EXHIBIT a Financial Consulting Report Related to the Proposed Transfer of Certain Assets from Eastern Connecticut Health Network, Inc
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

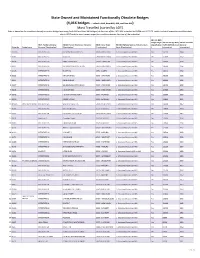
State Owned and Maintained Structurally Deficient Bridges
State Owned and Maintained Structurally Deficient Bridges (4,016 bridges - includes NHS, Non-NHS, NBI, and Non-NBI) Most Travelled (sorted by ADT) Data is based on the condition data of our entire bridge inventory (both NBI and Non-NBI bridges) at the time of the 2018 NBI submittal to FHWA on 03/15/18, which included inspection condition data due in 2017 and the most recent inspection condition data at the time of the submittal NBI 29: Average NBI 112: NBIS Daily Traffic (ADT) NBI 27: Year NBI 7: Facility Carried by Structure NBI 6A: Feature Intersected: NBI 4: City or Town NBI 104: Highway System of the Bridge Length [General Built [General Bridge No. Bridge Name [Classification] Narrative [Classification] [Classification] Inventory Route [Classification] [Classification] Information] Information] YANKEE DOODLE 1 00059 BRIDGE INTERSTATE-95 NORWALK RV,HENDRICKS AVE 56060 - NORWALK 1 - Structure/Route is on NHS Yes 145000 1957 2 06798 INTERSTATE-95 STUBBY PLAIN BROOK 47535 - MILFORD 1 - Structure/Route is on NHS No 137500 1958 3 00162 INTERSTATE-95 METRO NORTH 82870 - WEST HAVEN 1 - Structure/Route is on NHS Yes 136400 1956 4 03093 INTERSTATE 91 N FRONT ST & QUINN RIVER 52070 - NEW HAVEN 1 - Structure/Route is on NHS Yes 133900 1964 5 03094 INTERSTATE-91 AMTRAK RAILROAD 52070 - NEW HAVEN 1 - Structure/Route is on NHS Yes 133900 1965 BYRAM RIVER 6 00001 BRIDGE INTERSTATE-95 BYRAM RIVER,S WATER ST 33620 - GREENWICH 1 - Structure/Route is on NHS Yes 131600 1958 7 00062 INTERSTATE-95 ROUTE 33 83500 - WESTPORT 1 - Structure/Route is on NHS -
Final Report
CAPITOL REGION COUNCIL OF GOVERNMENTS FINAL REPORT SILVER LANE (SR 502) CORRIDOR STUDY EAST HARTFORD, CT February 19, 2020 Silver Lane Corridor Study Draft Final Report February 19, 2020 Prepared for: Capitol Region Council of Governments 241 Main Street Hartford, CT 06106 Prepared by: TranSystems Corporation 530 Preston Avenue Meriden, CT 06450 With the assistance of: Fitzgerald & Halliday Inc. 416 Asylum Street Hartford, CT, 06103 Silver Lane CorridorCorridor Study – Final Report TABLE OF CONTENTS Executive Summary ........................................................................................................................................................... 1 Existing Conditions Assessment ................................................................................................................................ 2 Future Conditions Assessment .................................................................................................................................. 4 Analysis of Alternatives and Recommendations .................................................................................................... 6 Corridor-wide Recommendations ....................................................................................................................... 6 Location-based Improvements .............................................................................................................................. 7 Interim Improvements .............................................................................................................................................. -
State Owned and Maintained Functionally Obsolete Bridges
State Owned and Maintained Functionally Obsolete Bridges (4,016 bridges - includes NHS, Non-NHS, NBI, and Non-NBI) Most Travelled (sorted by ADT) Data is based on the condition data of our entire bridge inventory (both NBI and Non-NBI bridges) at the time of the 2018 NBI submittal to FHWA on 03/15/18, which included inspection condition data due in 2017 and the most recent inspection condition data at the time of the submittal NBI 112: NBIS Bridge Length NBI 29: Average Daily NBI 27: Year Built NBI 7: Facility Carried by NBI 6A: Feature Intersected: Narrative NBI 4: City or Town NBI 104: Highway System of the Inventory [Classification Traffic (ADT) [General [General Bridge No. Bridge Name Structure [Classification] [Classification] [Classification] Route [Classification] ] Information] Information] 1 00105A INTERSTATE-95 METRO NORTH & CITY ST'S 08070 - BRIDGEPORT 1 - Structure/Route is on NHS Yes 161300 1999 2 00164 INTERSTATE-95 ROUTE 10 52070 - NEW HAVEN 1 - Structure/Route is on NHS Yes 152800 1957 3 00038 INTERSTATE-95 HAMILTON AVENUE 73070 - STAMFORD 1 - Structure/Route is on NHS Yes 149600 1958 4 00014 INTERSTATE-95 METRO NORTH RR & STATION 33620 - GREENWICH 1 - Structure/Route is on NHS Yes 146000 1958 5 00045 INTERSTATE-95 ROUTE 136 18850 - DARIEN 1 - Structure/Route is on NHS Yes 144100 1952 6 00033 INTERSTATE-95 MAPLE AVENUE 73070 - STAMFORD 1 - Structure/Route is on NHS Yes 143900 1958 7 00011 INTERSTATE-95 DAVIS AVENUE 33620 - GREENWICH 1 - Structure/Route is on NHS Yes 143800 1958 8 00027 INTERSTATE-95 SSR 493(WASHINGTON -

Town of Glastonbury Request for Proposal Restaurant Lease at Minnechaug Golf Course Rpgl-2020-14
TOWN OF GLASTONBURY REQUEST FOR PROPOSAL RESTAURANT LEASE AT MINNECHAUG GOLF COURSE RPGL-2020-14 The Town of Glastonbury will be accepting proposals from qualified firms or individuals to operate the restaurant at the Town-owned nine-hole Minnechaug Golf Course. Interested individuals or firms may obtain proposal documents and project details from the Purchasing Agent, 2155 Main Street, Glastonbury, CT 06033 or via the Town’s website at www.glastonbury-ct.gov. An optional pre-proposal site inspection and meeting will be held on March 11, 2020 at 10:00 a.m. at the golf course at 16 Fairway Crossing in Glastonbury. Respondents are strongly encouraged to attend. Proposals must be submitted to the Office of the Purchasing Agent, Town Hall, 2155 Main Street, Glastonbury, Connecticut 06033, no later than 11:00 a.m. on March 17, 2020. LATE PROPOSALS WILL NOT BE ACCEPTED. The Town reserves the right to waive informalities or reject any part of, or the entire proposal, when said action is deemed to be in the best interests of the Town. All sealed proposals must be submitted to the Office of the Purchasing Agent no later than the time and date indicated. An Affirmative Action/Equal Opportunity Employer. Minority/Women /Disadvantaged Business Enterprises are encouraged to submit a proposal. Mary F. Visone Purchasing Agent 1 Request for Proposal Restaurant Lease at Minnechaug Golf Course RPGL-2020-14 TABLE OF CONTENTS SECTION I GENERAL INFORMATION BACKGROUND SECTION II CONSIDERATIONS & RESTRICTIONS & OTHER REQUIREMENTS SCOPE OF SERVICES SECTION III -
Final Report
CAPITOL REGION COUNCIL OF GOVERNMENTS DRAFT FINAL REPORT SILVER LANE (SR 502) CORRIDOR STUDY EAST HARTFORD, CT January 14, 2020 Silver Lane Corridor Study Draft Final Report January 14, 2020 Prepared for: Capitol Region Council of Governments 241 Main Street Hartford, CT 06106 Prepared by: TranSystems Corporation 530 Preston Avenue Meriden, CT 06450 With the assistance of: Fitzgerald & Halliday Inc. 416 Asylum Street Hartford, CT, 06103 Silver Lane Corridor Study – Final Report TABLE OF CONTENTS Executive Summary ........................................................................................................................................................... 1 Existing Conditions Assessment ................................................................................................................................ 2 Future Conditions Assessment .................................................................................................................................. 4 Analysis of Alternatives and Recommendations .................................................................................................... 6 Corridor-wide Recommendations ....................................................................................................................... 6 Location-based Improvements .............................................................................................................................. 7 Interim Improvements .............................................................................................................................................. -

Downtown North Historic District
OMts Form 1C -900 RPCFr^.H ??RO uSl/NrS iNrihf Registration Form (Rev. 8-86) 1024-0018 PROPERTY >AME D~oWnt< >wn North Historic District, Hartford. CT Pagel United States ] teparti lent of the Interior National Register of Historic Places Registration Form WAT REGISTER OF HiSTCtfiC PUCES NATIONAL PARK SERVICE 1. Name of Property historic name NA other names/site number Downtown North Historic District 2. Location street & number 480-484, 490r 500r 506-512. 529-543 Ann Street; 35-37 Atlantic? Street: 24 Ely Street; 21 lr 220r 225-23 l r 249r 263-26Sr 269-273r 275-277 High Street: 1279-1283r 1293-1297, 1301-1307, 1304, 1306. 1313-1317, 1325-1329, 1331-1337, 135S-1357r 13S9-1363r 1391-1405 Main Street; 180 Pleasant Street________________u not for publication MA city or town Hartford vicinity NA state Connecticut code CT county Hartford codejQQl zip code 06112 3, State/Federal Agency Certification As the designated authority under the National Historic Preservation Act of 1986, as amended, 1 hereby certify that this X nomination __ request for determination of eligibility meets the documentation standards for registering properties in the National Register of Historic Places and meets the procedural and professional requirements set forth in 36 CFR Part 60. In my opinion, the property % meets __ does not meet the National Register Criteria. I recommend that this property be considered significant _ nationally _ statewide js;_ locally. ( _ See contjjttwrti^sEeet for additional comments.) Signature of certitymt5"official Date Acting Director/Deputy State Historic Preservation Officer State or Federal agency and bureau In my opinion, the property __ meets does not meet the National Register criteria. -

Complete Streets Report: Breaking Through Barriers for Non-Motorized
Completesummer 2013 StreetsReport iers for Non-Motorized rr tion Users a orta Br B sp ea h n kin g ra g Throu T Prepared In-House by Staff of the State of Connecticut Department of Transportation 2800 Berlin Turnpike P.O. Box 317546 Newington, CT 06131-7546 In Cooperation with the U.S. Department of Transportation’s Federal Highway Administration and the Federal Transit Administration Web Site Address www.ct.gov/dot/completestreets Contents Message from the Commissioner 1 A Year in Review 3 Achievements 3 Real World Application 3 Progressive Steps 3 Complete Streets Strategies 5 Design, Maintenance, and Infrastructure 6 Design Considerations 6 Internal Task Force 6 Training Events 7 Bicycle and Pedestrian Travel Needs Assessment Form 8 Sidewalk Policy 10 Eleven-Foot Travel Lanes 12 Cyclist Friendly Amenities for Transit Riders 14 ADA Upgrades at Signalized Intersections 16 Project Highlights 18 East Coast Greenway (ECG) Signage 18 East Hartford “Road Diet” 20 Putnam Bridge Access across the Connecticut River 24 CTfastrak 26 Feasibility Study for a Merritt Parkway Trail 30 Addressing Stratford Sidewalks 34 Alternative Systems 36 Programmatic Successes 40 Safe Routes to Schools (SRTS) Program 40 Share the Road Campaign 42 Improving Bicycle and Pedestrian Access 44 Addressing Gaps in the State Network of Multi-Use Trails 46 Assistance with Local and Regional Priorities 50 Looking Ahead 51 What’s Next 51 Challenges Yet to Face 51 Exciting News! Dear Non-Motorized Transportation Enthusiasts, It is with great pleasure that I share with you the Department of Transportation’s first-ever report on Complete Streets. -

AGENDA COVENTRY TOWN COUNCIL MEETING May 5, 2014 7:30 PM Town Hall Annex
AGENDA COVENTRY TOWN COUNCIL MEETING May 5, 2014 7:30 PM Town Hall Annex 1. Call To Order, Roll Call 2. Pledge Of Allegiance To The Flag 3. Audience Of Citizens: (30 Minutes - 5 minutes maximum per citizen) 3.A. Resolution: Dennis Dittrich, CVFA 50 Years Of Service 4. Acceptance Of Minutes: 4.A. April 21, 2014 (E) Documents: APRIL 21, 2014.PDF 5. Consent Agenda: All items listed with an asterisk (*) will be acted on by one motion. There will be no separate discussion on these items unless a Council member so requests, in which case, the item will be removed from the consent agenda and considered in its normal sequence on the agenda. 6. Reports: 6.A. Report Of Chairperson - Jeff Shorts 6.B. Report Of Council Members 6.C. Steering: Mike Griswold, Chairperson 6.C.1. Reappointments (E) 6.C.1.a. Economic Development Commission #205: Belsito (E) Documents: STATEMENT OF INTEREST BELSITO.PDF 6.C.2. Appointments (E) 6.C.2.a. Conservation Commission #204: Coss (E) Documents: STATEMENT OF INTEREST COSS.PDF 6.C.2.b. Zoning Board Of Appeals #129: Vinkels (E) Documents: STATEMENT OF INTEREST VINKELS.PDF 6.C.3. * Minutes, April 28, 2014 (E) Documents: STEERING 4-28-14.PDF 6.D. Finance: Wayne Post, Chairperson 6.D.1. * Minutes, April 21, 2014 (E) Documents: FINANCE MINUTES 4-21-14.PDF 6.E. COVRRA: John A. Elsesser 6.F. Town Manager: John A. Elsesser 6.F.1. Projects Update: 6.F.2. UConn Transportation Study Project Accepted (E) Documents: PATHWAYS MEMO.PDF, PATHWAYS PRELIMINARY STUDY SCOPE 2014_04_28.PDF 6.F.3. -
Horsley Witten Group Stormwater Management Planning Services
Horsley Witten Group Sustainable Environmental Solutions 55 Dorrance Street, Suite 403 • Providence, RI • 02903 Phone - 401-272-1717 • Fax - 401-437-8368 • www.horsleywitten.com Qualifications for Stormwater Management Planning Services Capitol Region Council of Governments August 31, 2016 HW conducts training on how to design, construct and maintain bioretention facilities that includes hands-on Submitted to: practice installation at Roger Williams Park in Maureen Goulet Providence, RI Capitol Region Council of Governments 241 Main Street, 4th Floor Hartford, CT 06106 Submitted by: Horsley Witten Group, Inc. August 31, 2016 Maureen Goulet Capitol Region Council of Governments 241 Main Street, 4th Floor Hartford, CT 06106 Re: Qualifications for Professional Services Stormwater Management Planning Services Dear Ms. Goulet: Horsley Witten Group, Inc. (HW) is pleased to submit the enclosed qualifications to provide professional services assisting the Capital Region Council of Governments (CRCOG) with development of stormwater management planning services to assist member communities. HW has teamed with Fitzgerald & Halliday, Inc. (FHI) to respond to the Request for Information. The partnering of our firms enables us to provide CRCOG with highly responsive, effective, innovative, and comprehensive services to address the new MS4 permit requirements. HW will be the lead consultant on this project. HW is a full‐service planning, engineering, and environmental‐science firm with offices located in Sandwich and Boston, Massachusetts, and Providence, Rhode Island. Incorporated in 1988, HW consists of professional engineers, landscape architects, community planners, GIS technicians, environmental analysts, surveyors, and supporting personnel. HW staff has extensive experience providing MS4 stormwater program compliance services throughout New England; with particular attention given to new NPDES MS4 permit conditions in MA and NH as well as sustainable stormwater financing, training, and implementation of green infrastructure to address impaired waters. -

Stormwater Management Plan
STORMWATER MANAGEMENT PLAN TOWN OF MANCHESTER PREPARED BY: ADAM G. FOX SENIOR PROJECT ENGINEER JOSEPH MAGDOL, P.E. SENIOR PROJECT MANAGER Submitted to: Submitted by: Mr. Jeff LaMalva, P.E. HRP Associates, Inc. Assistant Town Engineer Engineering & Geology Town of Manchester 167 New Britain Avenue P.O. Box 191 Plainville, Connecticut Manchester, CT 06045-0191 J:\MANTO\MAN3000.MC\Stormwater Management Plan.doc TABLE OF CONTENTS Section Page Key Definitions ......................................................................................................................... i Acronyms ................................................................................................................................iii INTRODUCTION ....................................................................................................................1 A. Background ..................................................................................................................1 B. Qualifying Local Program............................................................................................. 2 C. Qualifying State Programs ........................................................................................... 2 D. Communications .......................................................................................................... 3 E. Urbanized Areas.......................................................................................................... 3 F. Town Wetlands........................................................................................................... -

Stamford's Stormwater Management Plan
Stormwater Management Plan Permit No. CT0030279 City of Stamford Stamford, Connecticut September 2, 2014 56 Quarry Road Trumbull, Connecticut About this Document The City of Stamford’s Stormwater Management Plan provides general guidance for developing a plan for non-structural and structural controls to reduce pollutants in stormwater runoff from post development activities in residential, commercial, industrial areas, and at public facilities. This Stormwater Management Plan (SMP) is written in an attempt to comply with the NPDES Permit for discharge of stormwater from Stamford’s municipal separate storm sewer system (MS4) on issued June 4, 2013. This SMP details requirements intended to address compliance with the NPDES Permit. The City of Stamford also has and/or may develop numerous other Planning, Zoning, Engineering, Environmental Protection Board and other regulations, guidelines and practices that apply to development within the City of Stamford. These may be more restrictive than those stated below, and it is the property owner and/or developer’s responsibility to ensure compliance with all applicable requirements. Table of Contents Stormwater Management Plan City of Stamford Executive Summary ............................................................................. vii 1 Introduction ................................................................................... 1 1.1 Overview .......................................................................................................................... 1 1.2 Overview of Selected -

Manchester's Plan of Conservation and Development
2012 Plan of Conservation and Development VISION – ASPIRATIONS – ACTIONS Adopted: December 17, 2012 Effective: January 14, 2013 ACKNOWLEDGEMENTS Planning and Zoning Commission Joseph Diminico, Chairman Kevin Dougan, Vice Chairman Andy Kidd, Secretary Horace Brown Eric Prause Anthony Petrone Susan Shanbaum John Chaput Michael Stebe Eugene Sierakowski Board of Directors Leo V. Diana, Mayor Jay Moran, Deputy Mayor Lisa P. O’Neill, Secretary Steve Gates Susan Holmes Rudy C. Kissmann Cheri A. Pelletier John D. Topping Mark D. Tweedie Planning Department Staff Mark Pellegrini, AICP Director of Planning and Economic Development Gary A. Anderson, AICP Senior Planner-Comprehensive/Special Projects Renata Bertotti, AICP Senior Planner-Current Planning Matthew R. Bordeaux Environmental Planner/Wetlands Agent Heather Donoghue Community Development Program Manager Manchester 2020 Participants Joie Aiken Bob Eckert Jim MacDonald Bruce Samborski Scott Aiken Christina Edelwich Doug MacGillvary Bob Samuelson Nick Albano Nicholas Ehr Phil MacVane Bettylou Sandy Peg Aldrich Mary Ann Ettinger Kathy Maffe Robert Santy Nicolas Arias Lauren Falzarano Amelia Mariotti Mary Savage-Dunham Barbara Armentano Mike Farina Martha Marteney Jack Sayre Mary Ann Attinger Eileen Faust James Martin Jan Sayre Betsy Baker David Fiereck Martha Martinez Bob Schneider Evelyn Banning Jennifer Fiereck Jon Marx Bob Sekoll Bob Barker Herb Flink Jeanne Matthew Sharon Sekoll Linda Barker Bruce Forde Steve Mazdski Bob Shanbaum Malcolm Barlow Donna Forde Lauren Mcavoy Susan Shanbaum Susan Barlow Margaret Forman Linnea McCaffrey Bill Siddons Maureen Barton Leslie Frey Jack McCoy Kathy Siddons George Beauregard Dan Gallagher Doug McDonough Chris Silver Jeri Beckford John Garaventa Charlie McFall Glenda Sinnamon Joni Belman Steve Gates Rita McParland Joe Sinnamon Joshua Beltre’ Sally Gifford Sarah Melquist Ed Slegeski Wilma Beltre’ Charles Gilbert Shelby Mertes Dave Smith Hector Beltre’, Sr.