Providing Healthcare in Armed Conflict: the Case of Nigeria
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Country Policy and Information Note: Medical and Healthcare Issues, Nigeria, January 2020
Country Policy and Information Note Nigeria: Medical and healthcare issues Version 3.0 January 2020 Preface Purpose This note provides country of origin information (COI) for decision makers handling cases where a person claims that to remove them from the UK would be a breach Articles 3 and / or 8 of the European Convention on Human Rights (ECHR) because of an ongoing health condition . It is not intended to be an exhaustive survey of healthcare in Nigeria. Country of origin information The country information in this note has been carefully selected in accordance with the general principles of COI research as set out in the Common EU [European Union] Guidelines for Processing Country of Origin Information (COI), dated April 2008, and the Austrian Centre for Country of Origin and Asylum Research and Documentation’s (ACCORD), Researching Country Origin Information – Training Manual, 2013. Namely, taking into account the COI’s relevance, reliability, accuracy, balance, currency, transparency and traceability. The structure and content of the country information section follows a terms of reference which sets out the general and specific topics relevant to this note. All information included in the note was published or made publicly available on or before the ‘cut-off’ date(s) in the country information section. Any event taking place or report/article published after these date(s) is not included. All information is publicly accessible or can be made publicly available, and is from generally reliable sources. Sources and the information they provide are carefully considered before inclusion. Factors relevant to the assessment of the reliability of sources and information include: • the motivation, purpose, knowledge and experience of the source • how the information was obtained, including specific methodologies used • the currency and detail of information, and • whether the COI is consistent with and/or corroborated by other sources. -
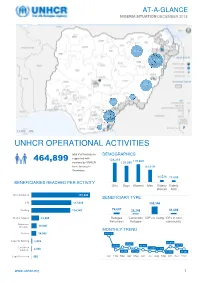
Unhcr Operational Activities 464,899
AT-A-GLANCE NIGERIA SITUATION DECEMBER 2018 28,280 388,208 20,163 1,770 4,985 18.212 177 Bénéficiaires Reached UNHCR OPERATIONAL ACTIVITIES total # of individuals DEMOGRAPHICS supported with 464,899 128,318 119,669 services by UNHCR 109,080 from January to 81,619 December; 34,825 of them from Mar-Apr 14,526 11,688 2018 BENEFICIARIES REACHED PER ACTIVITY Girls Boys Women Men Elderly Elderly Women Men Documentation 172,800 BENEFICIARY TYPE CRI 117,838 308,346 Profiling 114,747 76,607 28,248 51,698 Shelter Support 22,905 Refugee Cameroon IDPs in Camp IDPs in host Returnees Refugee community Awareness Raising 16,000 MONTHLY TREND Referral 14,956 140,116 Capacity Building 2,939 49,819 39,694 24,760 25,441 34,711 Livelihood 11,490 11,158 Support 2,048 46,139 37,118 13,770 30,683 Legal Protection 666 Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec www.unhcr.org 1 NIGERIA SITUATION AT-A-GLANCE / DEC 2018 CORE UNHCR INTERVENTIONS IN NIGERIA UNHCR Nigeria strategy is based on the premise that the government of Nigeria assumes the primary responsibility to provide protection and assistance to persons of concern. By building and reinforcing self-protection mechanisms, UNHCR empowers persons of concern to claim their rights and to participate in decision-making, including with national and local authorities, and with humanitarian actors. The overall aim of UNHCR Nigeria interventions is to prioritize and address the most serious human rights violations, including the right to life and security of persons. -

National Coordination Meeting
National Coordination Meeting Kyiv, 20 January 2021 Business of the Day 1. Q&A on Health Reform. Guest speakers: • Dr. Elina Dale, Adviser on Health Policy at WHO Ukraine • Anastasiya Brylova, Officer on Service Delivery, WHO Ukraine 2. Health Cluster Calendar 2021 3. Situation update: COVID-19 and ECA - WHO & partners 4. Update on Public Health Situation Analysis (PHSA) and ongoing assessments 5. Health Cluster M&E Framework 6. AOB • Update on Q4 2020 HRP and COVID-19 reporting • Update on COVID-19 Distribution Planning Tool (4W) • Health Cluster Assessment Database Health Cluster Meeting Q&A on Health Reform in Ukraine Dr. Elina Dale, Adviser on Health Policy Anastasiya Brylova , Officer on Service Delivery WHO Ukraine 2. HС Calendar Q1 & Q2 2021 # Month Date Q&A topics (TBC) 1 January 20 Health reform HeRAMS, Attacks on Health 2 February 3 Facilities 3 February 17 IPC & WASH 4 March 3 MHPSS 5 March 17 HIV/TB 6 April 14 Laboratories 7 April 28 Field focus: GCA & NGCA 8 May 12 Post COVID Rehab Human Rights/Protection and 9 May 26 Health 10 June 2 Epi and Surveillance 11 June 9 Behavioral Insights 12 June 16 Comms in Health 4. Public Health Situation Analysis (PHSA) • PHSA is part of the Public Health Information Services (PHIS) tools of the Global Health Cluster. • Provides all health sector partners with a common and comprehensive understanding of the public health situation in a crisis in order to inform evidence-based collective humanitarian health response planning. Focus of the assessment: Donetska & Luhanska Oblasts Eastern Ukraine -

Advanced Practice Nursing in Nigerian Healthcare: Prospects and Challenges
Journal of Social Change 2019, Volume 11, Issue 1, Pages 61–74 DOI: 10.5590/JOSC.2019.11.1.06 Advanced Practice Nursing in Nigerian Healthcare: Prospects and Challenges Raymond O. Chimezie University of San Francisco Sally N. Ibe Federal University of Technology This study explored the prospects and challenges of introducing advanced practice nursing (APN) in the Nigerian health system. It sought to address the following: career pathways for registered nurses and midwives, advanced duties performed by them and the circumstances, their views and willingness for autonomous practice, and doctors’ degree of acceptance. Research population composed of registered nurses, midwives and medical doctors in primary healthcare. The conceptual framework for this study was based on the scope of practice, standards and competencies of the APN established by the International Council of Nurses (2008). A 12-item checklist of typical duties of APN from the framework provided a guide for the design of eight main questions and 19 subquestions. Data was collected from 17 participants through in-depth interviews and group discussions and analyzed using Charmaz’s three simplified methods for qualitative data. Findings were that (a) registered nurses and midwives are constrained to perform advanced duties, (b) doctors delegate advanced roles to nurses and midwives, (c) nurses and midwives lacked pathways for advancement, (d) APN would substitute for doctor shortage, and (e) advocacy and lobbying has to done by the Nursing and Midwifery Council of Nigeria to change the current policy. The social change implication is that it offers insight into the potentials for APN in healthcare delivery. Keywords: advanced practice nursing, advanced nursing, nursing education in Nigeria, healthcare in Nigeria, health workforce development, primary healthcare in Nigeria Introduction Background Nigeria’s three-tier health system is managed in accordance with the three tiers of government: the local (primary), state (secondary), and federal (tertiary). -

North-East Nigeria January 2021
OPERATIONAL UPDATE North-East Nigeria January 2021 Over 6,100 men, women and UNHCR’s protection, human rights and UNHCR and partners raised children were newly border monitoring teams reached nearly awareness about COVID-19 and displaced in Borno, 33,000 internally displaced people and protection among over 22,000 Adamawa and Yobe States refugee returnees in Borno, Adamawa and people in the BAY States in in January. Yobe (BAY) States. January 2021. A UNHCR protection partner colleague conducts a rapid protection assessment with internally displaced people in Bama, Borno State. © UNHCR/Daniel Bisu www.unhcr.or g 1 NORTH-EAST NIGERIA OPERATIONAL UPDATE JANUARY 2021 Operational Highlights ■ The security situation in the North-East remains unpredictable. The operational area continues to be impacted by the ongoing violent conflict, terrorism, and criminal activities, which have resulted in the displacement, killing and abduction of civilians as well as the destruction of properties and critical infrastructure. The second wave of COVID-19 also continues to exacerbate the already worsening situation. A total of 43 security incidents perpetrated by NSAG in the BAY States comprised of attacks on civilians, improvised explosive devices, and attacks on security forces. ■ In Borno State, members of the non-State armed groups (NSAGs) continued their attacks on both civilian and military targets, attempted to overrun of villages and towns and mounted illegal vehicle checkpoints for the purpose of abduction, looting and robbery. The main supply routes Maiduguri- Gubio, Maiduguri-Mafa and Mungono-Ngala in the Northern axis were most severely hit. The situation along the Maiduguri-Damaturu road, a main supply route, worsened further in January, forcing the reclassification of the route from the hitherto “Restricted” to “No go” for humanitarian staff and cargo. -

Agulu Road, Adazi Ani, Anambra State. ANAMBRA 2 AB Microfinance Bank Limited National No
LICENSED MICROFINANCE BANKS (MFBs) IN NIGERIA AS AT FEBRUARY 13, 2019 S/N Name Category Address State Description 1 AACB Microfinance Bank Limited State Nnewi/ Agulu Road, Adazi Ani, Anambra State. ANAMBRA 2 AB Microfinance Bank Limited National No. 9 Oba Akran Avenue, Ikeja Lagos State. LAGOS 3 ABC Microfinance Bank Limited Unit Mission Road, Okada, Edo State EDO 4 Abestone Microfinance Bank Ltd Unit Commerce House, Beside Government House, Oke Igbein, Abeokuta, Ogun State OGUN 5 Abia State University Microfinance Bank Limited Unit Uturu, Isuikwuato LGA, Abia State ABIA 6 Abigi Microfinance Bank Limited Unit 28, Moborode Odofin Street, Ijebu Waterside, Ogun State OGUN 7 Above Only Microfinance Bank Ltd Unit Benson Idahosa University Campus, Ugbor GRA, Benin EDO Abubakar Tafawa Balewa University Microfinance Bank 8 Limited Unit Abubakar Tafawa Balewa University (ATBU), Yelwa Road, Bauchi BAUCHI 9 Abucoop Microfinance Bank Limited State Plot 251, Millenium Builder's Plaza, Hebert Macaulay Way, Central Business District, Garki, Abuja ABUJA 10 Accion Microfinance Bank Limited National 4th Floor, Elizade Plaza, 322A, Ikorodu Road, Beside LASU Mini Campus, Anthony, Lagos LAGOS 11 ACE Microfinance Bank Limited Unit 3, Daniel Aliyu Street, Kwali, Abuja ABUJA 12 Achina Microfinance Bank Limited Unit Achina Aguata LGA, Anambra State ANAMBRA 13 Active Point Microfinance Bank Limited State 18A Nkemba Street, Uyo, Akwa Ibom State AKWA IBOM 14 Ada Microfinance Bank Limited Unit Agwada Town, Kokona Local Govt. Area, Nasarawa State NASSARAWA 15 Adazi-Enu Microfinance Bank Limited Unit Nkwor Market Square, Adazi- Enu, Anaocha Local Govt, Anambra State. ANAMBRA 16 Adazi-Nnukwu Microfinance Bank Limited Unit Near Eke Market, Adazi Nnukwu, Adazi, Anambra State ANAMBRA 17 Addosser Microfinance Bank Limited State 32, Lewis Street, Lagos Island, Lagos State LAGOS 18 Adeyemi College Staff Microfinance Bank Ltd Unit Adeyemi College of Education Staff Ni 1, CMS Ltd Secretariat, Adeyemi College of Education, Ondo ONDO 19 Afekhafe Microfinance Bank Ltd Unit No. -

Growth Geographical Determinants of the Structural and Functional
Growth Vol. 1, No. 1, 10-17, 2014 http://asianonlinejournals.com/index.php/Growth Geographical Determinants of the Structural and Functional Growth of Damaturu Town in Yobe State, Nigeria Ahmed AbubakarJajere1* --- Ibrahim Jaro Musa2 --- Muhammad Isma’il3 1Department of Geography, Umar Sulaiman College of Education, Gashua 2,3Department of Geography, Ahmadu Bello University, Zaria Abstract Damaturu town became the capital of Yobe State when the state was created in 1991. Since then, the town has been experiencing rapid changes in the landuse/landcover types due to urban expansion, economic development, and social transformation in the town. This study examined the geographical determinants of the growth of Damaturu town from 1986 to 2009. The satellite imageries of Damaturu were obtained processed and analysed using Remote Sensing and Geographic Information System techniques to determine the growth rate of the town within the period of study. This was complemented with the information acquired from the field survey to achieve the objectives of the study. Findings revealed that within this period (1991-1999), Damaturu built-up area increased about four times while the urban area increased more than four times. This significant growth was influenced by the location of the administrative offices and housing estates at the periphery of the town, categorisation of the land into administrative, residential, commercial, and industrial areas; as well as the transportation network and substantial population growth within the period. The most influential change within the second period (1999-2005) was increased agriculture and significant urban expansion. Within the current period (2005-2009), the urban area expanded by about 22Km2. -

Nigeria – Complex Emergency JUNE 7, 2021
Fact Sheet #3 Fiscal Year (FY) 2021 Nigeria – Complex Emergency JUNE 7, 2021 SITUATION AT A GLANCE 206 8.7 2.9 308,000 12.8 MILLION MILLION MILLION MILLION Estimated Estimated Number of Estimated Estimated Projected Acutely Population People in Need in Number of IDPs Number of Food-Insecure w of Nigeria Northeast Nigeria in Nigeria Nigerian Refugees Population for 2021 in West Africa Lean Season UN – December 2020 UN – February 2021 UNHCR – February 2021 UNHCR – April 2021 CH – March 2021 Major OAG attacks on population centers in northeastern Nigeria—including Borno State’s Damasak town and Yobe State’s Geidam town—have displaced hundreds of thousands of people since late March. Intercommunal violence and OCG activity continue to drive displacement and exacerbate needs in northwest Nigeria. Approximately 12.8 million people will require emergency food assistance during the June-to-August lean season, representing a significant deterioration of food security in Nigeria compared with 2020. 1 TOTAL U.S. GOVERNMENT HUMANITARIAN FUNDING USAID/BHA $230,973,400 For the Nigeria Response in FY 2021 State/PRM2 $13,500,000 For complete funding breakdown with partners, see detailed chart on page 7 Total $244,473,400 1 USAID’s Bureau for Humanitarian Assistance (USAID/BHA) 2 U.S. Department of State Bureau for Population, Refugees, and Migration (State/PRM) 1 KEY DEVELOPMENTS Violence Drives Displacement and Constrains Access in the Northeast Organized armed group (OAG) attacks in Adamawa, Borno, and Yobe states have displaced more than 200,000 people since March and continue to exacerbate humanitarian needs and limit relief efforts, according to the UN. -

Drought Occurrences and Its Implications on the Households in Yobe State, Nigeria Jude Nwafor Eze
Eze Geoenvironmental Disasters (2018) 5:18 Geoenvironmental Disasters https://doi.org/10.1186/s40677-018-0111-7 RESEARCH Open Access Drought occurrences and its implications on the households in Yobe state, Nigeria Jude Nwafor Eze Abstract The study assesses the extent of droughts and its implications on the households in the study area. This is to highlight the need to integrate drought adaptation options into the government development plans. Strategies for drought adaptation options in the study area have often been made without experimental foundations placed on the extent of drought and its implications on the households. To achieve this, the study employed Normalized Rainfall Index (NRI) to determine the extent of droughts and its implications on the households, which has much to offer in terms of policy decisions. The study also utilized questionnaire administrated to 400 households to determine the annual income from different occupations that yielded more income to the people in the study area using one-way analysis of variance (ANOVA). The NRI shows that the study area was characterized by mild to severe drought events. The first (1986–1995) and third (2006–2017) decades experienced high incidences of droughts, while the second decade (1996–2005), witnessed the least incidences of droughts. The result of the economic activities of the households reveals that 65% of the total household respondents were involved in farming, while 35% were involved in non-farming activities as their major source of livelihood. The analysis of variance on the economic activities that generated more income to the households in Yobe State shows that farming activities provided more opportunities for income generation. -
![English.Pdf Purchasing Power Parity [PPP])—Much Lower Than 2 World Bank](https://docslib.b-cdn.net/cover/2888/english-pdf-purchasing-power-parity-ppp-much-lower-than-2-world-bank-1082888.webp)
English.Pdf Purchasing Power Parity [PPP])—Much Lower Than 2 World Bank
CENTRAL Public Disclosure Authorized AFRICAN REPUBLIC ECONOMIC Public Disclosure Authorized UPDATE FOURTH EDITION Investing in Public Disclosure Authorized Human Capital to Protect the Future JULY 2021 Public Disclosure Authorized © 2021 The World Bank 1818 H Street NW, Washington DC 20433 Telephone: 202-473-1000; Internet: www.worldbank.org Some rights reserved This work is a product of the staff of The World Bank. The findings, interpretations, and conclusions expressed in this work do not necessarily reflect the views of the Executive Directors of The World Bank or the governments they represent. The World Bank does not guarantee the accuracy of the data included in this work. The boundaries, colors, denominations, and other information shown on any map in this work do not imply any judgment on the part of The World Bank concerning the legal status of any territory or the endorsement or acceptance of such boundaries. Rights and Permissions The material in this work is subject to copyright. Because The World Bank encourages dissemination of its knowledge, this work may be reproduced, in whole or in part, for noncommercial purposes as long as full attribution to this work is given. Attribution—Please cite the work as follows: “World Bank. 2021. Central African Republic Economic Update: Investing in Human Capital to Protect the Future. © World Bank.” All queries on rights and licenses, including subsidiary rights, should be addressed to World Bank Publications, The World Bank Group, 1818 H Street NW, Washington, DC 20433, USA; fax: 202-522-2625; -

Nigeria's Financing of Health Care During the COVID-19 Pandemic
Munich Personal RePEc Archive Nigeria’s financing of health care during the COVID-19 pandemic: challenges and recommendations Aregbeshola, Bolaji Samson and Folayan, Morenike Oluwatoyin The University of Newcastle, Australia, Obafemi Awolowo University, Nigeria January 2021 Online at https://mpra.ub.uni-muenchen.de/105293/ MPRA Paper No. 105293, posted 25 Jan 2021 02:47 UTC Nigeria’s financing of health care during the COVID-19 pandemic: challenges and recommendations Bolaji Samson Aregbeshola The University of Newcastle, Australia Morenike Oluwatoyin Folayan Obafemi Awolowo University, Nigeria Abstract An analysis of the financing of Nigeria’s health care system in response to the COVID- 19 pandemic, using three key health care financing indicators: revenue collection, pooling, and purchasing was conducted. Nigeria projected that it would need US$330 million to control its COVID-19 pandemic. However, it raised more than US$560.52 million, of which more than 90% came from the private sector and the donor/philanthropist community. The pooled COVID-19 fund is mainly being expended on temporary public health and clinical care measures, with little invested to strengthen the health system beyond the pandemic. The poor turn-around time for COVID-19 test results and the huge stigma associated with the disease results in most persons with mild to moderate symptoms seeking care from alternatives to the healthcare institutions designated for COVID-19 health care. The huge out-of-pocket expenses, and the inability of most Nigerians to earn money because of measures instituted to contain the pandemic, will likely cause many Nigerians to become economically impoverished by the COVID-19 pandemic. -

Sustainable Healthcare System in Nigeria: Vision, Strategies and Challenges
IOSR Journal of Economics and Finance (IOSR-JEF) e-ISSN: 2321-5933, p-ISSN: 2321-5925.Volume 5, Issue 2. (Sep.-Oct. 2014), PP 28-39 www.iosrjournals.org Sustainable Healthcare System in Nigeria: Vision, Strategies and Challenges. Oyibocha, E.O.a, Irinoye, O.b, Sagua, E.O.c, Ogungide – Essien, O.T.d, Edeki, J.E.e & Okome, O.L.f. 1School of Nursing, Warri, Delta State 2Department of Nursing, Obafemi Awolowo University, Ile – Ife, Osun State 3Faculty of Nursing, Medical – Surgical Department, Niger – Delta University, Bayelsa State 4Family Planning Clinic, Department of Obstetrics and Gynaecology, College of Medicine, University of Ibadan, Oyo State. 5Primary Health Care Department, Ukwani Local Government Area, Obiaruku, Delta State 6School of Nursing, Eku, Delta State __________________________________________________________________________________________ Abstract: Every nation’s dream is for its government to achieve a sustainable improvement in the quality of life of its citizens. This can only be achieved through good governance and planned actions that detail the vision, mission, goals/objectives and strategies to be attained over a given period of time. Nigeria like other countries around the globe has not for once lacked any development plans. Unfortunately, with its current estimated population of 150 million and estimated total of 23,640 health facilities operated via a three – tiered governance structure, it is still ranked by World Health Organization at 187th position in its health system among 191 member states. This article reviewed related relevant literature which revealed that, for more than two decades ago, African countries including Nigeria have been plunged into economic crisis which seriously affected a large portion of their populations and raised social and political tensions.