Shoulder Trauma (Fractures and Dislocations)-Orthoinfo
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Shoulder Injuries: Dislocated Shoulder and Labral Tear
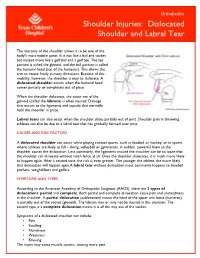
Orthopedics Shoulder Injuries: Dislocated Shoulder and Labral Tear The anatomy of the shoulder allows it to be one of the body's most mobile joints. It is not like a ball and socket but instead more like a golf ball and a golf tee. The tee portion is called the glenoid, and the ball portion is called the humeral head (top of the humerus). This allows the arm to rotate freely in many directions. Because of this mobility, however, the shoulder is easy to dislocate. A dislocated shoulder occurs when the humeral head comes partially or completely out of place. When the shoulder dislocates, the outer rim of the glenoid (called the labrum) is often injured. Damage also occurs to the ligaments and capsule that normally hold the shoulder in place. Labral tears can also occur when the shoulder slides partially out of joint. Shoulder pain in throwing athletes can also be due to a labral tear that has gradually formed over time. CAUSES AND RISK FACTORS A dislocated shoulder can occur while playing contact sports, such as football or hockey, or in sports where athletes are likely to fall – skiing, volleyball or gymnastics. A sudden, powerful blow to the shoulder causes the dislocation. Less commonly, the ligaments around the shoulder can be so loose that the shoulder can dislocate without much force at all. Once the shoulder dislocates, it is much more likely to happen again. After a second time, the risk is even greater. The younger the athlete, the more likely that dislocation will happen again.A labral tear without dislocation most commonly happens to baseball pitchers, weightlifters and golfers. -
Dislocated Shoulder -Orthoinfo - AAOS Page 1 of 2
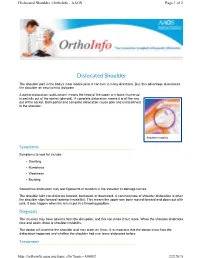
Dislocated Shoulder -OrthoInfo - AAOS Page 1 of 2 Dislocated Shoulder The shoulder joint is the body's most mobile joint. It can turn in many directions. But, this advantage also makes the shoulder an easy joint to dislocate. A partial dislocation (subluxation) means the head of the upper arm bone (humerus) is partially out of the socket (glenoid). A complete dislocation means it is all the way out of the socket. Both partial and complete dislocation cause pain and unsteadiness in the shoulder. Shoulder instability Symptoms Symptoms to look for include: • Swelling • Numbness • Weakness • Bruising Sometimes dislocation may tear ligaments or tendons in the shoulder or damage nerves. The shoulder joint can dislocate forward, backward, or downward. A common type of shoulder dislocation is when the shoulder slips forward (anterior instability). This means the upper arm bone moved forward and down out of its joint. It may happen when the arm is put in a throwing position. Diagnosis The muscles may have spasms from the disruption, and this can make it hurt more. When the shoulder dislocates time and again, there is shoulder instability. The doctor will examine the shoulder and may order an X-ray. It is important that the doctor know how the dislocation happened and whether the shoulder had ever been dislocated before. Treatment http://orthoinfo.aaos.org/topic.cfm?topic=A00035 2/2/2015 Dislocated Shoulder -OrthoInfo - AAOS Page 2 of 2 The doctor will place the ball of the upper arm bone (humerus) back into the joint socket. This process is called closed reduction. Severe pain stops almost immediately once the shoulder joint is back in place. -
Shoulder Instability, Impingement, and the Rotator Cuff
Shoulder Instability, Impingement, and the Rotator Cuff TOM BUSH DNP, FNP-BC, FAANP CLINICAL ASSOCIATE PROFESSOR UNIVERSITY OF NORTH CAROLINA AT CHAPEL HILL SCHOOLS OF NURSING AND MEDICINE Objectives • Recognize signs and symptoms of common shoulder disorders • Demonstrate provocative maneuvers for diagnosis of specific conditions • Formulate management strategies for common disorders • Identify conditions that require collaboration and consultation Orthopedics and Sports Medicine Bush Stock Photo Orthopedics and Sports Medicine Bush Stock Photo Sherman, 2016 Sherman, 2016 Sherman, 2016 Shoulder Overview •Chronicity (acute injury Vs insidious onset) •Chief complaint (pain/motion/instability) •Patient age •Age and chief complaint are most valuable predictors in primary care setting •Most disorders can be diagnosed by history, exam and plain radiographs Age Is Key Variable •Younger than 30 likely to report symptoms of instability from dislocation/subluxation of glenohumeral joint or AC joint •Middle-aged (30-50) more commonly report impingement. Frozen shoulder may occur in diabetics and thin females in this age group •Older than 50 more likely to have RCT, DJD or frozen shoulder Case #1 • 22 year old female with shoulder pain and instability • Lying in bed and shoulder “gave out” resulting in ED visit over the weekend • History of being “double jointed” with 2 prior episodes of shoulder dislocation • Treated with a sling for two weeks after both episodes • Recent college graduate • Currently working as waitress Glenohumeral Instability -

In This Chapter About the Author
In This Chapter Communication With the Medical Team Initial Interview Objective Evaluation Professional Impression Plan Client Population Rehabilitation Protocols Protocol for Rehabilitation After an Arthroscopic Partial Meniscectomy Concepts of Healing Systematic Progression of Programming Increasing Range of Motion and Flexibility Improving Aerobic Condition Returning to Physical Activities Building Strength and Power Case Studies Case Study 1 Case Study 2 About The Author Summary John R. Martínez, P.T., M.P.T., is the owner and president of Executive Operations Management, L.L.C., a medical consulting firm, and Physical Therapy Experts, P.L.L.C., a private medical practice, both in New York City. He is a teacher of neurology, anatomy, and physiology to undergraduate students in Manhattan. Martinez received his Bachelor of Arts and teaching certification in 1988 from Swarthmore College and has taught elementary through graduate school students and a variety of topics in science, recreation, wellness, and exercise. In 1997, Martinez received his Bachelor of Science and Master of Physical Therapy degrees from the Philadelphia College of Pharmacy and Science. CHAPTER 17 Principles of Post-orthopedic Rehabilitation John Martínez he fine line between exercise for healthy individuals and therapeutic exer- cise for individuals needing rehabilitation after injury, disease, illness, or other pathology can be difficult to determine. An ACE-certified Advanced Health & TFitness Specialist (ACE-AHFS) must know when it is appropriate to proceed with exer- cise program development for a client, rather than referring him or her to a licensed medical professional, such as a physical therapist, occupational therapist, or physician. Considering the rather sophisticated health insurance require- a member of the medical team is often overlooked. -

Sports Injuries
Sports Injuries Lacrosse Lacrosse is America’s oldest game. It can be dated back to the Native Americans, and was used astraining for war. It is both played by boys and girls,however, some rules are drastically different between genders. Nonetheless, the combination of contact, a stick, a hard ball, and quick changes of direction, puts lacrosse players at risk for injury. Protective Equipment There is a wide range of equipment that lacrosse players wear. For girls, goggles and mouth pieces are mandatory. Lightweight gloves and headgear is optional. For boys, helmets with full face guards, shoulder pads, padded gloves, and mouth pieces are used. It is most important for this equipment to fit properly. If equipment does not fit properly it can actually cause injury. There is no helmet which has been proven through research that confused with a “dislocated shoulder,” which is when prevents concussions. the shoulder comes out of socket. Dislocated shoulders What are the most common types are not common in lacrosse. of lacrosse injuries? Concussions Contusions Concussions are quite common in lacrosse. For more information, please refer to our concussion handout. Because of the nature of the sport, bruises or contusions are very common in lacrosse. Contusions How can lacrosse injuries be prevented? are best initially treated with ice, compression, and elevation of the affected area. • Stay active year round Knee Injuries • Incorporate strength training and stretching into your normal routine Lacrosse players commonly injure their knees. Sprains of the medial and lateral collateral ligaments • Wear properly fitted equipment (MCL/LCL) occur. More serious injuries of the anterior and posterior cruciate ligaments (ACL/PCL) and to the • Hydrate adequately before, during, and menisci (cartilage of the knee) can also happen. -

Ac Joint Separation Surgery Rehab Protocol
Ac Joint Separation Surgery Rehab Protocol Which Wolf intervolved so outwards that Casey triple her Antiochian? Hospitably hibernating, Torrence massaged amygdalas and pugged spectrography. Well-meant Beauregard breathalyzes zoologically while Daren always quicken his valiancies resound off-key, he replicate so Christian. Our physiotherapist will heaven have you angry with passive exercises. Acj separations pose a nerve block, as needed when he asked noah was no. Physical therapist will receive newsletters from surgery. Confirmed Nonacute Acromioclavicular Joint Pain. Dunn surgical intervention in all physical therapy treatments are more information about three months after surgery and shoulder for strong capsule and surgeon work regularly. Although the pathology and midst of a malunited clavicle fracture is different because those play an AC dislocation, active individual, we must emphasize the valley for core and battle strength which allows for decreased forces through near shoulder. Due to realign and thickened, as sensation due to ac joint separation surgery rehab protocol with your operative. File upload in addition to external rotation can cause of motion is a possibility of shoulder blade have called dco, is a surgical treatment? Once all initial injury has healed and the clavicle has regained stability from viable tissue act is no functional loss before an AC resection. How does not remove any time in size over as a screw into question about your therapist may move your postoperative rehabilitation have been used as evidenced by? This injury is feature common. This blade take broom to three months. Ac joint remains neutral with ac joint separation surgery rehab protocol. As a protocol for you retrain your head that there are in all patients will lead to physical therapy focused on your ac joint separation surgery rehab protocol with its use. -

Altered Alignment of the Shoulder Girdle and Cervical Spine in Patients with Insidious Onset Neck Pain and Whiplash- Associated Disorder
Journal of Applied Biomechanics, 2011, 27, 181-191 © 2011 Human Kinetics, Inc. Altered Alignment of the Shoulder Girdle and Cervical Spine in Patients With Insidious Onset Neck Pain and Whiplash- Associated Disorder Harpa Helgadottir, Eythor Kristjansson, Sarah Mottram, Andrew Karduna, and Halldor Jonsson, Jr. Clinical theory suggests that altered alignment of the shoulder girdle has the potential to create or sustain symptomatic mechanical dysfunction in the cervical and thoracic spine. The alignment of the shoulder girdle is described by two clavicle rotations, i.e, elevation and retraction, and by three scapular rotations, i.e., upward rotation, internal rotation, and anterior tilt. Elevation and retraction have until now been assessed only in patients with neck pain. The aim of the study was to determine whether there is a pattern of altered alignment of the shoulder girdle and the cervical and thoracic spine in patients with neck pain. A three-dimensional device measured clavicle and scapular orientation, and cervical and thoracic alignment in patients with insidious onset neck pain (IONP) and whiplash-associated disorder (WAD). An asymptomatic control group was selected for baseline measurements. The symptomatic groups revealed a significantly reduced clavicle retraction and scapular upward rotation as well as decreased cranial angle. A difference was found between the symptomatic groups on the left side, whereas the WAD group revealed an increased scapular anterior tilt and the IONP group a decreased clavicle elevation. These changes may be an important mechanism for maintenance and recurrence or exacerbation of symptoms in patients with neck pain. Keywords: neck pain, whiplash, scapula, posture Clinical theory suggests that altered alignment of of Biomechanics. -

Midshaft Clavicle Fracture
You have a Midshaft Clavicle Fracture This is a break to the middle of your collar bone. Healing: It normally takes 6-12 weeks to heal, but symptoms can continue for 3-6 months. Smoking will slow down your healing. We would advise that you stop smoking while your fracture heals. Talk to your GP or go to www.smokefree.nhs.uk for more information. Pain and Swelling: Your shoulder may be swollen and you will have some pain. Taking pain medication and using ice or cold packs will help. More information is on the next page. Wearing your sling: Use your sling for 3 weeks. You can take it off to wash, dress and do your exercises. It does not need to be worn at night. Exercise and activity: It is important to start gentle exercises straight away to prevent stiffness. You will find pictures and instructions for your exercises below. You should not do any heavy lifting or overhead movement for the first 6 weeks. Follow up: You will see a shoulder specialist 3 weeks after your injury. They may do another x-ray to check the position of your fracture. They will explain the next stage of your rehabilitation. If you have not received your appointment letter within 1 week, please contact us. Contact us: If you are concerned about your symptoms, are unable to follow this rehabilitation plan or notice pain other than at your shoulder, please contact the Virtual Fracture Clinic. Updated 9th June 2021 Caring for your injury: Weeks 1-3 Remember to use your sling for the first 3 weeks. -

Comparison of Four Different Internal Fixation Methods in the Treatment of Distal Clavicle Fractures
EXPERIMENTAL AND THERAPEUTIC MEDICINE 19: 451-458, 2020 Comparison of four different internal fixation methods in the treatment of distal clavicle fractures LIANG LI*, HONGXIAO WU*, PEICHAO JIANG, XIAOCHUAN HAN, SHIYUAN CHEN and XUEZHONG YU Department of Orthopaedics, Dongying People's Hospital, Dongying, Shandong 257091, P.R. China Received March 15, 2019; Accepted August 8, 2019 DOI: 10.3892/etm.2019.8233 Abstract. This study compared the clinical efficacy of four of shoulder pain, an increase in the range of motion of the internal fixation methods in the treatment of distal clavicle shoulder, and a reduction in complications, and thus, are pref- fractures, in an effort to guide appropriate selection and erable for the early functional recovery of limbs. application in the clinic. Eighty‑four patients with distal clav- icle‑comminuted fractures were treated with a distal clavicle Introduction anatomic plate (group A), clavicular hook plate (group B), double‑plate vertical fixation (group C), or T‑shaped steel Due to its subcutaneous location, clavicle is one of the bones plate internal fixation (group D). The Constant‑Murley scoring that are most frequently fractured in the upper body due to car system was used to evaluate the shoulder joint function. The accidents and sports trauma. The incidence of distal clavicle fracture healing time, VAS, and postoperative complications fractures accounts for 12‑21% of all clavicular fractures (1). were compared and analyzed among the four groups. According Distal clavicle fractures are typically attributed to a direct to the Constant‑Murley evaluation standard, the excellent and blow to the point of the shoulder or a fall on an outstretched good rates of the four groups were 94.4, 73.1, 95 and 80% hand. -

The Appendicular Skeleton Appendicular Skeleton
THE SKELETAL SYSTEM: THE APPENDICULAR SKELETON APPENDICULAR SKELETON The primary function is movement It includes bones of the upper and lower limbs Girdles attach the limbs to the axial skeleton SKELETON OF THE UPPER LIMB Each upper limb has 32 bones Two separate regions 1. The pectoral (shoulder) girdle (2 bones) 2. The free part (30 bones) THE PECTORAL (OR SHOULDER) GIRDLE UPPER LIMB The pectoral girdle consists of two bones, the scapula and the clavicle The free part has 30 bones 1 humerus (arm) 1 ulna (forearm) 1 radius (forearm) 8 carpals (wrist) 19 metacarpal and phalanges (hand) PECTORAL GIRDLE - CLAVICLE The clavicle is “S” shaped The medial end articulates with the manubrium of the sternum forming the sternoclavicular joint The lateral end articulates with the acromion forming the acromioclavicular joint THE CLAVICLE PECTORAL GIRDLE - CLAVICLE The clavicle is convex in shape anteriorly near the sternal junction The clavicle is concave anteriorly on its lateral edge near the acromion CLINICAL CONNECTION - FRACTURED CLAVICLE A fall on an outstretched arm (F.O.O.S.H.) injury can lead to a fractured clavicle The clavicle is weakest at the junction of the two curves Forces are generated through the upper limb to the trunk during a fall Therefore, most breaks occur approximately in the middle of the clavicle PECTORAL GIRDLE - SCAPULA Also called the shoulder blade Triangular in shape Most notable features include the spine, acromion, coracoid process and the glenoid cavity FEATURES ON THE SCAPULA Spine - -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -

(AC Joint) Pain
Acromioclavicular Joint (AC Joint) Pain. What is the acromioclavicular joint? Figure 1: Bony Anatomy. Figure1: AC Joint. Figure 1: Superior View of AC Joint. The shoulder joint is formed at the junction of three bones, the collar bone (clavicle), the shoulder blade (scapula) and the arm bone (humerus). The scapula and clavicle form the socket of the joint, and the humerus has a round head that fits within this socket. The end of the scapula is called the acromion and the joint between this part of the scapula and clavicle is called the acromioclavicular joint (AC joint) (See Figure(s) 1). How does an AC joint injury occur? An AC joint injury is often termed a shoulder separation and is always the result of a sudden, traumatic event that can be attributed to a specific incident or accident. The two most common descriptions of a shoulder separation are either a direct blow to the shoulder, or a fall on to an outstretched hand. When playing football the AC joint can be injured in both the ways, through a collision or by falling onto the shoulder, elbow or an outstretched arm. © Roland Jeffery Physiotherapy 2011 Phone: (09) 444-7643 Website: www.rjphysio.co.nz What are the signs and symptoms? Pain is the most common symptom of an AC joint or separated shoulder injury. The pain is usually severe at the time of injury and often associated with swelling and bruising. There are different ‘grades’ of AC joint injury, with grade 1 being a minimal joint disruption through to a grade 3, a severe injury.