Syria's Displaced Health Workforce: Policy Opportunities and Challenges
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

National Coordination Meeting
National Coordination Meeting Kyiv, 20 January 2021 Business of the Day 1. Q&A on Health Reform. Guest speakers: • Dr. Elina Dale, Adviser on Health Policy at WHO Ukraine • Anastasiya Brylova, Officer on Service Delivery, WHO Ukraine 2. Health Cluster Calendar 2021 3. Situation update: COVID-19 and ECA - WHO & partners 4. Update on Public Health Situation Analysis (PHSA) and ongoing assessments 5. Health Cluster M&E Framework 6. AOB • Update on Q4 2020 HRP and COVID-19 reporting • Update on COVID-19 Distribution Planning Tool (4W) • Health Cluster Assessment Database Health Cluster Meeting Q&A on Health Reform in Ukraine Dr. Elina Dale, Adviser on Health Policy Anastasiya Brylova , Officer on Service Delivery WHO Ukraine 2. HС Calendar Q1 & Q2 2021 # Month Date Q&A topics (TBC) 1 January 20 Health reform HeRAMS, Attacks on Health 2 February 3 Facilities 3 February 17 IPC & WASH 4 March 3 MHPSS 5 March 17 HIV/TB 6 April 14 Laboratories 7 April 28 Field focus: GCA & NGCA 8 May 12 Post COVID Rehab Human Rights/Protection and 9 May 26 Health 10 June 2 Epi and Surveillance 11 June 9 Behavioral Insights 12 June 16 Comms in Health 4. Public Health Situation Analysis (PHSA) • PHSA is part of the Public Health Information Services (PHIS) tools of the Global Health Cluster. • Provides all health sector partners with a common and comprehensive understanding of the public health situation in a crisis in order to inform evidence-based collective humanitarian health response planning. Focus of the assessment: Donetska & Luhanska Oblasts Eastern Ukraine -
![English.Pdf Purchasing Power Parity [PPP])—Much Lower Than 2 World Bank](https://docslib.b-cdn.net/cover/2888/english-pdf-purchasing-power-parity-ppp-much-lower-than-2-world-bank-1082888.webp)
English.Pdf Purchasing Power Parity [PPP])—Much Lower Than 2 World Bank
CENTRAL Public Disclosure Authorized AFRICAN REPUBLIC ECONOMIC Public Disclosure Authorized UPDATE FOURTH EDITION Investing in Public Disclosure Authorized Human Capital to Protect the Future JULY 2021 Public Disclosure Authorized © 2021 The World Bank 1818 H Street NW, Washington DC 20433 Telephone: 202-473-1000; Internet: www.worldbank.org Some rights reserved This work is a product of the staff of The World Bank. The findings, interpretations, and conclusions expressed in this work do not necessarily reflect the views of the Executive Directors of The World Bank or the governments they represent. The World Bank does not guarantee the accuracy of the data included in this work. The boundaries, colors, denominations, and other information shown on any map in this work do not imply any judgment on the part of The World Bank concerning the legal status of any territory or the endorsement or acceptance of such boundaries. Rights and Permissions The material in this work is subject to copyright. Because The World Bank encourages dissemination of its knowledge, this work may be reproduced, in whole or in part, for noncommercial purposes as long as full attribution to this work is given. Attribution—Please cite the work as follows: “World Bank. 2021. Central African Republic Economic Update: Investing in Human Capital to Protect the Future. © World Bank.” All queries on rights and licenses, including subsidiary rights, should be addressed to World Bank Publications, The World Bank Group, 1818 H Street NW, Washington, DC 20433, USA; fax: 202-522-2625; -
Assessments of Health Services Availability in Humanitarian Emergencies: a Review of Assessments in Haiti and Sudan Using a Health Systems Approach Jason W
Nickerson et al. Conflict and Health (2015) 9:20 DOI 10.1186/s13031-015-0045-6 RESEARCH ARTICLE Open Access Assessments of health services availability in humanitarian emergencies: a review of assessments in Haiti and Sudan using a health systems approach Jason W. Nickerson1,2,3*, Janet Hatcher-Roberts3, Orvill Adams4, Amir Attaran5 and Peter Tugwell3,6 Abstract Background: Assessing the availability of health services during humanitarian emergencies is essential for understanding the capacities and weaknesses of disrupted health systems. To improve the consistency of health facilities assessments, the World Health Organization has proposed the use of the Health Resources Availability Mapping System (HeRAMS) developed in Darfur, Sudan as a standardized assessment tool for use in future acute and protracted crises. This study provides an evaluation of HeRAMS’ comprehensiveness, and investigates the methods, quality and comprehensiveness of health facilities data and tools in Haiti, where HeRAMS was not used. Methods and findings: Tools and databases containing health facilities data in Haiti were collected using a snowball sampling technique, while HeRAMS was purposefully evaluated in Sudan. All collected tools were assessed for quality and comprehensiveness using a coding scheme based on the World Health Organization’s health systems building blocks, the Global Health Cluster Suggested Set of Core Indicators and Benchmarks by Category, and the Sphere Humanitarian Charter and Minimum Standards in Humanitarian Response. Eight assessments and databases were located in Haiti, and covered a median of 3.5 of the 6 health system building blocks, 4.5 of the 14 Sphere standards, and 2 of the 9 Health Cluster indicators. -

Humanitarian Needs Overview Iraq Issued November 2019
HUMANITARIAN HUMANITARIAN PROGRAMME CYCLE 2020 NEEDS OVERVIEW ISSUED NOVEMBER 2019 IRAQ 1 HUMANITARIAN NEEDS OVERVIEW 2020 About Get the latest updates This document has been consolidated by OCHA on behalf of the Humanitarian OCHA coordinates humanitarian action to ensure Country Team and partners. It provides a shared understanding of the crisis, crisis-affected people receive the assistance and protection they need. It works to overcome obstacles including the most pressing humanitarian needs and the estimated number of that impede humanitarian assistance from reaching people who need assistance. It represents a consolidated evidence base and helps people affected by crises, and provides leadership in inform joint strategic response planning. mobilizing assistance and resources on behalf of the The designations employed and the presentation of material in the report do not imply humanitarian system. the expression of any opinion whatsoever on the part of the Secretariat of the United www.unocha.org/iraq Nations concerning the legal status of any country, territory, city or area or of its www.twitter.com/ochairaq authorities, or concerning the delimitation of its frontiers or boundaries. PHOTO ON COVER Meeting with women displaced by flooding in April 2019, Maysan, © A Lazau-Ratz, OCHA Humanitarian Response aims to be the central website for Information Management tools and services, enabling information exchange between clusters and IASC members operating within a protracted or sudden onset crisis. www.humanitarianresponse.info/iraq Humanitarian InSight supports decision-makers by giving them access to key humanitarian data. It provides the latest verified information on needs and delivery of the humanitarian response as well as financial contributions. -
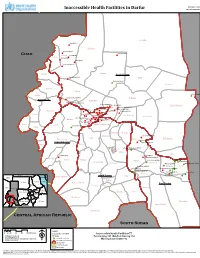
Inaccessible Health Facilities in Darfur Map Ref.:2014-0002
WHO-HISU-SUDAN Inaccessible Health Facilities in Darfur Map Ref.:2014-0002 El Malha Boba(BHU) ! Um Buru Gasimba(BHU) Chad ! Karnoi(PHCC) Kornoi Kamu(BHU) ! ! El Tina Hilaliya(BHU) ! Miski(BHU) ! Ed El Kheir(BHU) ! Kutum Kulbus North Darfur Abu Gamra(BHU) ! Mellit Hashaba(PHCC) ! El Kuma Jebel Moon El Sireaf El Naim(BHU) Sirba ! Umjarwa Asani(BHU) ! El Fasher West Darfur Kebkabiya Melesah(BHU) Korgol(BHU) Saraf Om!ra ! Tina South(BHU) !Tina West(BHU) Umm Keddada !Tawilla !Koshiny North(BHU) Nobo(BHU) Mali(BHU) ! !Khezan Tonjur(BHU) Kereinik ! Rokoro Finga(BHU) Tukumare(BHU) Taibon(B!HU)!Daia!(BHU)! ! El Geneina Samonga(BHU) !!!Solow(BHU) ! Bouri(BHU) Dar El Salam ! ! Klaimendo Um Haraz(BHU) !!Kerbi(BHU) Mara(BH!U) ! Zalingei ! ! Kroun(BH!U)Tagal(BHU) Martagalo(BHU)Baringo(BHU) ! Beida Azum Nertiti Sharq Jabel Marra Urukum(PHCC) Habila ! Marshang Niteaga Alwehda Um Shugeira(BHU) Kass ! Wadi Salih Sheiria El Taweisha Art!u(BHU) Central Darfur ! Abu dangal(BHU) Foro Baranga Shattai Labado(PHCC)Labado(BHU) Nyala North ! Nyala Bielel Ailliet Kubuk(PHCC) Angabu(BHU) ! ! !Almatawrat(BHU) Bindisi Alnayra(BHU) Mukjar Kubum Yassin Kelekle west(BHU) ! ! Ed El Fursan ! !Altaalba(BHU) El Salam Ed Daein Alkhitma(BHU) Wadjoda(Mob_clinic) ! ! Umelkhairat(BHU) Abu Karinka Adila ! Um Boim(BHU) Daralsalam(BHU)Hilal!(BHU) ! Keleikle mugu(BHU) ! ! ! Um Rak!uba(BHU) Sharif(BHU) Assalaya ! Al Gura(BH!U) Um totahana(BHU) Egypt South Darfur ! Umm Dukhun Gerida Libya Saudi Arabia Red Sea Tullus Northern Red Sea Rahad El Berdi East Darfur Nile Katayla Dimsu Chad -

Northeast Nigeria Response BORNO State Health Sector Bulletin
BORNO STATE GOVERNMENT UNICEF’s C4D teams conducted trainings on meningitis social mobilization (Photo: UNICEF) Northeast Nigeria Response BORNO State Health Sector Bulletin #24 16th to 30th April 2017 6.9 MILLION 5.9 MILLION 1,428,947* PEOPLE IN NEED OF TARGET BY THE HEALTH 1,976,644 IDPS IN HEALTH CARE IN; SECTOR; ADAMAWA, POLIO VACCINATED CHILDREN ADAMAWA, BORNO AND BORNO AND YOBE BORNO STATE YOBE STATES STATES HIGHLIGHTS HEALTH SECTOR The Borno State Ministry of Health (SMoH)’s Rapid Response Team 21 HEALTH SECTOR PARTNERS (RRT) mechanism has been re-activated under the umbrella of the Health Sector Coordination, and with the support of WHO, UNICEF HEALTH FACILITIES** and partners. The mechanism aims to respond to the looming threat 288 of Cerebro-Spinal Meningitis (CSM) epidemic that has already FUNCTIONING** (OF TOTAL 749 affected at least five states in Nigeria. A series of trainings for ASSESSED HEALTH FACILITIES) clinicians, nurses and laboratory scientists of secondary health-care 262 FULLY DESTROYED facilities is taken place in Maiduguri and Biu LGAs in Borno State. 215 PARTIALLY DAMAGED Health sector is supporting the State MoH of Adamawa, Borno and IDP CAMPS CUMULATIVE CONSULTATIONS Yobe states on preparedness and response planning for cerebro- spinal meningitis epidemic prevention and control in the north-east 217,335 MEDICAL CONSULTATIONS*** region. A draft epidemic preparedness and response plan has been prepared for north-east Nigeria. A one-day workshop was organized EARLY WARNING & ALERT RESPONSE in Maiduguri on Wednesday 19th April to discuss the preparedness 149 EWARS SENTINEL SITES 91 REPORTING SENTINEL SITES and response plan under the lead of Borno State Ministry of Health supported by WHO, UNICEF and Health Sector Partners 21 TOTAL ALERTS RAISED**** In Yobe, state Ministry of Health and partners are on high alert while VACCINATION undertaking preparedness and response interventions for containment of cerebro spinal meningitis (CSM) outbreak. -

Local and International Responses to Attacks on Healthcare in Conflict Zones
L O C A L A N D I NTERNATIONAL R ESPONSES TO A T T A C K S O N H EALTHCARE IN C O N F L I C T Z ONES A CASE STUDY OF SYRI A Master of Arts in Law and Diplomacy Capstone Project Submitted by: Karen Taylor Advisor: Professor Elizabeth Stites July 21, 2018 Acknowledgements This paper is dedicated to the doctors, nurses and aid workers working in conflict zones who risk their lives every day to help others. You have shown us the true meaning of sacrifice. Without your dedicated service, healthcare for civilians in Syria would cease to exist. Many thanks to my advisor, Dr. Elizabeth Stites, for her timely and thoughtful guidance throughout the process. Thank you to Dr. Jennifer Leaning, Dr. Alex De Waal, Dr. Kimberly Howe and Dr. Stephanie Kayden for providing key suggestions that shaped the flow of this paper, and for helping me locate resources and participants to interview. Thank you to my husband and my parents for their constant support and encouragement. 1 TABLE OF CONTENTS Introduction ............................................................................................................................ 4 Methodology ............................................................................................................................ 5 Scope ...................................................................................................................................... 5 Global Prevalence of the Issue ............................................................................................................ 5 Categorization -

Providing Healthcare in Armed Conflict: the Case of Nigeria
Providing Healthcare in Armed Conflict: The Case of Nigeria JANUARY 2019 This issue brief was drafted by Alice Introduction Debarre, Senior Policy Analyst at IPI. It accompanies a policy paper published in 2018 entitled “Hard to Nigeria is facing multiple crises across the country. In the northeast, particu - Reach: Providing Healthcare in larly in the states of Borno, Adamawa, and Yobe, the government is fighting Armed Conflict,” as well as another the Boko Haram insurgency. Since the beginning of the conflict, over 20,000 case study on provision of health - people have reportedly been killed, over 2 million are internally displaced, and care in Mali. These papers aim to over 200,000 have fled to Cameroon, Niger, or Chad. 1 In the Middle Belt assist UN agencies, NGOs, member region, conflicts between herders and farmers escalated in 2018, killing over states, and donor agencies in 1,300 over the course of the year, making it deadlier than the Boko Haram providing and supporting the insurgency. 2 Climate change is one of the causes of this conflict, as it has provision of adequate health brought about desertification, resulting in clashes over resources. 3 Nigeria is services to conflict-affected popula - also dealing with an influx of refugees fleeing the violence in Cameroon’s tions. Anglophone region and arriving in Cross River, Benue, and Taraba States. 4 This issue brief is based on a Despite the humanitarian needs triggered by these other crises, the bulk of the combination of desk and field humanitarian response and the only large-scale humanitarian structure are in research. -

Idps and Public Health
IDPs and Public Health Bayard Roberts Revitalising IDP Research Workshop 20 July 2018 1 1. Evidence on health effects – mortality Meta analysis: death rate ratios (emergency death rates over baseline death rates), by displacement status Source: Heudtlass et al. Excess mortality in refugees, internally displaced persons and resident populations in complex humanitarian emergencies (1998-2012). Confl Health, 2016. 10. Evidence on health effects ealth effects – mental health Meta-analysis: Effect size means of mental disorder outcomes associated with locus of displacement: Key points: • Worse mental health outcomes for IDPs compared to refugees • Strong influence of ongoing daily stressors (e.g. insecurity & economic insecurity) • Longevity of burden of mental disorders among small group • Ongoing research gaps – access to MHPSS services; responsiveness of health systems Source: Porter M, Haslam N. Predisplacement and Postdisplacement Factors Associated With Mental Health of Refugees and Internally Displaced Persons. A meta-analysis. JAMA. 2005;294(5):602–612. 2. Research and evidence gaps Systematic review on evidence gaps on effectiveness of public health interventions in humanitarian crises in LMICs, 1980-2014 Number of quantitative papers on health intervention effectiveness for IDPs (N=22) and refugees (N=52), by health outcome 25 20 15 Refugees IDPs 10 Number Number of papers 5 0 Communicable Nutrition Mental health NCDs SRH/MCH diseases Source: Blanchet, …Roberts B. et al. Lancet, 390, 18-27 Nov 2017 Systematic review on evidence gaps on effectiveness of public health interventions in humanitarian crises in LMICs, 1980-2014 Key messages: • Limited studies overall and on specific health topics (e.g. NCDs) • Only marginal increase in number of papers over time • One study with urban IDPs • No studies including economic methods • Few studies including process implementation & effectiveness Source: Blanchet, …Roberts B. -

Northeast Nigeria Response BORNO State Health Sector Bulletin
BORNO STATE GOVERNMENT Hard to Reach team providing basic health services in a community in Borno State (Photo: WHO) Northeast Nigeria Response BORNO State Health Sector Bulletin #22 31st March 2017 6.9 MILLION 5.9 MILLION 1,506,170* PEOPLE IN NEED OF TARGET BY THE HEALTH 1,891,160 IDPS IN HEALTH CARE IN; SECTOR; ADAMAWA, POLIO VACCINATED CHILDREN ADAMAWA, BORNO AND BORNO AND YOBE BORNO STATE YOBE STATES STATES HIGHLIGHTS HEALTH SECTOR Despite security challenges in Borno state, more than 19 HEALTH SECTOR PARTNERS 14,000 volunteers were deployed to vaccinate 1.9 million HEALTH FACILITIES** children under 5-years old against wild poliovirus. The 288 exercise, which is the first nationwide campaign against polio FUNCTIONING** (OF TOTAL 749 ASSESSED HEALTH FACILITIES) this year, took place from 25 to 29 March 2017. WHO and partners have trained 1,817 house-to-house, 410 fixed posts 262 FULLY DESTROYED 215 and 362 transit teams in addition to 150 health camps across PARTIALLY DAMAGED 206 wards in all local government areas (LGAs) except IDP CAMPS CUMULATIVE CONSULTATIONS Abadam and Marte due to insecurity. 119,885 MEDICAL CONSULTATIONS*** Risk of disease outbreaks looms as temperatures continue to rise over the coming weeks and months. For instance, the EARLY WARNING & ALERT RESPONSE rainy season in April will further heighten the risk of cholera 149 EWARS SENTINEL SITES 87 REPORTING SENTINEL SITES and meningitis epidemics and cases of malaria. 20 TOTAL ALERTS RAISED**** More than 84 Mobile Health Teams are operational across accessible areas in Borno state providing health services to VACCINATION the affected population. -

Internal Displacement's Impacts on Health in Yemen (PDF)
INTERNAL DISPLACEMENT’S IMPACTS ON HEALTH IN YEMEN www.internal-displacement.org ACKNOWLEDGEMENTS Authors: Suprenant, M.P.1; Hussein, R.1; Al Dheeb, N.2; Basaleem, H.3; Zaman, M.1, Yasukawa, L.4 Editor: Jeremy Lennard Design and layout: Gregory van der Donk Cover Image: Children fetching clean water at a water distribution point supported by UNICEF in Al-Dhalie governorate, Yemen. © UNICEF/UN0372135/Alzekri, January 2020. 1. Boston University 2. UNICEF 3. University of Aden 4. IDMC INTERNAL DISPLACEMENT’S IMPACTS ON HEALTH IN YEMEN TABLE OF CONTENTS | Introduction . 5 | IDPs’ health risks � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 6 | Climate change, disasters and IDPs’ access to healthcare . 8 | The impact of decreasing aid on IDPs’ health . .10 || Impacts on health . 11 || Impacts on livelihoods ���������������������������������������������������������������������������������������������������������������������������� 13 || Impacts on housing . 13 || Impacts on education ���������������������������������������������������������������������������������������������������������������������������� 13 || Conclusion . 14 | Policy implications . .15 | Conclusion . .17 | Notes ����������������������������������������������������������������������������������������������������������������������������������������18 A young child is measured while being screened for severe acute malnutrition at Arhab Health Centre in Sana’a governorate, Yemen. © UNICEF/UN0372081/Alzekri, June 2020. INTRODUCTION -

Resident/Humanitarian Coordinator Report on the Use of Cerf Funds
RESIDENT/HUMANITARIAN COORDINATOR REPORT ON THE USE OF CERF FUNDS RESIDENT/HUMANITARIAN COORDINATOR REPORT ON THE USE OF CERF FUNDS 19-UF-UKR-35074 UKRAINE UNDERFUNDED EMERGENCIES ROUND I DISRUPTION OF BASIC SERVICES 2019 RESIDENT/HUMANITARIAN COORDINATOR OSNAT LUBRANI REPORTING PROCESS AND CONSULTATION SUMMARY a. Please indicate when the After-Action Review (AAR) was conducted and who participated. N/A It was not possible to meet and jointly conduct an AAR due to restrictions imposed during the COVID-19 pandemic. Because of the urgent need to prepare a COVID-19 response, two UHF allocations and a new CERF COVID-related allocation, it was decided not to conduct a process virtually. In addition, the HCT has been involved in significant extra work to support the Government of Ukraine to respond to COVID-19. HCT members have also been involved in significant advocacy efforts to ensure the continuation of humanitarian access in NGCA after the closure of entry-exit crossing points (EECPs). Recipient agencies provided input through email. b. Please confirm that the Resident Coordinator and/or Humanitarian Coordinator (RC/HC) Report on the Yes No use of CERF funds was discussed in the Humanitarian and/or UN Country Team. As noted above, it was not possible to meet in person, and there was no virtual discussion. c. Was the final version of the RC/HC Report shared for review with in-country stakeholders (i.e. the CERF recipient agencies and their implementing partners, cluster/sector coordinators and members and relevant Yes No government counterparts)? The report was shared and reviewed by the HC and the HCT.