin 18 Dynabolon – Durabolin – Dianabol 19 Esiclene – Equipoise 20 Primobolan Depot – Proviron – Primobolan orals – Pronobol 21 Sustanon – Stromba, Strombaject – Testosterone Cypionate Testosterone Enanthate 22 Testosterone Propionate – Testosterone Suspension 23 Trenbolone Acetate – Winstrol OTHER DRUGS 24 Aldactone – Arimidex 25 Clenbuterol – Cytomel 26 Ephedrine Hydrochloride – GHB 27 Growth Hormone 28 Insulin 30 Insulin-Like Growth Factor-1 – Human Chorionic Gonadotrophin 31 Tamoxifen – Nubain – Recreational Drugs 32 Steroids and the Law 34 Glossary ANABOLIC STEROIDS People use anabolic steroids for various reasons, some use them to build muscle for their job, others just want to look good and some use them to help them in sport or body building. Whatever the reason, care needs to be taken so that as little harm is done to the body as possible because despite having muscle building effects they also have serious side effects especially when used incorrectly. WHAT ARE THEY? Anabolic steroids are man made versions of the hormone testosterone. Testosterone is the chemical in men responsible for facial hair, deepening of the voice and sex organ development, basically the masculine things Steroids are in a man. used in medicine to treat anaemia, muscle weakness after These masculine effects surgery etc, vascular are called the androgenic disorders and effects of testosterone.