RESEARCH BMJ: First Published As 10.1136/Bmj.C1241 on 23 March 2010
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Meta Analysis of County, Gender, and Year Specific Effects of Active Labour Market Programmes
A Meta Analysis of County, Gender, and Year Speci…c E¤ects of Active Labour Market Programmes Agne Lauzadyte Department of Economics, University of Aarhus E-Mail: [email protected] and Michael Rosholm Department of Economics, Aarhus School of Business E-Mail: [email protected] 1 1. Introduction Unemployment was high in Denmark during the 1980s and 90s, reaching a record level of 12.3% in 1994. Consequently, there was a perceived need for new actions and policies in the combat of unemployment, and a law Active Labour Market Policies (ALMPs) was enacted in 1994. The instated policy marked a dramatic regime change in the intensity of active labour market policies. After the reform, unemployment has decreased signi…cantly –in 1998 the unemploy- ment rate was 6.6% and in 2002 it was 5.2%. TABLE 1. UNEMPLOYMENT IN DANISH COUNTIES (EXCL. BORNHOLM) IN 1990 - 2004, % 1990 1992 1994 1996 1998 2000 2002 2004 Country 9,7 11,3 12,3 8,9 6,6 5,4 5,2 6,4 Copenhagen and Frederiksberg 12,3 14,9 16 12,8 8,8 5,7 5,8 6,9 Copenhagen county 6,9 9,2 10,6 7,9 5,6 4,2 4,1 5,3 Frederiksborg county 6,6 8,4 9,7 6,9 4,8 3,7 3,7 4,5 Roskilde county 7 8,8 9,7 7,2 4,9 3,8 3,8 4,6 Western Zelland county 10,9 12 13 9,3 6,8 5,6 5,2 6,7 Storstrøms county 11,5 12,8 14,3 10,6 8,3 6,6 6,2 6,6 Funen county 11,1 12,7 14,1 8,9 6,7 6,5 6 7,3 Southern Jutland county 9,6 10,6 10,8 7,2 5,4 5,2 5,3 6,4 Ribe county 9 9,9 9,9 7 5,2 4,6 4,5 5,2 Vejle county 9,2 10,7 11,3 7,6 6 4,8 4,9 6,1 Ringkøbing county 7,7 8,4 8,8 6,4 4,8 4,1 4,1 5,3 Århus county 10,5 12 12,8 9,3 7,2 6,2 6 7,1 Viborg county 8,6 9,5 9,6 7,2 5,1 4,6 4,3 4,9 Northern Jutland county 12,9 14,5 15,1 10,7 8,1 7,2 6,8 8,7 Source: www.statistikbanken.dk However, the unemployment rates and their evolution over time di¤er be- tween Danish counties, see Table 1. -
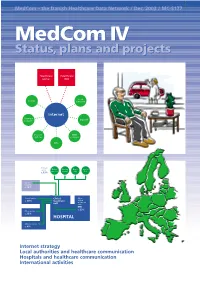
Medcom IV Status, Plans and Projects
MedCom – the Danish Healthcare Data Network / Dec. 2003 / MC-S177 MedComMedCom IV IV Status,Status, plans plans andand projectsprojects Healthcare Healthcare portal DIX Local County authority Internet Pharmacy Dan Net network Doctors’ KMD systems network KPLL Primary sector Medical Nursing Home Specia- practice homes care lists c. 13% Other hospitals c. 10% Clinical service Clinical Other c. 40% treatment clinical treatment unit units EPR c. 23% Other service c. 13% HOSPITAL Administration c. 4% ● Internet strategy ● Local authorities and healthcare communication ● Hospitals and healthcare communication ● International activities 2 MedCom IV – status, plans and projects Contents Aims of MedCom 2 The local authorities and healthcare communication 20 Introduction 3 The Hospital-Local Authority XML project 20 Healthcare on the move 3 The Hospital-Local Authority project and Common Language 22 History 4 Commentary: The Minister of Social Affairs, Henriette Kjær 22 The MedCom steering group 6 The LÆ form project 23 Commentary: The Minister of the Interior and Commentary: The Chairman of the National Health, Lars Løkke Rasmussen 7 Association of Local Authorities, Perspective: MedCom certifies communication 8 Ejgil W. Rasmussen 24 Perspective: The IT Lighthouse’s local authority- The Internet strategy 9 medical practice communication 24 The infrastructure project 9 The hospitals and Commentary: The Chairman of the Association of healthcare communication 25 County Councils, Kristian Ebbensgaard 12 Perspective: The Internet strategy and the From -

Jens Galschiot Portrait of a Sculptor
Jens Galschiot Portrait of a sculptor www.galschiot.com Index About Jens Galschiot 5 Balancing act (2005-14) 38 Art In Defence Of Humanism 6 The Little Matchstick Girl (2005) 38 My Inner Beast (1993) 10 The Golden Calf (2005) 39 The Silent Dead (1995) 12 The Nightmare (2002) 40 The Pillar of Shame (1997-??.) 14 In the Name of God (2006) 42 The Earth is Poisonous (1997) 18 The Color Orange (2008) 45 Young People in Glass Tubes (1997) 20 Seven Meters (2009) 46 Fear Eats Up Souls (1998) 21 Ending Homelessness (2010) 48 The Messenger (2000) 22 The Refugee Ship (2010) 50 Hands of Stone (2000) 24 Fundamentalism (2013) 52 NGO Gathering in Prague(2000) 25 Unbearable (2015) 54 The Tenth Plague (2001) 26 Polar Bear Army (2015) 54 Just do it (2001) 28 550+1 (2015) 55 The Hunger March. (2002) 29 Major Projects/Sculpture groups Freedom to Pollute (2002) 30 Cocoon 57 Survival of the Fattest (2002) 32 The Occult Temple 58 European Social Forum (2003-2008) 34 The Utmost Silence 58 Mad Cow Disease (2005) 36 The Little Prince 59 2 Ornamentation of a Nursery Garden 60 Clothing Sculptures 67 Civilization 60 Miscellaneous Sculptures 69 Why Me? 60 Commissioned work 69 The Fiery Soul 61 Works for awards 70 Catwings 61 Concepts of future projects 71 The Bella Center 61 Review of exhibitions 73 Justitia 62 Exhibition in Denmark 73 From Duckling to Swan 62 Permanent or recurring exhibitions 75 The Asian Pavilion 63 Exhibition Abroad 75 The Storyteller‟s Fountain 64 Events in the gallery 76 Hans Christian Andersen 65 Member of/Participating in 77 Historical Traces - Dock Worker Monument 66 Support from Foundations, Companies, etc. -

Medcom 2 in Print (Pdf)
MedCom MC-S117 / December 1999 -the Danish Health Care Data Network MedCom2MedCom2 inin print print Ministry of Health Ministry of Social Affairs The National Board of Health Association of County Councils in Denmark The National Association of Local Authorities in Denmark Copenhagen Hospital Corporation Copenhagen and Frederiksberg Local Authorities Danish Pharmaceutical Association Danish Dental Association Association of Danish Doctors Kommunedata Tele Danmark Dan Net The MedCom project A nation-wide network and EPR implementation, which takes place in the hospitals. MedCom is a project involving co- operation between authorities, The parties behind the permanent healthcare organisations and priv- MedCom are the Ministry of ate companies linked to the health- Health, the Association of County care sector. The purpose behind Councils in Denmark, the National this co-operation is to establish and Board of Health, Copenhagen MedCom 1 (1994 - 96) continue the development of a Hospital Corporation, Copenhagen had the purpose of coherent Danish healthcare data and Frederiksberg Local Authori- G developing communication stan- network. ties, the Danish Pharmaceutical dards for the most common com- Association, the Association of munication flows between medical MedCom is to contribute towards Danish Doctors and Dan Net. practices, hospitals and pharmacies. implementing the Danish Govern- ment’s IT policy action plan for the MedCom 1, 2 and 3 MedCom 2 (1997 - 99) healthcare sector, including conti- MedCom activities are carried out had the purpose of nuing the dissemination and quali- as projects for defined periods of G developing communication stan- ty assurance of electronic commu- time, and each project period con- dards for the most common com- nication. -

Syddansk Universitet Ulykker 2003: Tilskadekomne Registreret På Skadestuen, Odense Universitetshospital Larsen, Lars Binderup
Syddansk Universitet Ulykker 2003: Tilskadekomne registreret på skadestuen, Odense Universitetshospital Larsen, Lars Binderup; Larsen, Morten Schultz; Lauritsen, Jens M Publication date: 2004 Document version Forlagets udgivne version Document license CC BY-NC Citation for pulished version (APA): Larsen, L. B., Larsen, M. S., & Lauritsen, J. (red.) (2004). Ulykker 2003: Tilskadekomne registreret på skadestuen, Odense Universitetshospital. (Årsrapporter: Tilskadekomne registreret på skadestuen, Odense Universitetshospital). General rights Copyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights. • Users may download and print one copy of any publication from the public portal for the purpose of private study or research. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying the publication in the public portal ? Take down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Download date: 19. Apr. 2017 Ulykker 2003 Tilskadekomne registreret på skadestuen, Odense Universitetshospital Accident victims treated at the A & E department, Odense University Hospital Inklusive nøgletal for henvendelser til skadestuerne i Middelfart og Svendborg Key figures of contacts to the A & E departments in Middelfart and Svendborg included UlykkesAnalyseGruppen Accident Analysis Group Ulykker 2003 Tilskadekomne registreret på skadestuen, Odense Universitetshospital Redigeret af Lars Binderup Larsen, Morten Schultz Larsen og Jens M. -

In the Workshop Presentation Anne Smetana Will Be Dealing With
Title : Model Project Children, Food and Activity. Author (s) : Anne Smetana, Deputy Office Manager, County of Funen Morten Kromann Nielsen, Project Coordinator, County of Funen E-mail : [email protected] Organisation : Department of Prevention and Health, Funen County, Ørbækvej 100, DK-5220 Odense SØ, Denmark. Tel: +45 6556 1209, Fax +45 6556 1205 Homepage : www.boernmadbevaegelse.dk The model project Children, Food and Activity is a cooperative project between the County of Funen and 10 municipalities (boroughs), the Danish Ministry of the Interior and Health, The National Board of Health, Aarhus School of Architecture and The County Centre for Education. The project began in August 2002, ended its first phase in January 2005, and has been extended to other municipalities in the county. The project has been evaluated by the National Institute of Public Health. The main aim is to enhance the well being and health, and prevent illness among children between 3 and 10 years of age through a number of precise and measurable goals: • To develop food and activity policies; • To enhance knowledge and action competence of professionals and children; • To involve parents and families; • To create social and physical environments that promotes healthy choices; • To ensure that children’s eating and activity habits meet the official the recommendations The core activity of the project is consultancy assistance for the development and implementation of policies and an educational programme on food and physical activity directed at professionals working with children in institutional contexts. These activities focus on the social and cultural framing of health behaviour of children by creating an attractive and inclusive culture of health i.e. -

Regional Environmental Accounts Denmark 2003
Regional Environmental Accounts Denmark 2003 Peter Rørmose Jensen Thomas Olsen This report has benefited from funding by the European Commission, GD Environment, by means to the grant agreement no. 200471401007, action 3 for the study entitled "Environmental Statistics and Accounts – Regional Environmental Accounts”. Regional environmental accounts Denmark 2003 Statistics Denmark December 2005 Contact information: Peter Rørmose Jensen Head of section National Accounts - Environmental Accounts and Input-Output Statistics Denmark Sejrogade 11 DK-2100 Phone: +45 3917 3917 Direct: +45 3917 3862 E-mail: [email protected] Thomas Olsen Head of section National Accounts - Environmental Accounts and Input-Output Statistics Denmark Sejrogade 11 DK-2100 Phone: +45 3917 3917 Direct: +45 3917 3828 E-mail: [email protected] Table of contents 1 INTRODUCTION................................................................................................................... 2 1.1 Regions in Denmark............................................................................................................. 2 2 REGIONAL ENERGY ACCOUNTS........................................................................................... 5 2.1 Data sources for energy accounts ......................................................................................... 7 2.1.1 Census on the use of energy in manufacturing industries ..........................................................8 2.1.2 Census on energy producers...................................................................................................10 -

Wild Bird H5N1 Outbreaks
Wild bird H5N1 Outbreaks 4 Aug 2006 BirdLife International Wellbrook Court Girton Road Cambridge CB3 0NA U.K. 1 Contents 1 KEY...................................................................................................................................................... 5 2 ALBANIA............................................................................................................................................ 5 3 AFGHANISTAN................................................................................................................................. 5 4 AUSTRIA ............................................................................................................................................ 5 5 AZERBAIJAN .................................................................................................................................... 6 6 BELGIUM ........................................................................................................................................... 7 7 BOSNIA-HERZEGOVINA................................................................................................................ 7 8 BURKINA FASO................................................................................................................................ 7 9 BULGARIA......................................................................................................................................... 7 10 CAMBODIA....................................................................................................................................... -

Restoration of Raised Bogs in Denmark Using New Methods – a LIFE Nature Project Layman’S Report Text Jesper Stenild
Restoration of raised bogs in Denmark using new methods – a LIFE Nature project Layman’s report Text Jesper Stenild Editing Jesper Stenild, Annita Svendsen and Søren Kjær Photography The Danish Nature Agency, Jydsk Luftfoto, Thomas Eske Holm (www.fugleognatur.dk) Aerial photo, front page Store Økssø viewed from the southeast. Photograph: Jydsk Luftfoto Illustration page 9 Niels Bach Graphic design Glindvad Grafisk Design MILJØM K Æ S R I K Printed by D N R I N O G N Scanprint. 1,000 copies printed on paper bearing the Nordic Swan ecolabel. 541 006 ISBN 978-87-7279-261-3 This “layman’s report” forms part of the reporting of the LIFE Nature project RERABOG. The purpose of the project is to restore raised bogs in 7 project areas and to develop and disseminate methods for the restoration of raised bogs in a Danish context. The project period ran from 2005 to 2011. In 2005-2006, the project was run as a collaboration between Viborg County, Vejle County, Southern Jutland County, Funen County and the Danish Nature Agency. The project was continued and brought to an end by the Danish Nature Agency. Restoration of raised bogs in Denmark using new methods Layman’s report Boest Mose. The raised bog – an endangered natural habitat From prehistoric right up to historical times, raised bogs were rity natural habitats protected by the EU’s Habitats Directive and one of Denmark’s commonest types of bog. They were most included in the European network of protected natural habitats widespread in Jutland, but they were also to be found in eastern known as Natura 2000. -
Jutland-Funen, Denmark
OECD/IMHE project Supporting the Contribution of Higher Education Institutions to Regional Development Self-Evaluation Report: Jutland-Funen, Denmark Søren Kerndrup March 2006 0. INTRODUCTION 5 1. OVERVIEW OF THE REGION 7 1.1. The Jutland-Funen Co-operation of Business Development 7 1.2. Geographical situation 7 1.3. Demographic situation 8 1.3.1. Population growth 8 1.4. The economic and social situation in Jutland-Funen 9 1.4.1. Education 9 1.4.2. Personal income 10 1.4.3 Employment 10 1.5. Occupational structure 10 1.5.1. Resource area geographical specialization 11 1.6. Research and development in the public and private sectors 14 1.6.1. Innovation 15 1.6.2. The interaction between knowledge institutions and local industries 15 1.6.3. Use of highly qualified labour force 15 1.6.4. Knowledge based entrepreneurs 15 1.7. The Danish system of government 16 1.7.1. Public sector financing in Denmark 16 1.7.2. Distribution of public sector services in Denmark 16 1.7.3. Distribution of health services 17 1.7.4. Distribution of responsibilities in relation to the promotion of industry and economic development 17 1.7.5. The distribution of responsibilities for educational services 18 1.7.6. Responsibilities for cultural initiatives 20 1.7.7. Financing of the educational system in Denmark 21 1.7.8. Regional influence on higher education and research 22 1.7.9. The Jutland-Funen Co-operation of Business Development 22 1.7.10. The Science and Enterprise Network 22 2. -
Support for Growth
Support for Growth > > > Objective 2 aid from the European Union to regions of Denmark with a particular need to strengthen development and growth > > > Authors: National Agency for Enterprise and Housing | National Labour Market Authority | Regional Municipality of Bornholm | Funen County | Storstrøm County | North Jutland County | Ringkjøbing County | South Jutland County | Viborg County | Århus County | Contents 4 Objective 2 – Briefly and to the Point 8 Regional Municipality of Bornholm 10 Funen County 12 Storstrøm County 14 North Jutland County 16 Ringkjøbing County 18 South Jutland County 20 Viborg County 22 Århus County Good results already – and many more under way The Objective 2 Programme for Denmark took effect in 2000. Since then, a large number of projects have been initiated based on assistance from the EU programme, which is intended to generate development and growth in areas with particular needs for new activities. The effects of this financial shot-in-the-arm are starting to appear throughout the areas in Denmark covered by the Objective 2 Programme. New jobs are being created, existing ones are being kept, the qualifications of managers and employees are being enhanced and the areas are becoming increasingly attractive to settle in or visit. This booklet provides an introduction to the aid offered by the Objective 2 Programme, i.e., the overall framework for Objective 2 projects, the application procedures and more. At the same time, the booklet provides insight into the actual implementation of the Objective 2 Programme with specific examples from the various Danish regions. The efforts up to year end 2002 are appraised, and the booklet includes information on the remaining, available Objective 2 funds. -

Det Samfundsvidenskabelige Fakultet
DET SAMFUNDSVIDENSKABELIGE FAKULTET Liste over tilhørende institutter Institut for Forskning og Udvikling i Landdistrikter Institut for Grænseregionsforskning Institut for Miljø- og Erhvervsøkonomi Institut for Marketing & Management Institut for Virksomhedsledelse & Økonomi Institut for Entreprenørskab og Relationsledelse Institut for Maritim Forskning og Innovation Institut for Statskundskab Juridisk Institut Forskningscentre: Center for Småvirksomhedsforskning (CESFO) Centre for Fisheries & Aquaculture Management & Economics (FAME) Centre for European Studies Tværfakultære institutter og centre: Center for Journalistik Centre for Tourism, Innovation and Culture (TIC) Institut for Sundhedstjenesteforskning Center for Velfærdsstatsforskning Center for Anvendt Sundhedstjenesteforskning og Teknologivurdering (CAST) Den Samfundsvidenskabelige Sektion af Mads Clausens Instituttet Oversigt over administrative medarbejdere ved fakultetet Dekan, Nis Jul Clausen Fakultetssekretær, Klaus Hollmann Fuldmægtig, Helle Damgaard Boeriths Fuldmægtig, Tanja Helskov Hansen (barselsorlov indtil 6. februar) Kontorfuldmægtig, Alice Borbély Kontorfunktionær, Vibeke Ølund Overassistent, Lena Haslestad Jeppesen Overassistent, Dorte Cohrt Nebel Overassistent Mette Fuglsig (orlov indtil 1. juni) Overassistent, Pernille Saaby Korrespondent, Charlotte Pilgaard Møller Assistent, Pia Vang (fratrådt 31. august) Assistent, Merete Pedersen (fratrådt 15. marts) Assistent, Stine Christensen (fratrådt 1. februar) Assistent, Joan Nielsen EDB-organistion: Fuldmægtig, Jan