UNIVERSITY of CALIFORNIA Los Angeles Uncovering the Molecular
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ingenuity Pathway Analysis of Differentially Expressed Genes Involved in Signaling Pathways and Molecular Networks in Rhoe Gene‑Edited Cardiomyocytes
INTERNATIONAL JOURNAL OF MOleCular meDICine 46: 1225-1238, 2020 Ingenuity pathway analysis of differentially expressed genes involved in signaling pathways and molecular networks in RhoE gene‑edited cardiomyocytes ZHONGMING SHAO1*, KEKE WANG1*, SHUYA ZHANG2, JIANLING YUAN1, XIAOMING LIAO1, CAIXIA WU1, YUAN ZOU1, YANPING HA1, ZHIHUA SHEN1, JUNLI GUO2 and WEI JIE1,2 1Department of Pathology, School of Basic Medicine Sciences, Guangdong Medical University, Zhanjiang, Guangdong 524023; 2Hainan Provincial Key Laboratory for Tropical Cardiovascular Diseases Research and Key Laboratory of Emergency and Trauma of Ministry of Education, Institute of Cardiovascular Research of The First Affiliated Hospital, Hainan Medical University, Haikou, Hainan 571199, P.R. China Received January 7, 2020; Accepted May 20, 2020 DOI: 10.3892/ijmm.2020.4661 Abstract. RhoE/Rnd3 is an atypical member of the Rho super- injury and abnormalities, cell‑to‑cell signaling and interaction, family of proteins, However, the global biological function and molecular transport. In addition, 885 upstream regulators profile of this protein remains unsolved. In the present study, a were enriched, including 59 molecules that were predicated RhoE‑knockout H9C2 cardiomyocyte cell line was established to be strongly activated (Z‑score >2) and 60 molecules that using CRISPR/Cas9 technology, following which differentially were predicated to be significantly inhibited (Z‑scores <‑2). In expressed genes (DEGs) between the knockout and wild‑type particular, 33 regulatory effects and 25 networks were revealed cell lines were screened using whole genome expression gene to be associated with the DEGs. Among them, the most signifi- chips. A total of 829 DEGs, including 417 upregulated and cant regulatory effects were ‘adhesion of endothelial cells’ and 412 downregulated, were identified using the threshold of ‘recruitment of myeloid cells’ and the top network was ‘neuro- fold changes ≥1.2 and P<0.05. -

ORM-Like Protein (ORMDL) – Annäherung an Die Funktion Über Die Interaktion
ORM-like protein (ORMDL) - Annäherung an die Funktion über die Interaktion Julian Klingbeil München 2019 Aus der Kinderklinik und Kinderpoliklinik im Dr. von Haunerschen Kinderspital der Ludwig–Maximilians–Universität München Direktor: Prof. Dr. med. Dr. sci. nat. C. Klein ORM-like protein (ORMDL) – Annäherung an die Funktion über die Interaktion Dissertation zum Erwerb des Doktorgrades der Medizin an der Medizinischen Fakultät der Ludwig–Maximilians–Universität zu München vorgelegt von Julian Malte Klingbeil aus Berlin 2019 Mit Genehmigung der Medizinischen Fakultät der Universität München Berichterstatterin: Prof. Dr. Ania Muntau Mitberichterstatter: Prof. Dr. Katja Radon PD Dr. Anne Hilgendorff Prof. Dr. Jürgen Behr Prof. Dr. Ortrud Steinlein Mitbetreuung durch den promovierten Mitarbeiter: Prof. Dr. Søren Gersting Dekan: Prof. Dr. med. dent. Reinhard Hickel Tag der mündlichen Prüfung: 10.10.2019 Inhaltsverzeichnis Zusammenfassung xiii 1 Einleitung 1 1.1 Asthma bronchiale . .1 1.1.1 Epidemiologie, Pathogenese und Klassifikation . .2 1.1.2 Therapie . .4 1.1.3 Gen-Umwelt-Interaktionen und Genomweite Assoziationsstudien5 1.2 Das neue Asthma-Risikogen ORMDL . .8 1.3 Der β2-Adrenorezeptor . 11 1.4 Protein-Protein-Interaktionen . 13 1.4.1 Biolumineszenz-Resonanz-Energie-Transfer . 15 1.5 Zielsetzung der Arbeit . 18 2 Material und Methoden 19 2.1 Material . 19 2.1.1 Laborgeräte . 19 2.1.2 Allgemeine Verbrauchsmaterialien, Chemikalien und Reagenzien . 21 2.1.3 Lösungen, Reagenzien-Kits und Puffer . 26 2.1.4 Medium . 28 2.1.5 Zelllinien und Bakterienstämme . 28 2.1.6 Antikörper . 29 2.1.7 β-Sympathomimetika . 29 2.1.8 Restriktionsenzyme . 30 2.1.9 Vektoren und DNA . -

Identification of Expression Qtls Targeting Candidate Genes For
ISSN: 2378-3648 Salleh et al. J Genet Genome Res 2018, 5:035 DOI: 10.23937/2378-3648/1410035 Volume 5 | Issue 1 Journal of Open Access Genetics and Genome Research RESEARCH ARTICLE Identification of Expression QTLs Targeting Candidate Genes for Residual Feed Intake in Dairy Cattle Using Systems Genomics Salleh MS1,2, Mazzoni G2, Nielsen MO1, Løvendahl P3 and Kadarmideen HN2,4* 1Department of Veterinary and Animal Sciences, Faculty of Health and Medical Sciences, University of Copenhagen, Denmark Check for 2Department of Bio and Health Informatics, Technical University of Denmark, Lyngby, Denmark updates 3Department of Molecular Biology and Genetics-Center for Quantitative Genetics and Genomics, Aarhus University, AU Foulum, Tjele, Denmark 4Department of Applied Mathematics and Computer Science, Technical University of Denmark, Lyngby, Denmark *Corresponding author: Kadarmideen HN, Department of Applied Mathematics and Computer Science, Technical University of Denmark, DK-2800, Kgs. Lyngby, Denmark, E-mail: [email protected] Abstract body weight gain and net merit). The eQTLs and biological pathways identified in this study improve our understanding Background: Residual feed intake (RFI) is the difference of the complex biological and genetic mechanisms that de- between actual and predicted feed intake and an important termine FE traits in dairy cattle. The identified eQTLs/genet- factor determining feed efficiency (FE). Recently, 170 can- ic variants can potentially be used in new genomic selection didate genes were associated with RFI, but no expression methods that include biological/functional information on quantitative trait loci (eQTL) mapping has hitherto been per- SNPs. formed on FE related genes in dairy cows. In this study, an integrative systems genetics approach was applied to map Keywords eQTLs in Holstein and Jersey cows fed two different diets to eQTL, RNA-seq, Genotype, Data integration, Systems improve identification of candidate genes for FE. -

Development of a Genomic Reference Population for Bovine Respiratory Disease in Pre-Weaning Dairy Calves Using Thoracic Ultrasonography
Development of a genomic reference population for bovine respiratory disease in pre-weaning dairy calves using thoracic ultrasonography Allison E. Quick, T.L. Ollivett, M.R. Skiba, A.M. Nuttleman, D.S. Weigel, R.L. Wallace, K.A. Weigel 2 Objectives Establish a protocol for objective and efficient assessment of bovine respiratory disease (BRD) phenotypes in dairy calves to build a large reference population and enable genomic selection for reduced incidence and severity Specific Aim 1: Identify markers associated with BRD in a genome wide association study using the established reference population Specific Aim 2: Estimate genomic breeding values of reference population animals and relatives to facilitate whole genome selection against BRD 3 Establishing a Reference Population . 1107 Holstein calves . 6 dairy farms in southern Wisconsin . 4 trained evaluators . Data collection from May to August 2017 . Each calf measured at 3-weeks and 6-weeks of age . Clinical Disease Scoring . UW-Madison Vet Med Calf Health Scorer iPad tool . Subclinical Disease Scoring . Thoracic Ultrasound (TUS) Evaluation 4 Clinical Scoring . Sensitivity = 62% . Specificity = 74% . Compared with gold standard post-mortem evaluation (Buczinski et al., 2015) https://www.vetmed.wisc.edu/dms/fapm/fapmtools/calves.htm 5 Subclinical Scoring: TUS . Sensitivity = 94% . Specificity = 100% . Compared with gold standard post-mortem evaluation (Ollivett et al, 2015) . 0 to 5 Scale (4 and 5 are multiple consolidated lobes) Score 0: Normal lung Score 2: Lesion > 1cm Score 3: Consolidated lobe 6 Overall BRD Scores Example: Calf 19893 Clinical Scores: Cough = 2 Temperature = 3 Subclinical Score: Ultrasound = 5 Overall BRD Score: 6 Clinical Lobar Pneumonia 7 Frequency using Overall BRD Scores 3-Week 6-Week Incidence Rate Incidence Rate (%) (%) Healthy (1) 81.1 77.1 Upper Respiratory Tract Infection (2) 2.9 2.7 Subclinical Lobular Pneumonia (3) 11.9 12.5 Subclinical Lobar Pneumonia (4) 2.6 5.3 Clinical Lobular Pneumonia (5) 0.8 1.4 Clinical Lobar Pneumonia (6) 0.7 1.0 8 Preliminary Genetic Analysis . -
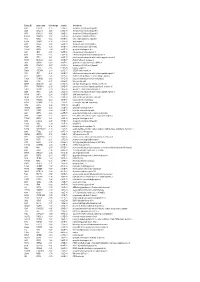
Entrez ID Gene Name Fold Change Q-Value Description
Entrez ID gene name fold change q-value description 4283 CXCL9 -7.25 5.28E-05 chemokine (C-X-C motif) ligand 9 3627 CXCL10 -6.88 6.58E-05 chemokine (C-X-C motif) ligand 10 6373 CXCL11 -5.65 3.69E-04 chemokine (C-X-C motif) ligand 11 405753 DUOXA2 -3.97 3.05E-06 dual oxidase maturation factor 2 4843 NOS2 -3.62 5.43E-03 nitric oxide synthase 2, inducible 50506 DUOX2 -3.24 5.01E-06 dual oxidase 2 6355 CCL8 -3.07 3.67E-03 chemokine (C-C motif) ligand 8 10964 IFI44L -3.06 4.43E-04 interferon-induced protein 44-like 115362 GBP5 -2.94 6.83E-04 guanylate binding protein 5 3620 IDO1 -2.91 5.65E-06 indoleamine 2,3-dioxygenase 1 8519 IFITM1 -2.67 5.65E-06 interferon induced transmembrane protein 1 3433 IFIT2 -2.61 2.28E-03 interferon-induced protein with tetratricopeptide repeats 2 54898 ELOVL2 -2.61 4.38E-07 ELOVL fatty acid elongase 2 2892 GRIA3 -2.60 3.06E-05 glutamate receptor, ionotropic, AMPA 3 6376 CX3CL1 -2.57 4.43E-04 chemokine (C-X3-C motif) ligand 1 7098 TLR3 -2.55 5.76E-06 toll-like receptor 3 79689 STEAP4 -2.50 8.35E-05 STEAP family member 4 3434 IFIT1 -2.48 2.64E-03 interferon-induced protein with tetratricopeptide repeats 1 4321 MMP12 -2.45 2.30E-04 matrix metallopeptidase 12 (macrophage elastase) 10826 FAXDC2 -2.42 5.01E-06 fatty acid hydroxylase domain containing 2 8626 TP63 -2.41 2.02E-05 tumor protein p63 64577 ALDH8A1 -2.41 6.05E-06 aldehyde dehydrogenase 8 family, member A1 8740 TNFSF14 -2.40 6.35E-05 tumor necrosis factor (ligand) superfamily, member 14 10417 SPON2 -2.39 2.46E-06 spondin 2, extracellular matrix protein 3437 -

RNA Sequencing Analyses Reveal Differentially Expressed Genes and Pathways As Notch2 Targets in B-Cell Lymphoma
www.oncotarget.com Oncotarget, 2020, Vol. 11, (No. 48), pp: 4527-4540 Research Paper RNA sequencing analyses reveal differentially expressed genes and pathways as Notch2 targets in B-cell lymphoma Ashok Arasu1, Pavithra Balakrishnan1 and Thirunavukkarasu Velusamy1 1Department of Biotechnology, School of Biotechnology and Genetic Engineering, Bharathiar University, Coimbatore, India Correspondence to: Thirunavukkarasu Velusamy, email: [email protected] Keywords: SMZL; Notch2; RNA sequencing; PI3K/AKT; NF-kB Received: August 04, 2020 Accepted: October 17, 2020 Published: December 01, 2020 Copyright: © 2020 Arasu et al. This is an open access article distributed under the terms of the Creative Commons Attribution License (CC BY 3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. ABSTRACT Splenic marginal zone lymphoma (SMZL) is a low grade, indolent B-cell neoplasm that comprises approximately 10% of all lymphoma. Notch2, a pivotal gene for marginal zone differentiation is found to be mutated in SMZL. Deregulated Notch2 signaling has been involved in tumorigenesis and also in B-cell malignancies. However the role of Notch2 and the downstream pathways that it influences for development of B-cell lymphoma remains unclear. In recent years, RNA sequencing (RNA-Seq) has become a functional and convincing technology for profiling gene expression and to discover new genes and transcripts that are involved in disease development in a single experiment. In the present study, using transcriptome sequencing approach, we have identified key genes and pathways that are probably the underlying cause in the development of B-cell lymphoma. We have identified a total of 15,083 differentially expressed genes (DEGs) and 1067 differentially expressed transcripts (DETs) between control and Notch2 knockdown B cells. -

Supplemental Information
1 1 Supplemental Information 2 3 Materials & Methods 4 Organisms. Anemones of the clonal Aiptasia strains CC7 (53) and H2 (54) were used 5 in this study, with H2 animals used only in the crosses to produce larvae for 6 transcriptome analyses (see below). Although CC7 and H2 have been described 7 previously as A. pallida and A. pulchella, respectively, recent global genotyping has 8 found two genetically distinct Aiptasia populations that do not conform to previous 9 species descriptions (5). Thus, we refer to both strains simply as Aiptasia in this paper. 10 Anemones were grown as described previously (19). Briefly, animals were raised in 11 a circulating artificial seawater (ASW) system at ~25ºC with 20-40 µmol photons m-2 s-1 12 of photosynthetically active radiation on a 12 h:12 h light:dark cycle and fed freshly 13 hatched Artemia (brine-shrimp) nauplii approximately twice per week. To generate 14 aposymbiotic anemones (i.e., animals without dinoflagellate symbionts), anemones were 15 placed in a polycarbonate tub and subjected to multiple repetitions of the following cycle: 16 cold-shocking by addition of 4ºC ASW and incubation at 4ºC for 4 h, followed by 1-2 d at 17 ~25ºC in ASW containing the photosynthesis inhibitor diuron (Sigma-Aldrich #D2425) at 18 50 µM (lighting approximately as above). The putatively aposymbiotic anemones were 19 then maintained for ≥1 month in ASW at ~25ºC in the light (as above) with feeding (as 20 above, with water changes on the days following feeding) to test for possible 21 repopulation of the animals by any residual dinoflagellates. -

A Molecular Model for Neurodevelopmental Disorders
OPEN Citation: Transl Psychiatry (2015) 5, e565; doi:10.1038/tp.2015.56 www.nature.com/tp ORIGINAL ARTICLE A molecular model for neurodevelopmental disorders CO Gigek1,2, ES Chen1,2,VKOta1, G Maussion, H Peng, K Vaillancourt, AB Diallo, JP Lopez, L Crapper, C Vasuta, GG Chen and C Ernst Genes implicated in neurodevelopmental disorders (NDDs) important in cognition and behavior may have convergent function and several cellular pathways have been implicated, including protein translational control, chromatin modification, and synapse assembly and maintenance. Here, we test the convergent effects of methyl-CpG binding domain 5 (MBD5) and special AT-rich binding protein 2 (SATB2) reduced dosage in human neural stem cells (NSCs), two genes implicated in 2q23.1 and 2q33.1 deletion syndromes, respectively, to develop a generalized model for NDDs. We used short hairpin RNA stably incorporated into healthy neural stem cells to supress MBD5 and SATB2 expression, and massively parallel RNA sequencing, DNA methylation sequencing and microRNA arrays to test the hypothesis that a primary etiology of NDDs is the disruption of the balance of NSC proliferation and differentiation. We show that reduced dosage of either gene leads to significant overlap of gene-expression patterns, microRNA patterns and DNA methylation states with control NSCs in a differentiating state, suggesting that a unifying feature of 2q23.1 and 2q33.1 deletion syndrome may be a lack of regulation between proliferation and differentiation in NSCs, as we observed previously for TCF4 and EHMT1 suppression following a similar experimental paradigm. We propose a model of NDDs whereby the balance of NSC proliferation and differentiation is affected, but where the molecules that drive this effect are largely specific to disease-causing genetic variation. -
PINTO-DISSERTATION-2014.Pdf
In vitro assays and zebrafish as an in vivo model to study nuclear receptor signaling _______________ A Dissertation Presented to The Faculty of the Department of Biology and Biochemistry University of Houston _______________ In Partial Fulfillment Of the Requirements for the Degree of Doctor of Philosophy _______________ By Caroline Lucia Pinto August, 2014 In vitro assays and zebrafish as an in vivo model to study nuclear receptor signaling _________________________ Caroline Lucia Pinto APPROVED: __________________________ Dr. Jan-Åke Gustafsson, Ph.D. Committee Chair ___________________________ Dr. Maria Bondesson Bolin, Ph.D. ___________________________ Dr. Robert Fox, Ph.D. ___________________________ Dr. Joseph Eichberg, Ph.D. ___________________________ Dr. Steven Bark, PhD. ___________________________ Dr. Paul Webb, PhD. _________________________ Dr. Dan Wells, Ph.D. Dean, College of Natural Sciences and Mathematics ii Acknowledgements This achievement would not have been possible without the help and encouragement from many people that I was blessed to meet during my Ph.D. I would like to start by thanking the Department of Biology and Biochemistry at University of Houston for allowing me to join the Ph.D. program, and be a part of this diverse academic community. I would like to thank Dr. Jan-Ake Gustafsson for the opportunity of joining the Center for Nuclear Receptors and Cell Signaling (CNRCS) and for his guidance and support throughout my Ph.D. I am grateful to Dr. Maria Bondesson for her support, kindness and encouragement with my projects, and for guiding me to become an autonomous scientist. I thank Dr. Anne Riu for her guidance, patience and always well-appreciated discussions and criticism, and for fostering critical thinking in me. -
Integrated Functional Genomic Analysis Enables Annotation of Kidney Genome-Wide Association Study Loci
BASIC RESEARCH www.jasn.org Integrated Functional Genomic Analysis Enables Annotation of Kidney Genome-Wide Association Study Loci Karsten B. Sieber,1 Anna Batorsky,2 Kyle Siebenthall,2 Kelly L. Hudkins,3 Jeff D. Vierstra,2 Shawn Sullivan,4 Aakash Sur,4,5 Michelle McNulty,6 Richard Sandstrom,2 Alex Reynolds,2 Daniel Bates,2 Morgan Diegel,2 Douglass Dunn,2 Jemma Nelson,2 Michael Buckley,2 Rajinder Kaul,2 Matthew G. Sampson,6 Jonathan Himmelfarb,7,8 Charles E. Alpers,3,8 Dawn Waterworth,1 and Shreeram Akilesh3,8 Due to the number of contributing authors, the affiliations are listed at the end of this article. ABSTRACT Background Linking genetic risk loci identified by genome-wide association studies (GWAS) to their causal genes remains a major challenge. Disease-associated genetic variants are concentrated in regions con- taining regulatory DNA elements, such as promoters and enhancers. Although researchers have previ- ously published DNA maps of these regulatory regions for kidney tubule cells and glomerular endothelial cells, maps for podocytes and mesangial cells have not been available. Methods We generated regulatory DNA maps (DNase-seq) and paired gene expression profiles (RNA-seq) from primary outgrowth cultures of human glomeruli that were composed mainly of podo- cytes and mesangial cells. We generated similar datasets from renal cortex cultures, to compare with those of the glomerular cultures. Because regulatory DNA elements can act on target genes across large genomic distances, we also generated a chromatin conformation map from freshly isolated human glomeruli. Results We identified thousands of unique regulatory DNA elements, many located close to transcription factor genes, which the glomerular and cortex samples expressed at different levels. -
Prenatal Diagnosis of a Maternal 7.22-Mb Deletion at Chromosome 4Q32.2Q32.3 by SNP Array Pingping Zhang, Yanmei Sun, Ping Huo, Haishen Tian, Jian Gao* and Yali Li*
Zhang et al. Molecular Cytogenetics (2020) 13:12 https://doi.org/10.1186/s13039-020-00480-8 CASE REPORT Open Access Prenatal diagnosis of a maternal 7.22-Mb deletion at chromosome 4q32.2q32.3 by SNP array Pingping Zhang, Yanmei Sun, Ping Huo, Haishen Tian, Jian Gao* and Yali Li* Abstract Background: Although Chromosomal microarray analysis (CMA) is a powerful diagnostic technology for detecting chromosomal copy number variants (CNVs), it detects numerous variants of unknown significance (VUSs), which poses a great challenge for genetic counselling. Terminal deletion of the long arm of chromosome 4 is a rare genetic aberration. Few cases of interstitial deletion sharing the common deleted segment have been reported. Case presentation: A male foetus with a 7.22-Mb deletion at chromosome 4q32.2q32.3 was found in the proband. The paternal genotype was normal. His asymptomatic mother with a normal phenotype and intelligence was found to carry the same deletion at the long arm of chromosome 4. The clinical significance of arr[GRCh37] 4q32.2q32.3(162858958_ 170081268)×1 remains uncertain. To the best of our knowledge, this is the first case report on a VUS of 4q32 deletion and the second report of a heterochromatic CNV involving part of the long arm of chromosome 4 in a phenotypically normal mother and child. The identification of this case contributes to additional understanding of deletion at 4q32.2q32.3. This report may provide a reference for prenatal diagnosis and genetic counselling in patients who have genotypes of similar cytogenetic abnormalities. Conclusions: The novel 7.22-Mb deletion at chromosome 4q32.2q32.3 (162858958-170081268) is a VUS. -

Gene Modules Associated with Human Diseases Revealed by Network
bioRxiv preprint doi: https://doi.org/10.1101/598151; this version posted June 15, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Gene modules associated with human diseases revealed by network analysis Shisong Ma1,2*, Jiazhen Gong1†, Wanzhu Zuo1†, Haiying Geng1, Yu Zhang1, Meng Wang1, Ershang Han1, Jing Peng1, Yuzhou Wang1, Yifan Wang1, Yanyan Chen1 1. Hefei National Laboratory for Physical Sciences at the Microscale, School of Life Sciences, University of Science and Technology of China, Hefei, Anhui 230027, China 2. School of Data Science, University of Science and Technology of China, Hefei, Anhui 230027, China * To whom correspondence should be addressed. Email: [email protected] † These authors contribute equally. 1 bioRxiv preprint doi: https://doi.org/10.1101/598151; this version posted June 15, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. ABSTRACT Despite many genes associated with human diseases have been identified, disease mechanisms often remain elusive due to the lack of understanding how disease genes are connected functionally at pathways level. Within biological networks, disease genes likely map to modules whose identification facilitates etiology studies but remains challenging. We describe a systematic approach to identify disease-associated gene modules.