Chapter 7 Chapter 7 the Evolution of Technology: Scientific Method, Engineering Design, & Translational Research
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Huda Y. Zoghbi, MD, Howard Hughes Medical Institute, Jan and Dan Duncan Neurological Research Institute at Texas Children’S Hospital and Baylor College of Medicine
Investigator Spotlight: Huda Y. Zoghbi, MD, Howard Hughes Medical Institute, Jan and Dan Duncan Neurological Research Institute at Texas Children’s Hospital and Baylor College of Medicine It is hard to believe that the 7th World Rett Syndrome Congress has come and gone with great success! Now with summer upon us, IRSF continues to move the spotlight to the committed scientists who have made the World Congress an impressive, high quality meeting with outstanding presentations and discussions. This month we are honored to focus on Dr. Huda Zoghbi who had co-chaired the Basic Research Symposium at the World Congress along with Dr. Gail Mandel. Together, they had produced an exciting lineup of speakers who were encouraged to present new, unpublished data in an effort to foster new ideas that will help chart the course for Rett syndrome research. Dr. Zoghbi is a Howard Hughes Medical Institute (HHMI) Investigator, the Director of the Jan and Dan Duncan Neurological Research Institute at Texas Children’s Hospital, and Professor of the Baylor College of Medicine in Houston, TX. She received her medical degree from Meharry Medical College and completed residency training in pediatrics and neurology at Baylor College of Medicine where she encountered her first Rett syndrome patient in 1983. Dr. Zoghbi was inspired to receive additional research training in the area molecular genetics and upon completion she joined the faculty of Baylor College of Medicine. In 1999, Dr. Zoghbi and collaborators including research fellow Ruthie Amir made a major breakthrough for Rett syndrome. They had discovered that mutations in MECP2, the gene encoding methyl-CpG-binding protein 2, causes Rett syndrome. -

UC San Diego UC San Diego Electronic Theses and Dissertations
UC San Diego UC San Diego Electronic Theses and Dissertations Title Spinocerebellar Ataxia Type 7 is Characterized by Defects in Mitochondrial and Metabolic Function Permalink https://escholarship.org/uc/item/02b7m809 Author Ward, Jacqueline Marie Publication Date 2016 Supplemental Material https://escholarship.org/uc/item/02b7m809#supplemental Peer reviewed|Thesis/dissertation eScholarship.org Powered by the California Digital Library University of California UNIVERSITY OF CALIFORNIA, SAN DIEGO Spinocerebellar Ataxia Type 7 is Characterized by Defects in Mitochondrial and Metabolic Function A dissertation submitted in partial satisfaction of the requirements for the degree Doctor of Philosophy in Biomedical Sciences by Jacqueline Marie Ward Committee in charge: Professor Albert La Spada, Chair Professor Eric Bennett Professor Lawrence Goldstein Professor Alysson Muotri Professor Miles Wilkinson 2016 Copyright Jacqueline Marie Ward, 2016 All rights reserved The Dissertation of Jacqueline Marie Ward is approved, and it is acceptable in quality and form for publication on microfilm and electronically: Chair University of California, San Diego 2016 iii DEDICATION This work is dedicated to my grandfather, Dr. Wayne Ward, the kindest person I’ve ever known. His memory inspires me to be a better person daily. iv TABLE OF CONTENTS SIGNATURE PAGE .......................................................................................... iii DEDICATION .................................................................................................. -
Program Book
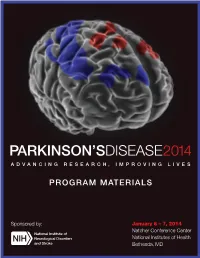
PARKINSON’SDISEASE2014 ADVANCING RESEARCH, IMPROVING LIVES PROGRAM MATERIALS Sponsored by: January 6 – 7, 2014 Natcher Conference Center National Institutes of Health Bethesda, MD About our cover: The program cover image is a stylized version of the Parkinson’s Disease Motor-Related Pattern (PDRP), an abnormal pattern of regional brain function observed in MRI studies which shows increased metabolism indicated by red in some brain regions (pallidothalamic, pontine, and motor cortical areas), and decreased metabolism indicated by blue in others (associated lateral premotor and posterior parietal areas). Original image used with permission of David Eidelberg, M.D. For further information see: Hirano et al., Journal of Neuroscience 28 (16): 4201-4209. Welcome Message from Dr. Story C. Landis Welcome to the National Institute of Neurological Disorders and Stroke (NINDS) conference, “Parkinson’s Disease 2014: Advancing Research, Improving Lives.” Remarkable new discoveries and technological advances are rapidly changing the way we study the biological mechanisms of Parkinson’s disease, identify paths to improved treatments, and design effective clinical trials. Elucidating mechanisms and developing and testing effective interventions require a diverse set of approaches and perspectives. The NINDS has organized this conference with the primary goal of seeking consensus on, and prioritizing, research recommendations spanning clinical, translational, and basic Parkinson’s disease research that we support. We have assembled a stellar and dedicated group of session chairs and panelists who have worked collaboratively to identify emerging research opportunities in Parkinson’s research. While we have divided our working groups into three main research areas, we expect each will inform the others over the course of the next two days, and we look forward to both complementary and unique perspectives. -

Huda Zoghbi: Taking Genetic Inquiry to the Next Level
Spectrum | Autism Research News https://www.spectrumnews.org NEWS, PROFILES Huda Zoghbi: Taking genetic inquiry to the next level BY RACHEL ZAMZOW 25 JUNE 2021 Listen to this story: Most mornings, Huda Zoghbi, 67, climbs a glass-encased, curling staircase to reach her lab on the top and 13th floor of the Jan and Dan Duncan Neurological Research Institute in Houston, Texas. The twisting glass tower, which she designed with a team of architects, echoes the double helix of DNA — a structure that has been central to her career-long quest to uncover genes underlying neurological conditions. As the institute’s director — and as a scientist— she is known for going beyond the standard job description. Genetics researchers often cast a wide net and sequence thousands of genes at a time. But in her prolific career, Zoghbi has focused on a handful of genes, methodically building up an understanding of their function one careful step at a time. Thanks to that approach, Zoghbi has made a number of landmark discoveries, including identifying the genetic roots of Rett syndrome, an autism-related condition that primarily affects girls, as well as the genetic mutations that spur spinocerebellar ataxia, a degenerative motor condition. She has authored more than 350 journal articles. Her accomplishments have earned her almost every major biology and neuroscience research award, including the prestigious Breakthrough Prize in 2017 and the Brain Prize in 2020. “She’s clearly the international leader in the field,” said the late Stephen Warren, professor of human genetics at Emory University in Atlanta, Georgia. Zoghbi never set out to lead a large research center, she says — her heart is in the lab. -
2016 Joint Meeting Program
April 15 – 17, 2016 Fairmont Chicago Millennium Park • Chicago, Illinois The AAP/ASCI/APSA conference is jointly provided by Boston University School of Medicine and AAP/ASCI/APSA. Meeting Program and Abstracts www.jointmeeting.org www.jointmeeting.org Special Events at the 2016 AAP/ASCI/APSA Joint Meeting Friday, April 15 Saturday, April 16 ASCI President’s Reception ASCI Food and Science Evening 6:15 – 7:15 p.m. 6:30 – 9:00 p.m. Gold Room The Mid-America Club, Aon Center ASCI Dinner & New Member AAP Member Banquet Induction Ceremony (Ticketed guests only) (Ticketed guests only) 7:00 – 10:00 p.m. 7:30 – 9:45 p.m. Imperial Ballroom, Level B2 Rouge, Lobby Level How to Solve a Scientific Puzzle: Speaker: Clara D. Bloomfield, MD Clues from Stockholm and Broadway The Ohio State University Comprehensive Cancer Center Speaker: Joe Goldstein, MD APSA Welcome Reception & University of Texas Southwestern Medical Center at Dallas Presidential Address APSA Dinner (Ticketed guests only) 9:00 p.m. – Midnight Signature Room, 360 Chicago, 7:30 – 9:00 p.m. John Hancock Center (off-site) Rouge, Lobby Level Speaker: Daniel DelloStritto, APSA President Finding One’s Scientific Niche: Musings from a Clinical Neuroscientist Speaker: Helen Mayberg, MD, Emory University Dessert Reception (open to all attendees) 10:00 p.m. – Midnight Imperial Foyer, Level B2 Sunday, April 17 APSA Future of Medicine and www.jointmeeting.org Residency Luncheon Noon – 2:00 p.m. Rouge, Lobby Level 2 www.jointmeeting.org Program Contents General Program Information 4 Continuing Medical Education Information 5 Faculty and Speaker Disclosures 7 Scientific Program Schedule 9 Speaker Biographies 16 Call for Nominations: 2017 Harrington Prize for Innovation in Medicine 26 AAP/ASCI/APSA Joint Meeting Faculty 27 Award Recipients 29 Call for Nominations: 2017 Harrington Scholar-Innovator Award 31 Call for Nominations: George M. -
An Eye to the Future Advances in Imaging Are Accelerating the Pace of Biological Discovery
fall 2007 An Eye to the Future Advances in imaging are accelerating the pace of biological discovery. A new cellular imaging initiative at the University has researchers seeing small and thinking big. story on page 8 p r o f i l e s college News c l a s s N o t e s from the dean Where curiosity- and solution- driven science meet ome scientists are driven by a curiosity to under- As a curiosity-driven college, it’s CBS’ job to keep S stand how life works—from molecules to eco- adding to the foundation of knowledge that supports systems—and to add to the world’s collective body of translational and solution-driven science in other col- knowledge. Others are searching for a puzzle piece leges. As such, we are the stewards of the foundational that may yield a better way to treat cancer, produce disciplines in the biological sciences: biochemistry, food or create renewable forms of energy. molecular biology, genetics, cell biology and develop- ment, ecology, plant biology, etc. Both are essential, and there is plenty of overlap Robert Elde, Dean between the two. Curiosity-driven research often turns In order to keep fueling translational and solution- up a bit of information that has immediate applications driven research, we need to infuse foundational disci- in medicine, agriculture or engineering. By the same plines with new technologies and other opportunities token, solution-driven research can add to knowledge. as science evolves. And some scientists travel between these two worlds. Fall 07 Vol. 5 No. 3 Cellular imaging, the subject of our cover story, is one As a whole, College of Biological Sciences faculty of those opportunities. -
View Final Program
142nd ANNUAL MEETING OF THE AMERICAN ANA2017 NEUROLOGICAL ASSOCIATION SAN DIEGO, CA • OCTOBER 15-17, 2017 SHERATON SAN DIEGO HOTEL & MARINA EXPLORE • EXAMINE • INVESTIGATE FINAL PROGRAM OCTOBER 14, 2017 | Pre-Meeting Symposium: Big Science and the BRAIN Initiative 2017.MYANA.org 142nd ANNUAL MEETING OF THE AMERICAN ANA2017 NEUROLOGICAL ASSOCIATION SAN DIEGO, CA • OCTOBER 15 -17, 2017 SHERATON SAN DIEGO HOTEL & MARINA ND Please note some session titles may have changed since this program was printed. Please refer THE 142 ANA to your Mobile app for the most current session updates. ANNUAL MEETING LETTER FROM THE CHAIR 3 Enjoy outstanding scientific SCHEDULE AT A GLANCE 4 symposia covering the latest HOTEL FLOOR PLANS 6 research in the fields of neurology and neuroscience GENERAL INFORMATION 7 while taking the opportunity WIRELESS CONNECTION 8 to network with leaders in the world of academic neurology CONTINUING MEDICAL EDUCATION 8 at the 142nd ANA Annual ANNUAL MEETING MOBILE APP 8 Meeting in San Diego, CA, October 15-17, 2017. PROGRAMS BY DAY 9 SATURDAY OCT 14 9 MEETING LOCATION SUNDAY OCT 15 9 Sheraton San Diego MONDAY OCT 16 17 Hotel & Marina 1380 Harbor Island Drive TUESDAY OCT 17 25 San Diego, California 92101 IN MEMORIAM 28 ONSITE MEETING CONTACTS SPEAKER ABSTRACTS 29 Registration and meeting questions: THANK YOU TO OUR SUPPORTERS & EXHIBITORS 42 [email protected] FUTURE MEETING DATES 42 OR visit the registration desk Bay View Foyer 2017 AWARDEES 43 (located in Marina Tower Lobby Level) ACADEMIC NEUROLOGY REPRESENTATIVES FROM JAPAN 47 Saturday, October 14 2017 ABSTRACT REVIEWERS 48 3:00 PM–7:00 PM BOARD OF DIRECTORS 49 Sunday, October 15 6:00 AM–5:45 PM ANA 2017 COMMITTEES, SUBCOMMITTEES & TASK FORCES 50 Monday, October 16 6:30 AM–5:45 PM Tuesday, October 17 6:30 AM–2:15 PM #ANAMTG2017 ANA 2017 FROM THE CHAIR Dear Colleagues, It is a pleasure to welcome you to the 142nd Annual Meeting of the American Neurological Association (ANA). -

FY 2017 Annual Report July 1, 2016 – June 30, 2017
FY 2017 Annual Report July 1, 2016 – June 30, 2017 A supporting organization of A. Sarah Hreha, Executive Director The Gruber Foundation November 20, 2017 [email protected] The Gruber Foundation FY 2017 Report 1 Executive Summary The Gruber Foundation honors individuals in the fields of Cosmology, Genetics, Neuroscience, Justice, and Women's Rights, whose groundbreaking work provides new models that inspire and enable fundamental shifts in knowledge and culture. The Gruber Foundation is a 509(a)(3) Type 1 supporting organization operated, supervised, or controlled by Yale University and incorporated in 2011 under the 501(c)(3) section of U.S. Corporate Law. It was funded by The Peter and Patricia Gruber Foundation, and Peter and Patricia Gruber were its Co-founders. As President Emeritus, Patricia Gruber A. Sarah Hreha, Executive Director has a lifetime seat on the Board. The Foundation ended its sixth year at Yale with the second Gruber Symposium organized by and for Gruber Science Fellows, in May 2016. Participants ranged from the life sciences to Astronomy, and within fields the topics varied. The third annual Gruber Cosmology Conference at Yale was held in October, and included Kip Thorne and Rainer Weiss, two of the 2016 Cosmology Prize co-recipients, and was attended by over 100 students, faculty and staff. The 2016 Gruber International Prizes were awarded in New York City, Vancouver, Canada, and San Diego, CA. The Prize events are staffed by Gruber Science Fellows in the respective disciplines who generously volunteer to help us honor our recipients. In addition to more mundane logistical tasks, they each have a minute or two to describe their research to a group comprising mostly eminent scientists – their future colleagues. -

2019 Victor A. Mckusick Leadership Award1
ASHG AWARDS AND ADDRESSES 2019 Victor A. McKusick Leadership Award1 Huda Y. Zoghbi2,3,4,5,6,7,* achieved. She withdrew from her parents and spent hours wringing her hands. Ashley was referred by her pediatrician, who suspected Rett syndrome based on a paper just pub- lished by Bengt Hagberg, describing the syndrome for the first time in English. I saw Ashley with Alan Percy and Vin- cent Riccardi, the attending neurologist and geneticist. I was intrigued by Ashley’s diagnosis, but a serendipitous meeting a week later with a girl diagnosed with cerebral palsy sealed my relationship with Rett syndrome. As she walked into the exam room, wringing her hands, I immediately realized it wasn’t cerebral palsy, but Rett syndrome. Combing through the clinic’s medical records, I ended up identifying and examining six girls with Rett syndrome within a few weeks. Rett was unlike any other disease I had seen, being neither congenital nor neurodegenerative. Thank you, David, for the kind introduction. I am honored After seeing these girls, I was convinced the cause was ge- to receive an award bearing the name of Victor McKusick, netic and felt compelled to figure it out. I approached Art one of my heroes in genetics, and to join the ranks of the Beaudet about doing a research fellowship in his lab to distinguished previous awardees who have inspired me in learn molecular genetics. Art took me on despite my hav- my career. I thank the board and the selection committee. ing no research background whatsoever. I shared my desire Most importantly, I thank my patients and their families to work on Rett, but Art urged me to find a Mendelian dis- for their trust and support. -

For Immediate Release
Contact: Seema Kumar Johnson & Johnson Pharmaceutical Research & Development, L.L.C. 908-218-6460 or [email protected] Frederik Wittock Johnson & Johnson Pharmaceutical Research & Development Division of Janssen Pharmaceutica, N.V +32 14 60 57 24 or [email protected] Drs. Erik De Clercq and Anthony S. Fauci Win 2010 Dr. Paul Janssen Award for Biomedical Research Recognized for Pioneering Work in Understanding and Combating HIV/AIDS Washington, DC – September 8, 2010 – Johnson & Johnson today announced that Erik De Clercq, M.D., Professor Emeritus, Rega Institute for Medical Research, Leuven, Belgium, and Anthony S. Fauci, M.D., Director of the National Institute of Allergy and Infectious Diseases, the National Institutes of Health, Bethesda, MD, have been named the recipients of the 2010 Dr. Paul Janssen Award for Biomedical Research by an independent selection committee comprised of world-renowned scientists. The Dr. Paul Janssen Award salutes the most passionate and creative scientists in basic or clinical research whose scientific achievements have made a measurable impact on human health. Drs. De Clercq and Fauci were selected for their pioneering work in understanding and combating viral diseases, particularly HIV/AIDS. The Award, which includes a $100,000 shared prize, will be presented to the winners during a ceremony in Washington, D.C., today. The award presentation and winners’ speeches may be viewed live beginning at 9:00 a.m. via www.pauljanssenaward.com. While accepting the honor, Dr. Fauci has declined his portion of the prize in order to comply with government ethics rules. Johnson & Johnson will donate his portion of the prize money to two organizations: Partners In Health—an international non-governmental organization dedicated to delivering quality health care to people and communities devastated by the joint burdens of poverty and disease, and Us Helping Us, People Into Living, Inc. -

Prize Winner Announcement
Contact: Seema Kumar Janssen Pharmaceutical Companies of Johnson & Johnson 908-218-6460 or [email protected] Diane Pressman Janssen Pharmaceutical Companies of Johnson & Johnson 908-927-6171 or [email protected] Frederik Wittock Janssen Pharmaceutical Companies of Johnson & Johnson +32 14 60 57 24 or [email protected] Dr. Napoleone Ferrara Wins 2011 Dr. Paul Janssen Award for Biomedical Research Discovery Unlocked Key to Novel Anti-angiogenesis Therapies Washington, DC – June 28, 2011 – Johnson & Johnson today announced the winner of the 2011 Dr. Paul Janssen Award for Biomedical Research during the BIO International Convention (BIO) in Washington D.C. Napoleone Ferrara, M.D., is the seventh leading scientist to win the Award, which honors a scientist or team of scientists whose contributions have the potential to significantly improve the health and lives of people around the world. Dr. Ferrara was selected by an independent committee of eight renowned scientists, including Nobel Laureates, Lasker Prize winners, and others, for his research on angiogenesis, the process of new blood vessel formation that plays a key role in cancer proliferation and a number of other diseases. Dr. Ferrara’s discoveries opened the door to the development of a new class of therapeutics to combat a serious eye disorder and contributed to the development of new oncology therapeutics. “With the 2011 Dr. Paul Janssen Award for Biomedical Research, Johnson & Johnson recognizes Dr. Ferrara for the meaningful impact his discoveries have had on the lives of patients all over the world,” said Paul Stoffels, M.D., Worldwide Chairman, Pharmaceuticals, Johnson & Johnson. “Like Dr. -

For Huda Zoghbi, Collaboration Is the Key to Unlocking the Secrets of Neurobiology
For Huda Zoghbi, collaboration is the key to unlocking the secrets of neurobiology Kathryn Claiborn J Clin Invest. 2011;121(9):3364-3364. https://doi.org/10.1172/JCI60154. News In June, the Peter and Patricia Gruber Foundation awarded the 2011 Neuroscience Prize to Huda Zoghbi in recognition of her work uncovering the genetic and molecular causes of neurological disorders. Zoghbi, a professor at Baylor College of Medicine, is also the director of the new Jan and Dan Duncan Neurological Research Institute (NRI), which opened in late 2010. The JCI recently spoke to Zoghbi about her accomplishments. JCI: How did you get interested in pediatric neurology? Zoghbi: I came to Baylor College of Medicine to be a pediatric cardiologist, and I didn’t have neurology on my radar screen. But during my pediatric residency, I rotated in neurology with Dr. Marvin Fishman, and the whole experience of encountering a neurological problem and figuring it out based on a very good clinical history and exam fascinated me. It felt like detective work. Afterward, I still thought I was going to be a cardiologist, but a month away from it, I missed neurology very much, and I decided I had to come back and revisit it. For me, part of the appeal of neurology was that if you take the time to think through the problem, most of the time you can reach the right clinical and anatomical diagnosis. JCI: You’ve made a number of remarkable discoveries, including identifying the genes that underlie […] Find the latest version: https://jci.me/60154/pdf News For Huda Zoghbi, collaboration is the key to unlocking the secrets of neurobiology In June, the Peter and Patricia Gruber Foun- that the final behavioral phenotype might dation awarded the 2011 Neuroscience Prize result from failure of neuronal homeostasis to Huda Zoghbi in recognition of her work rather than a specific physiological change.