OHIP Dental Schedule
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Lumps and Swellings
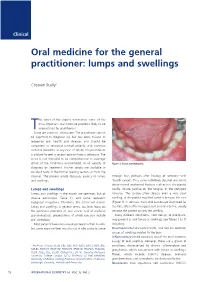
Clinical Oral medicine for the general practitioner: lumps and swellings Crispian Scully 1 his series of five papers summarises some of the most important oral medicine problems likely to be Tencountered by practitioners. Some are common, others rare. The practitioner cannot be expected to diagnose all, but has been trained to recognise oral health and disease, and should be competent to recognise normal variants, and common orofacial disorders. In any case of doubt, the practitioner is advised to seek a second opinion from a colleague. The series is not intended to be comprehensive in coverage either of the conditions encountered, or all aspects of Figure 1: Torus mandibularis. diagnosis or treatment: further details are available in standard texts, in the further reading section, or from the internet. The present article discusses aspects of lumps through fear, perhaps after hearing of someone with and swellings. ‘mouth cancer’. Thus some individuals discover and worry about normal anatomical features such as tori, the parotid Lumps and swellings papilla, foliate papillae on the tongue, or the pterygoid Lumps and swellings in the mouth are common, but of hamulus. The tongue often detects even a very small diverse aetiologies (Table 1), and some represent swelling, or the patient may first notice it because it is sore malignant neoplasms. Therefore, this article will discuss (Figure 1). In contrast, many oral cancers are diagnosed far lumps and swellings in general terms, but later focus on too late, often after being present several months, usually the particular problems of oral cancer and of orofacial because the patient ignores the swelling. -

ISSN: 2320-5407 Int. J. Adv. Res. 7(10), 979-1021
ISSN: 2320-5407 Int. J. Adv. Res. 7(10), 979-1021 Journal Homepage: - www.journalijar.com Article DOI: 10.21474/IJAR01/9916 DOI URL: http://dx.doi.org/10.21474/IJAR01/9916 RESEARCH ARTICLE MINOR ORAL SURGICAL PROCEDURES. Harsha S K., Rani Somani and Shipra Jaidka. 1. Postgraduate Student, Department of Pediatric and Preventive Dentistry, Divya Jyoti college of Dental Sciences & Research, Modinagar, UP, India. 2. Professor and Head of the Department, Department of Pediatric and Preventive Dentistry, Divya Jyoti College of Dental Sciences & Research, Modinagar, UP, India. 3. Professor, Department of Pediatric and Preventive Dentistry, Divya Jyoti College of Dental Sciences & Research, Modinagar, UP, India. ……………………………………………………………………………………………………………………….... Manuscript Info Abstract ……………………. ……………………………………………………………… Manuscript History Minor oral surgery includes removal of retained or burried roots, Received: 16 August 2019 broken teeth, wisdom teeth and cysts of the upper and lower jaw. It also Final Accepted: 18 September 2019 includes apical surgery and removal of small soft tissue lesions like Published: October 2019 mucocele, ranula, high labial or lingual frenum etc in the mouth. These procedures are carried out under local anesthesia with or without iv Key words:- Gamba grass, accessions, yield, crude sedation and have relatively short recovery period. protein, mineral contents, Benin. Copy Right, IJAR, 2019,. All rights reserved. …………………………………………………………………………………………………….... Introduction:- Children are life‟s greatest gifts. The joy, curiosity and energy all wrapped up in tiny humans. This curiosity and lesser motor coordination usually leads to increased incidence of falls in children which leads to traumatic dental injuries. Trauma to the oral region may damage teeth, lips, cheeks, tongue, and temporomandibular joints. These traumatic injuries are the second most important issue in dentistry, after the tooth decay. -

WHAT HAPPENED? CDR, a 24-Year-Old Chinese Male
CHILDHOOD DEVELOPMENTAL SCREENING 2020 https://doi.org/10.33591/sfp.46.5.up1 FINDING A MASS WITHIN THE ORAL CAVITY: WHAT ARE THE COMMON CAUSES AND 4-7 GAINING INSIGHT: WHAT ARE THE ISSUES? In Figure 2 below, a list of masses that could arise from each site Figure 3. Most common oral masses What are the common salivary gland pathologies Salivary gland tumours (Figure 7) commonly present as channel referrals to appropriate specialists who are better HOW SHOULD A GP MANAGE THEM? of the oral cavity is given and elaborated briey. Among the that a GP should be aware of? painless growing masses which are usually benign. ey can equipped in centres to accurately diagnose and treat these Mr Tan Tai Joum, Dr Marie Stella P Cruz CDR had a slow-growing mass in the oral cavity over one year more common oral masses are: torus palatinus, torus occur in both major and minor salivary glands but are most patients, which usually involves surgical excision. but sought treatment only when he experienced a sudden acute mandibularis, pyogenic granuloma, mucocele, broma, ere are three pairs of major salivary glands (parotid, commonly found occurring in the parotid glands. e most 3) Salivary gland pathology may be primary or secondary to submandibular and sublingual) as well as hundreds of minor ABSTRACT onset of severe pain and numbness. He was fortunate to have leukoplakia and squamous cell carcinoma – photographs of common type of salivary gland tumour is the pleomorphic systemic causes. ese dierent diseases may present with not sought treatment as it had not caused any pain. -

Abscesses Apicectomy
BChD, Dip Odont. (Mondchir.) MBChB, MChD (Chir. Max.-Fac.-Med.) Univ. of Pretoria Co Reg: 2012/043819/21 Practice.no: 062 000 012 3323 ABSCESSES WHAT IS A TOOTH ABSCESS? A dental/tooth abscess is a localised acute infection at the base of a tooth, which requires immediate attention from your dentist. They are usually associated with acute pain, swelling and sometimes an unpleasant smell or taste in the mouth. More severe infections cause facial swelling as the bacteria spread to the nearby tissues of the face. This is a very serious condition. Once the swelling begins, it can spread rapidly. The pain is often made worse by drinking hot or cold fluids or biting on hard foods and may spread from the tooth to the ear or jaw on the same side. WHAT CAUSES AN ABSCESS? Damage to the tooth, an untreated cavity, or a gum disease can cause an abscessed tooth. If the cavity isn’t treated, the inside of the tooth can become infected. The bacteria can spread from the tooth to the tissue around and beneath it, creating an abscess. Gum disease causes the gums to pull away from the teeth, leaving pockets. If food builds up in one of these pockets, bacteria can grow, and an abscess may form. An abscess can cause the bone around the tooth to dissolve. WHY CAN'T ANTIBIOTIC TREATMENT ALONE BE USED? Antibiotics will usually help the pain and swelling associated with acute dental infections. However, they are not very good at reaching into abscesses and killing all the bacteria that are present. -

Recognition and Management of Oral Health Problems in Older Adults by Physicians: a Pilot Study
J Am Board Fam Pract: first published as 10.3122/jabfm.11.6.474 on 1 November 1998. Downloaded from BRIEF REPORTS Recognition and Management of Oral Health Problems in Older Adults by Physicians: A Pilot Study Thomas V. Jones, MD, MPH, Mitchel J Siegel, DDS, andJohn R. Schneider, A1A Oral health problems are among the most com of the nation's current and future health care mon chronic health conditions experienced by needs, the steady increase in the older adult popu older adults. Healthy People 2000, an initiative to lation, and the generally high access elderly per improve the health of America, has selected oral sons have to medical care provided by family health as a priority area. l About 11 of 100,000 physicians and internists.s,7,8 Currently there is persons have oral cancer diagnosed every year.2 very little information about the ability of family The average age at which oral cancer is diagnosed physicians or internists, such as geriatricians, to is approximately 65 years, with the incidence in assess the oral health of older patients. We con creasing from middle adulthood through the sev ducted this preliminary study to determine how enth decade of life. l-3 Even though the mortality family physicians and geriatricians compare with rate associated with oral cancer (7700 deaths an each other and with general practice dentists in nually)4 ranks among the lowest compared with their ability to recognize, diagnose, and perform other cancers, many deaths from oral cancer initial management of a wide spectrum of oral might be prevented by improved case finding and health problems seen in older adults. -

Management of Ankylogossia by Frenectomy- a Case Report
British Journal of Medicine & Medical Research 18(8): 1-5, 2016, Article no.BJMMR.28162 ISSN: 2231-0614, NLM ID: 101570965 SCIENCEDOMAIN international www.sciencedomain.org Management of Ankylogossia by Frenectomy- A Case Report Meghna Singh1, Ashish Saini2*, Pranav Kumar Singh2, Charu Tandon2, Snehlata Verma3 and Tanu Tewari4 1Department of Pedodontics, BBD College of Dental Sciences, Lucknow, India. 2Department of Periodontics, BBD College of Dental Sciences, Lucknow, India. 3Department of Orthodontics and Dentofacial Orthopedics, BBD College of Dental Sciences, Lucknow, India. 4Department of Conservative Denstistry and Endodontics, BBD College of Dental Sciences, Lucknow, India. Authors’ contributions This surgery was carried out by authors MS and AS. Author PKS wrote the first draft of the manuscript. Authors CT and SV managed the literature searches. Author TT managed the final draft. All authors read and approved the final manuscript. Article Information DOI: 10.9734/BJMMR/2016/28162 Editor(s): (1) Joao Paulo Steffens, Department of Stomatology, Universidade Federal do Parana, Brazil. (2) Emad Tawfik Mahmoud Daif, Professor of Oral & Maxillofacial Surgery, Cairo University, Egypt. (3) James Anthony Giglio, Adjunct Clinical Professor of Oral and Maxillofacial Surgery, School of Dentistry, Virginia Commonwealth University, Virginia, USA. (4) Philippe E. Spiess, Department of Genitourinary Oncology, Moffitt Cancer Center, USA and Department of Urology and Department of Oncologic Sciences (Joint Appointment), College of Medicine, University of South Florida, Tampa, FL, USA. Reviewers: (1) Kritika Jangid, Saveetha Dental College, India. (2) Jaspreet Singh Gill, Desh BhagatDental College & Hospital, Muktsar, Punjab. Baba Farid University of Health Sciences, Faridkot, Punjab, India. (3) Vishal Mehrotra, Rama University of Health Scemces, Kanpur, India. -

Aadsm Annual Meeting San Antonio: June 7-919
AADSM ANNUAL MEETING SAN ANTONIO: JUNE 7-919 FINAL PROGRAM WELCOME to the 2019 AADSM Annual Meeting 2 This year’s meeting features: • Three rooms of general sessions on Saturday and Sunday – Fundamentals, Clinical Applications and Advances in DSM; • Poster presentations, located just outside of the exhibit hall, including new “late-breaking abstracts;” • Lunch presentations from vendors during the industry product theatres on Saturday; • A lounge for Diplomates of the ABDSM and dental directors of AADSM-accredited facilities to network; and • Special sessions for dentists on faculty at dental schools, interested in performing clinical research, looking for information on getting more involved with the AADSM. Information about these opportunities can be found in the pages of this final program. I have no doubt that this year’s meeting will offer you the opportunity to renew and initiate relationships with colleagues from around the world while expanding your knowledge of dental sleep medicine. Enjoy, Sheri Katz, DDS Chair, Annual Meeting Committee AADSM ANNUAL MEETING SAN ANTONIO: JUNE 7-919 ON-SITE REGISTRATION HOURS EXHIBIT HALL HOURS Salon A- F Friday, June 7 6:30am – 5:30pm Saturday, June 8 7:00am – 5:00pm Friday, June 7 10:00am – 4:00pm Sunday, June 9 7:00am – 1:30pm Saturday, June 8 10:00am – 4:00pm Sunday, June 9 10:00am – 12:30pm The registration desk is located in the Salon Ballroom Foyer of the Marriott Rivercenter. Learn about the newest products and services in the field by visiting Your registration includes admission to: the exhibit hall! The AADSM Annual • General Sessions (Friday-Sunday) Meeting exhibit hall showcases oral appliance manufacturers, • President’s Reception dental laboratories, software • Industry Supported Events companies and more. -

Treatments for Ankyloglossia and Ankyloglossia with Concomitant Lip-Tie Comparative Effectiveness Review Number 149
Comparative Effectiveness Review Number 149 Treatments for Ankyloglossia and Ankyloglossia With Concomitant Lip-Tie Comparative Effectiveness Review Number 149 Treatments for Ankyloglossia and Ankyloglossia With Concomitant Lip-Tie Prepared for: Agency for Healthcare Research and Quality U.S. Department of Health and Human Services 540 Gaither Road Rockville, MD 20850 www.ahrq.gov Contract No. 290-2012-00009-I Prepared by: Vanderbilt Evidence-based Practice Center Nashville, TN Investigators: David O. Francis, M.D., M.S. Sivakumar Chinnadurai, M.D., M.P.H. Anna Morad, M.D. Richard A. Epstein, Ph.D., M.P.H. Sahar Kohanim, M.D. Shanthi Krishnaswami, M.B.B.S., M.P.H. Nila A. Sathe, M.A., M.L.I.S. Melissa L. McPheeters, Ph.D., M.P.H. AHRQ Publication No. 15-EHC011-EF May 2015 This report is based on research conducted by the Vanderbilt Evidence-based Practice Center (EPC) under contract to the Agency for Healthcare Research and Quality (AHRQ), Rockville, MD (Contract No. 290-2012-00009-I). The findings and conclusions in this document are those of the authors, who are responsible for its contents; the findings and conclusions do not necessarily represent the views of AHRQ. Therefore, no statement in this report should be construed as an official position of AHRQ or of the U.S. Department of Health and Human Services. The information in this report is intended to help health care decisionmakers—patients and clinicians, health system leaders, and policymakers, among others—make well-informed decisions and thereby improve the quality of health care services. This report is not intended to be a substitute for the application of clinical judgment. -

Oral Health and Disease
Downloaded from bmj.com on 19 August 2005 ABC of oral health: Oral health and disease Ruth Holt, Graham Roberts and Crispian Scully BMJ 2000;320;1652-1655 doi:10.1136/bmj.320.7250.1652 Updated information and services can be found at: http://bmj.com/cgi/content/full/320/7250/1652 These include: Rapid responses One rapid response has been posted to this article, which you can access for free at: http://bmj.com/cgi/content/full/320/7250/1652#responses You can respond to this article at: http://bmj.com/cgi/eletter-submit/320/7250/1652 Email alerting Receive free email alerts when new articles cite this article - sign up in the box at service the top right corner of the article Topic collections Articles on similar topics can be found in the following collections Dentistry and Oral Medicine (79 articles) Notes To order reprints of this article go to: http://www.bmjjournals.com/cgi/reprintform To subscribe to BMJ go to: http://bmj.bmjjournals.com/subscriptions/subscribe.shtml Clinical review Downloaded from bmj.com on 19 August 2005 ABC of oral health Oral health and disease Ruth Holt, Graham Roberts, Crispian Scully A healthy dentition and mouth is important to both quality of life and nutrition, and oral disease may affect systemic health, as Enamel covering crown Gingival crevice discussed in later articles in this series. (gingival sulcus) Dentine Development of the dentition Gingiva Pulp chamber Teeth form mainly from neuroectoderm and comprise a crown of insensitive enamel surrounding sensitive dentine and a root Periodontal ligament that has no enamel covering. -

Icd-9-Cm (2010)
ICD-9-CM (2010) PROCEDURE CODE LONG DESCRIPTION SHORT DESCRIPTION 0001 Therapeutic ultrasound of vessels of head and neck Ther ult head & neck ves 0002 Therapeutic ultrasound of heart Ther ultrasound of heart 0003 Therapeutic ultrasound of peripheral vascular vessels Ther ult peripheral ves 0009 Other therapeutic ultrasound Other therapeutic ultsnd 0010 Implantation of chemotherapeutic agent Implant chemothera agent 0011 Infusion of drotrecogin alfa (activated) Infus drotrecogin alfa 0012 Administration of inhaled nitric oxide Adm inhal nitric oxide 0013 Injection or infusion of nesiritide Inject/infus nesiritide 0014 Injection or infusion of oxazolidinone class of antibiotics Injection oxazolidinone 0015 High-dose infusion interleukin-2 [IL-2] High-dose infusion IL-2 0016 Pressurized treatment of venous bypass graft [conduit] with pharmaceutical substance Pressurized treat graft 0017 Infusion of vasopressor agent Infusion of vasopressor 0018 Infusion of immunosuppressive antibody therapy Infus immunosup antibody 0019 Disruption of blood brain barrier via infusion [BBBD] BBBD via infusion 0021 Intravascular imaging of extracranial cerebral vessels IVUS extracran cereb ves 0022 Intravascular imaging of intrathoracic vessels IVUS intrathoracic ves 0023 Intravascular imaging of peripheral vessels IVUS peripheral vessels 0024 Intravascular imaging of coronary vessels IVUS coronary vessels 0025 Intravascular imaging of renal vessels IVUS renal vessels 0028 Intravascular imaging, other specified vessel(s) Intravascul imaging NEC 0029 Intravascular -

QUICK ORAL HEALTH FACTS ABOUT the YOUNG Dr Ng Jing Jing, Dr Wong Mun Loke
ORAL health IN PRIMARY CARE UNIT NO. 2 QUICK ORAL HEALTH FACTS ABOUT THE YOUNG Dr Ng Jing Jing, Dr Wong Mun Loke ABSTRACT Table 1. Eruption sequence of Primary Dentition This article sheds light on the sequence of teeth eruption Primary Upper Teeth Primary Lower Teeth in the young and teething problems; highlights the importance and functions of the primary dentition and Central Incisors: 8-13 months Central Incisors: 6-10 months provides a quick overview of common developmental Lateral Incisors: 8-13 months Lateral Incisors: 10-16 months dental anomalies and other dental conditions in Canines: 16-23 months Canines: 16-23 months children. First Molars: 16-23 months First Molars: 13-19 months Second Molars: 25-33 months Second Molars: 23-31 months SFP2011; 37(1) Supplement : 10-13 Table 2. Eruption sequence of Adult Dentition Adult Upper Teeth Adult Lower Teeth INTRODUCTION Central Incisors: 7-8 years Central Incisors: 6-7 years The early years are always full of exciting moments as we observe Lateral Incisors: 8-9 years Lateral Incisors: 7-8 years our children grow and develop. One of the most noticeable Canines: 11-12 years Canines: 9-10 years aspects of their growth and development is the eruption of First Premolars: 10-11 years First Premolars: 10-11 years teeth. The first sign of a tooth in the mouth never fails to Second Premolars: 11-12 years Second Premolars: 11-12 years attract the attention of the parent and child. For the parent, it First Molars: 6-7 years First Molars: 6-7 years marks an important developmental milestone of the child but Second Molars: 12-13 years Second Molars: 11-13 years for the child, it can be a source of irritation brought on by the Third Molars: 18-25 years Third Molars: 18-25 years whole process of teething. -

Obstructive Sleep Apnea and the Role of Tongue Reduction Surgery in Children with Beckwith-Wiedemann Syndrome (2018)
RESEARCH INSTITUTE Obstructive sleep apnea and the role of tongue reduction surgery in children with Beckwith-Wiedemann syndrome (2018) Christopher M. Cielo, Kelly A. Duffy, Aesha Vyas, Jesse A. Taylor, Jennifer M. Kalish Background Patients with Beckwith-Wiedemann syndrome (BWS) can be affected by a large tongue (macroglossia). Similar to other features of BWS, macroglossia can vary in severity between patients. Studies suggest that children with macroglossia are at an increased risk for obstructive sleep apnea (OSA), a condition that is also highly variable, ranging from mild sleep obstruction to severe respiratory distress. No recommendations regarding OSA management in patients with BWS and macroglossia exist. Purpose This article reviews all available evidence regarding children with Beckwith-Wiedemann Syndrome (BWS) and macroglossia. The prevalence of obstructive sleep apnea (OSA) and management strategies in this population are discussed. Findings Evaluations Children suspected of having BWS and macroglossia should receive the following evaluations. No clear guidelines exist for at what age children should be evaluated. • Clinical Genetics: Any child with a feature suggestive of BWS should be referred to a clinical geneticist, who can evaluate the patient and determine whether the patient meets criteria for a clinical diagnosis of BWS. • Plastic Surgery: Patients with macroglossia should be referred to a plastic surgeon, who can evaluate the size of the tongue to determine whether a tongue reduction surgery is necessary. • Pulmonology: A pulmonologist can evaluate the degree to which the large tongue affects breathing, as an increased tongue size can narrow the airway and cause upper airway obstruction. o Polysomnography (sleep study) is used for evaluation of OSA in children and has been used in certain studies of BWS children to detect the following: moderate- severe OSA, upper airway obstruction, apnea, upper airway resistance, severe desaturation, sleep-disordered breathing, and snoring.