UCSF TMS and Neuromodulation Service ATHQ PATIENT NAME
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Still the Leading Antidepressant After 40
BRITISH JOURNAL OF PSYCHIATRY "2001), 178, 129^144 REVIEW ARTICLE Amitriptyline vv.therest:stilltheleading METHOD Inclusion criteria antidepressant after 40 years of randomised All RCTs comparing amitriptyline with any y other tricyclic,heterocyclic or SSRI were in- controlled trials cluded. Crossover studies were excluded. Studies adopting any criteria to define CORRADO BARBUI and MATTHEW HOTOPF patients suffering from depression were included; a concurrent diagnosis of another psychiatric disorder was not considered an exclusion criterion. Trials in patients with depression with a concomitant medical ill- Background Tricyclic antidepressants Amitriptyline is one of the first `reference' ness were not included in this review. have similar efficacy and slightly lower tricyclic antidepressants TCAs). Over the past 40 years a number of newer tricyclics, tolerability than selective serotonin Search strategy heterocyclics and selective serotonin re- Relevant studies were located by searching reuptakeinhibitorsreuptake inhibitors SSRIs).However, uptake inhibitors SSRIs) have been intro- the Cochrane Collaboration Depression, there are no systematic reviews assessing duced Garattini et aletal,1998). Despite Anxiety and Neurosis Controlled Trials several large systematic reviews comparing amitriptyline, the reference tricyclic drug, Register CCDANCTR). This specialised tricyclics and SSRIs there is no clear agree- vv. other tricyclics and SSRIs directly. register is regularly updated by electronic ment over first-line treatment of depression Medline,Embase,PsycINFO,LILACS, SongSong et aletal,1993; Anderson & Tomenson, Aims ToreviewTo review the tolerability and Psyndex,CINAHL,SIGLE) and non-electro- 1995; Montgomery & Kasper,1995; efficacy of amitriptyline inthe nicnicliterature searches. The register was HotopfHotopf et aletal,1996; Canadian Coordinating management of depression. searched using the following terms: Office for Health Technology Assessment, AMITRIPTYLIN**AMITRIPTYLIN oror AMITRILAMITRIL oror ELA-ELA- 19971997aa). -

(12) Patent Application Publication (10) Pub. No.: US 2005/0065218A1 Migeon Et Al
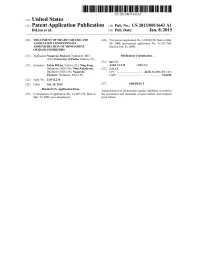
US 2005.0065218A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2005/0065218A1 Migeon et al. (43) Pub. Date: Mar. 24, 2005 (54) UTILIZATION OF ALVERINE, ALONE OR IN (30) Foreign Application Priority Data COMBINATION WITH TRICYCLC ANTDEPRESSANT OR A SPECIFIC Jun. 13, 2003 (FR).............................................. O307176 SEROTONIN REUPTAKE INHIBITOR FOR Apr. 30, 2004 (FR).............................................. O404639 THE TREATMENT OF DEPRESSION Publication Classification (76) Inventors: Jacques Migeon, Seattle, WA (US); Frederic Revah, Paris (FR) (51) Int. C.7 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - A61K 31/137 (52) U.S. Cl. .............................................................. 514/649 Correspondence Address: SESD LARDNER (57) ABSTRACT 3000 KSTREET NW WASHINGTON, DC 20007 (US) The present invention relates to the utilization of Alverine or its metabolites, alone or in combination with a tricyclic (21) Appl. No.: 10/866,079 antidepressant or a Specific Serotonin reuptake inhibitor, for the preparation of pharmaceutical compositions for the (22) Filed: Jun. 14, 2004 treatment of depression. 80 120 OO 8 O 6 O 40 20 t Excipicnts Alverine Alverine Alverine Imiprannine (1% methylcellulose) Citate Citrate Citrate 10 mg/kg 3 mg/kg 10 mg/kg 30 mg/kg Patent Application Publication Mar. 24, 2005 Sheet 1 of 4 US 2005/0065218 A1 Excipients Alverine Alveline Alveline Inipramine (1% methylcellulose) Citrate Citrate Citrate 10 mg/kg 3 mg/kg 10 mg/kg 30 mg/kg Fi gure US 2005/0065218A1 Imipramine 30 mg/kg Figure 2 Patent Application Publication Mar. 24, 2005 Sheet 3 of 4 US 2005/0065218A1 20 Vehicle + Whicule -- Averine Alvérine Vehicule + Alverine Vehicule imipramine 3 ring/kg it 3 mg/kg t- Impramine 10 mg/kg + 3 mg/kg Wellicule imipramine 10 mg/kg Vehicule 3 mg/kg Figure 3 Patent Application Publication Mar. -

'Gating' Residues Ile199 and Tyr326 in Human Monoamine Oxidase B
The ‘gating’ residues Ile199 and Tyr326 in human monoamine oxidase B function in substrate and inhibitor recognition Erika M. Milczek1,*, Claudia Binda2, Stefano Rovida2, Andrea Mattevi2 and Dale E. Edmondson1 1 Departments of Chemistry and Biochemistry, Emory University, Atlanta, Georgia, USA 2 Department of Genetics and Microbiology, University of Pavia, Italy Keywords The major structural difference between human monoamine oxidases A dipartite to monopartite cavity conversion; (MAO A) and B (MAO B) is that MAO A has a monopartite substrate inhibitor specificity; monoamine oxidase B; cavity of 550 A˚3 volume and MAO B contains a dipartite cavity struc- mutations of gating residues; structure of ture with volumes of 290 A˚3 (entrance cavity) and 400 A˚3 (substrate methylene blue complex cavity). Ile199 and Tyr326 side chains separate these two cavities in MAO Correspondence B. To probe the function of these gating residues, Ile199Ala and Ile199Ala- D. E. Edmondson, Department of Tyr326Ala mutant forms of MAO B were investigated. Structural data on Biochemistry, Emory University, 1510 the Ile199Ala MAO B mutant show no alterations in active site geometries Clifton Road, Atlanta, GA 30322, USA compared with wild-type enzyme while the Ile199Ala-Tyr326Ala MAO B Fax: +1 404 727 2738 mutant exhibits alterations in residues 100–103 which are part of the loop Tel: +1 404 727 5972 gating the entrance to the active site. Both mutant enzymes exhibit catalytic E-mail: [email protected] properties with increased amine KM but unaltered kcat values. The altered *Present address KM values on mutation are attributed to the influence of the cavity struc- Department of Chemistry, Princeton ture in the binding and subsequent deprotonation of the amine substrate. -

2019 Instrumentation and Consumable Catalog 2 INSTRUMENTATION and CONSUMABLE CATALOG
PRODUCT CATALOG 2019 Instrumentation and Consumable Catalog 2 INSTRUMENTATION AND CONSUMABLE CATALOG Resolvex® A200 Part Numbers: A200 96: 253-1160 Resolvex® A200 96 Resolvex A200 Standalone work station for automated sample preparation. The compact benchtop offers the one stop solution for automating sample preparation utilizing creation of multiple work flows, and programmable dispensing of up to 11 solvents. Along with its innovative positive pressure system leading to clean samples, improving accuracy, throughput and enhancing the Life time of your analytical instrument. The A200 comes with an easy to use touch screen interface allowing for easy set up of multiple work flows. In addition the light curtain safety feature will release gas pressure when manifold is activated to prevent any injuries. INSTRUMENTATION AND CONSUMABLE CATALOG 3 Resolvex® A100 Part Numbers: A100 96: 253-0019 A100 48: 253-0014 Resolvex® A100 Standalone work station for automated sample preparation. The compact benchtop offers the one stop solution for automating sample preparation utilizing creation of multiple work flows, and programmable dispensing of up to 11 solvents. Along with its innovative positive pressure system leading to clean samples, improving accuracy, throughput and enhancing the Life time of your analytical instrument. The A100 comes in 96 and 4 configuration allowing for for automated Work Flow solutions in multiple SPE formats. 4 INSTRUMENTATION AND CONSUMABLE CATALOG Resolvex® M10 96/M10 96 XT/M10 48 Part Numbers: M10 96 XT: 288-0006 M10 96: 288-0001 M10 48: 289-0004 Resolvex® M10 Standalone work station for Positive Pressure solid phase extraction. The manual Resolvex M10 48 and 96 are positive pressure manifold for 1, 3, and 6 ml cartridges, or 1ml 96 well plates. -

Still the Leading Antidepressant After 40 Years of Randomised Controlle
BRITISH JOURNAL OF PSYCHIATRY "2001), 178, 129^144 REVIEW ARTICLE Amitriptyline vv.therest:stilltheleading METHOD Inclusion criteria antidepressant after 40 years of randomised All RCTs comparing amitriptyline with any y other tricyclic,heterocyclic or SSRI were in- controlled trials cluded. Crossover studies were excluded. Studies adopting any criteria to define CORRADO BARBUI and MATTHEW HOTOPF patients suffering from depression were included; a concurrent diagnosis of another psychiatric disorder was not considered an exclusion criterion. Trials in patients with depression with a concomitant medical ill- Background Tricyclic antidepressants Amitriptyline is one of the first `reference' ness were not included in this review. have similar efficacy and slightly lower tricyclic antidepressants TCAs). Over the past 40 years a number of newer tricyclics, tolerability than selective serotonin Search strategy heterocyclics and selective serotonin re- Relevant studies were located by searching reuptakeinhibitorsreuptake inhibitors SSRIs).However, uptake inhibitors SSRIs) have been intro- the Cochrane Collaboration Depression, there are no systematic reviews assessing duced Garattini et aletal,1998). Despite Anxiety and Neurosis Controlled Trials several large systematic reviews comparing amitriptyline, the reference tricyclic drug, Register CCDANCTR). This specialised tricyclics and SSRIs there is no clear agree- vv. other tricyclics and SSRIs directly. register is regularly updated by electronic ment over first-line treatment of depression Medline,Embase,PsycINFO,LILACS, SongSong et aletal,1993; Anderson & Tomenson, Aims ToreviewTo review the tolerability and Psyndex,CINAHL,SIGLE) and non-electro- 1995; Montgomery & Kasper,1995; efficacy of amitriptyline inthe nicnicliterature searches. The register was HotopfHotopf et aletal,1996; Canadian Coordinating management of depression. searched using the following terms: Office for Health Technology Assessment, AMITRIPTYLIN**AMITRIPTYLIN oror AMITRILAMITRIL oror ELA-ELA- 19971997aa). -
(12) Patent Application Publication (10) Pub. No.: US 2015/0011643 A1 Dilisa Et Al
US 2015 0011643A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2015/0011643 A1 DiLisa et al. (43) Pub. Date: Jan. 8, 2015 (54) TREATMENT OF HEART FAILURE AND (60) Provisional application No. 61/038,230, filed on Mar. ASSOCATED CONDITIONS BY 20, 2008, provisional application No. 61/155,704, ADMINISTRATION OF MONOAMINE filed on Feb. 26, 2009. OXIDASE INHIBITORS (71) Applicants:Nazareno Paolocci, Baltimore, MD Publication Classification (US); Univeristy of Padua, Padova (IT) (51) Int. Cl. (72) Inventors: Fabio DiLisa, Padova (IT): Ning Feng, A63L/38 (2006.01) Baltimore, MD (US); Nina Kaludercic, (52) U.S. Cl. Baltimore, MD (US); Nazareno CPC ..... ... A61 K31/138 (2013.01) Paolocci, Baltimore, MD (US) USPC .......................................................... S14/651 (21) Appl. No.: 14/332,234 (22) Filed: Jul. 15, 2014 (57) ABSTRACT Related U.S. Application Data Administration of monoamine oxidase inhibitors is useful in (63) Continuation of application No. 12/407,739, filed on the prevention and treatment of heart failure and incipient Mar. 19, 2009, now abandoned. heart failure. Patent Application Publication Jan. 8, 2015 Sheet 1 of 2 US 201S/0011643 A1 Figure 1 Sial 8. Sws-L) Cleaved Š Caspase-3 ) Figure . Prevention of caspase-3 productief) fron cardiomyocytes Lapoi) reatment with clorgyi Be. Patent Application Publication Jan. 8, 2015 Sheet 2 of 2 US 201S/0011643 A1 Figure 2 8:38:8 ::::::::8: US 2015/0011643 A1 Jan. 8, 2015 TREATMENT OF HEART FAILURE AND in the art is a variety of MAO inhibitors and their pharmaceu ASSOCATED CONDITIONS BY tically acceptable compositions for administration, in accor ADMINISTRATION OF MONOAMINE dance with the present invention, to mammals including, but OXIDASE INHIBITORS not limited to, humans. -
Attendee Guidelines
(Temple of Eternal Sound) Attendee Guidelines 1. Introduction 2. Practical Guidelines -Preparation -Contraindications -Food -Clothing -Cleansing -During the Session -Suggested Best Practices -Temple Practices & Ritual Norms -Single Sacrament Sanctuary 3. Code of Ethics 4. Dietary Guidelines 5. Medical Information 6. Attendee Waiver Céu do Som Welcome, Thank you for your interest in our Forest Family Circles, Realisation Retreats and Wisdom Works at the Temple of Céu do Som & Abuelatree Sanctuary. You are endeavouring to participate in what, for us, is one of the most profound and meaningful doorways into the mysteries of the Sacred & Profound. The following pages are practical suggestions outlining our expectations, guidelines and safety measures to ensure harmony for you, for our work and for our community. We seek to uphold a high standard in regards to the safe space of transformation and realisation that may create a positive impact through healing and integration of our participants. The guidelines in this booklet all serve a direct purpose. We ask that each one be approached with due respect. It is not necessary to subscribe to our points of view in order to receive the sacrament. We do not discriminate and find that ultimately it is up to the individual to discover what is true for them. Así Céu do Som PRACTICAL GUIDELINES Preparation for the spiritual study Contraindications (refer to Medical Information section for more details) 1. If you are uncertain about any contraindications or factors please ask. 2. If you have any personal concerns a meeting can be arranged prior in order to discuss. 3. If you are taking any prescription medication, namely antidepressants, antipsychotics or SSRI's please speak to us (Refer to Medical Information section). -

Treatment Resistant Depression Clinic Clinician Referral Form
Treatment Resistant Depression Clinic Clinician Referral Form Patient Date: Name: Contact DOB: Sex: No: Ref. By: Contact: **Treating Contact: Psychiatrist: Primary Please Include Copy of Patient’s Insurance Insurance Card (Front and Back) Provider: PSYCHIATRIC NOTES How long have you known this patient? Current Diagnosis/Diagnoses: Current/Target Symptoms Past History of ECT □NO □YES If YES, # of sessions: Type: □UL □BF □BT Dates: Past response: □excellent □good □fair □poor □unknown Past History of TMS □NO □YES If YES, # of sessions: Dates: Past response: □excellent □good □fair □poor □unknown Current Medications: Current Medical Problems Emory Treatment Resistant Depression Clinic Clinician Referral Form 10/07/15 Allergies Do we have permission to contact the patient? □NO □YES ADDITIONAL NOTES Clinical Impression : Please complete the attached medication history form Include a copy of the patient’s insurance card (front and back) Fax referral form to: 404 712 7436. Attn: Emory TRD Clinic If you have any questions, please contact: Taelar Johnson at 404 712 8732 Emory Treatment Resistant Depression Clinic Clinician Referral Form 10/07/15 Generic Date drug How many weeks drug Drug Class Name was tried Min. Dose Max Dose Dosage was taken? Was it helpful?/Side Effects TCA Adapin Doxepin 150mg/d 250mg/d Anafranil Clomipramine 150mg/d 250mg/d Asendin Amoxapine 150mg/d 250mg/d Endep/Elavil Amitriptyline 150mg/d 250mg/d Ludiomil Maprotiline 150mg/d 250mg/d Norpramin Desipramine 150mg/d 250mg/d Pamelor Nortyrptiline 75mg/d 125mg/d Sinequin Doxepin -

1 Supplemental Figure 1: Illustration of Time-Varying
Supplemental Material Table of Contents Supplemental Table 1: List of classes and medications. Supplemental Table 2: Association between benzodiazepines and mortality in patients initiating hemodialysis (n=69,368) between 2013‐2014 stratified by age, sex, race, and opioid co‐dispensing. Supplemental Figure 1: Illustration of time‐varying exposure to benzodiazepine or opioid claims for one person. Several sensitivity analyses were performed wherein person‐day exposure was extended to +7 days, +14 days, and +28 days beyond the outlined periods above. 1 Supplemental Table 1: List of classes and medications. Class Medications Short‐acting benzodiazepines Alprazolam, estazolam, lorazepam, midazolam, oxazepam, temazepam, and triazolam Long‐acting benzodiazepines chlordiazepoxide, clobazam, clonazepam, clorazepate, diazepam, flurazepam Opioids alfentanil, buprenorphine, butorphanol, codeine, dihydrocodeine, fentanyl, hydrocodone, hydromorphine, meperidine, methadone, morphine, nalbuphine, nucynta, oxycodone, oxymorphone, pentazocine, propoxyphene, remifentanil, sufentanil, tapentadol, talwin, tramadol, carfentanil, pethidine, and etorphine Antidepressants citalopram, escitalopram, fluoxetine, fluvozamine, paroxetine, sertraline; desvenlafaxine, duloxetine, levomilnacipran, milnacipran, venlafaxine; vilazodone, vortioxetine; nefazodone, trazodone; atomoxetine, reboxetine, teniloxazine, viloxazine; bupropion; amitriptyline, amitriptylinoxide, clomipramine, desipramine, dibenzepin, dimetacrine, dosulepin, doxepin, imipramine, lofepramine, melitracen, -

Info on Skin Testing
Information on Skin Testing *Please review 1 week prior to testing* Your Doctor has ordered an allergy test for you. Your appointment has been made for: ___________________________________ at _______________________AM/PM at our (date) (time) _ Foulkstone / Limestone / Glasgow _ office. Skin tests are a method of testing for allergic reactions to substances, or allergens, in the environment. Our practice utilizes a test that involves no needles! We use a prick method which involves a series of small plastic applicators that carry a specific antigen which is placed on your arms. The types of allergens we test for include weeds, trees, grasses, molds, animal dander, dust mites and some foods. The testing will take 45 minutes. Please remember to wear comfortable clothing with short sleeves. Reactions can consist of itchy eyes, nose or throat, nasal congestion, runny nose, tightness in the throat or chest, wheezing, lightheadedness, hives or anaphylactic shock. Although this is very rare, our staff is fully prepared with emergency equipment and a physician is always on site. To ensure accurate testing results, certain medicines should be stopped 5 days prior to testing, although you should not stop medicines without talking to your prescribing physician. Medications that interfere with testing include but are not limited to: Antihistamines are medicines used to treat allergies, nausea, and dizziness. Many are found in over the counter cold medicines. They include, but are not limited to: ALAVERT / CLARITIN (LORATIDINE) DRAMAMINE (DIMENHYDRINATE) -

Mikocka-Walus Et Al-2017
This is a repository copy of Adjuvant therapy with antidepressants for the management of inflammatory bowel disease (Protocol). White Rose Research Online URL for this paper: https://eprints.whiterose.ac.uk/118724/ Version: Published Version Article: Mikocka-Walus, Antonina Anna orcid.org/0000-0003-4864-3956, Fielder, Andrea, Prady, Stephanie Louise orcid.org/0000-0002-8933-8045 et al. (3 more authors) (2017) Adjuvant therapy with antidepressants for the management of inflammatory bowel disease (Protocol). Cochrane Database of Systematic Reviews. ISSN 1469-493X https://doi.org/10.1002/14651858.CD012680 Reuse Items deposited in White Rose Research Online are protected by copyright, with all rights reserved unless indicated otherwise. They may be downloaded and/or printed for private study, or other acts as permitted by national copyright laws. The publisher or other rights holders may allow further reproduction and re-use of the full text version. This is indicated by the licence information on the White Rose Research Online record for the item. Takedown If you consider content in White Rose Research Online to be in breach of UK law, please notify us by emailing [email protected] including the URL of the record and the reason for the withdrawal request. [email protected] https://eprints.whiterose.ac.uk/ Cochrane Database of Systematic Reviews Adjuvant therapy with antidepressants for the management of inflammatory bowel disease (Protocol) Mikocka-Walus A, Fielder A, Prady SL, Esterman AJ, Knowles S, Andrews JM Mikocka-Walus A, Fielder A, Prady SL, Esterman AJ, Knowles S, Andrews JM. Adjuvant therapy with antidepressants for the management of inflammatory bowel disease. -

Federal Register / Vol. 60, No. 80 / Wednesday, April 26, 1995 / Notices DIX to the HTSUS—Continued
20558 Federal Register / Vol. 60, No. 80 / Wednesday, April 26, 1995 / Notices DEPARMENT OF THE TREASURY Services, U.S. Customs Service, 1301 TABLE 1.ÐPHARMACEUTICAL APPEN- Constitution Avenue NW, Washington, DIX TO THE HTSUSÐContinued Customs Service D.C. 20229 at (202) 927±1060. CAS No. Pharmaceutical [T.D. 95±33] Dated: April 14, 1995. 52±78±8 ..................... NORETHANDROLONE. A. W. Tennant, 52±86±8 ..................... HALOPERIDOL. Pharmaceutical Tables 1 and 3 of the Director, Office of Laboratories and Scientific 52±88±0 ..................... ATROPINE METHONITRATE. HTSUS 52±90±4 ..................... CYSTEINE. Services. 53±03±2 ..................... PREDNISONE. 53±06±5 ..................... CORTISONE. AGENCY: Customs Service, Department TABLE 1.ÐPHARMACEUTICAL 53±10±1 ..................... HYDROXYDIONE SODIUM SUCCI- of the Treasury. NATE. APPENDIX TO THE HTSUS 53±16±7 ..................... ESTRONE. ACTION: Listing of the products found in 53±18±9 ..................... BIETASERPINE. Table 1 and Table 3 of the CAS No. Pharmaceutical 53±19±0 ..................... MITOTANE. 53±31±6 ..................... MEDIBAZINE. Pharmaceutical Appendix to the N/A ............................. ACTAGARDIN. 53±33±8 ..................... PARAMETHASONE. Harmonized Tariff Schedule of the N/A ............................. ARDACIN. 53±34±9 ..................... FLUPREDNISOLONE. N/A ............................. BICIROMAB. 53±39±4 ..................... OXANDROLONE. United States of America in Chemical N/A ............................. CELUCLORAL. 53±43±0