Cambodia—High Contamination at Collection and Consumption Level
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Collective Land Registration of Indigenous Communities in Ratanakiri Province
Briefing Note Senate Region 8 Collective Land Registration of Indigenous Communities in Ratanakiri province Researcher in charge: Mr. KHAM Vanda Assisted by: Mr. NUN Assachan Ms. CHEA Malika Ms. WIN Moh Moh Htay April, 2016 Parliamentary Institute of Cambodia Notice of Disclaimer The Parliamentary Institute of Cambodia (PIC) is an independent parliamentary support institution for the Cambodian Parliament which, upon request from parliamentarians and parliamentary commissions, offers a wide range of services. These include capacity development in the form of training, workshops, seminars and internships, as well as support for outreach activities. Parliamentary research has been a particular focus and PIC has placed an emphasis on developing the associated skills of parliamentary staff while producing the research reports needed to guide Parliamentarians in pursuing their legislation role. PIC research reports provide information about subjects that are relevant to parliamentary and constituency work including key emerging issues, legislation and major public policy topics. They do not, however, purport to represent or reflect the views of the Parliamentary Institute of Cambodia, the Parliament of Cambodia, or of any of its members. The contents of these reports, current at the date of publication, are for reference purposes only. They are not designed to provide legal or policy advice, and do not necessarily deal with every important topic or aspect of the issues they consider. The contents of this research report are covered by applicable Cambodian laws and international copyright agreements. Permission to reproduce in whole or in part or otherwise use the content of this research may be sought from the appropriate source. -

The Cambodia Climate Change Alliance (CCCA)
2014:48 Sida Decentralised Evaluation Mr. Alan Ferguson Dr. Sovith Sin The Cambodia Climate Change Alliance (CCCA) Final Report The Cambodia Climate Change Alliance (CCCA) Final Report June 2014 Mr. Alan Ferguson Dr. Sovith Sin Sida Decentralised Evaluation 2014:48 Sida Authors: Mr. Alan Ferguson and Dr. Sovith Sin The views and interpretations expressed in this report are the authors’ and do not necessarily reflect those of the Swedish International Development Cooperation Agency, Sida. Sida Decentralised Evaluation 2014:48 Commissioned by the UNDP, which Sweden funded 30%. Copyright: Sida and the authors Date of final report: June 2014 Published by Citat 2014 Art. no. Sida61807en urn:nbn:se:sida-61807en This publication can be downloaded from: http://www.sida.se/publications SWEDISH INTERNATIONAL DEVELOPMENT COOPERATION AGENCY Address: S-105 25 Stockholm, Sweden. Office: Valhallavägen 199, Stockholm Telephone: +46 (0)8-698 50 00. Telefax: +46 (0)8-20 88 64 E-mail: [email protected]. Homepage: http://www.sida.se TABLE OF CONTENTS Executive Summary .................................................................................................................... v 1. Introduction ...................................................................................................................... 1 1.1 Overall Objectives of CCCA ...................................................................... 1 1.2 Final Review Assignment........................................................................... 2 1.3 Context ......................................................................................................... -

Cambodian Journal of Natural History
Cambodian Journal of Natural History Rediscovery of the Bokor horned frog Four more Cambodian bats How to monitor a marine reserve The need for community conservation areas Eleven new Masters of Science December 2013 Vol 2013 No. 2 Cambodian Journal of Natural History ISSN 2226–969X Editors Email: [email protected] • Dr Jenny C. Daltry, Senior Conservation Biologist, Fauna & Flora International. • Dr Neil M. Furey, Research Associate, Fauna & Flora International: Cambodia Programme. • Hang Chanthon, Former Vice-Rector, Royal University of Phnom Penh. • Dr Nicholas J. Souter, Project Manager, University Capacity Building Project, Fauna & Flora International: Cambodia Programme. International Editorial Board • Dr Stephen J. Browne, Fauna & Flora International, • Dr Sovanmoly Hul, Muséum National d’Histoire Singapore. Naturelle, Paris, France. • Dr Martin Fisher, Editor of Oryx—The International • Dr Andy L. Maxwell, World Wide Fund for Nature, Journal of Conservation, Cambridge, United Kingdom. Cambodia. • Dr L. Lee Grismer, La Sierra University, California, • Dr Jörg Menzel, University of Bonn, Germany. USA. • Dr Brad Pett itt , Murdoch University, Australia. • Dr Knud E. Heller, Nykøbing Falster Zoo, Denmark. • Dr Campbell O. Webb, Harvard University Herbaria, USA. Other peer reviewers for this volume • Dr Judith Eger, Royal Ontario Museum, Toronto, • Berry Mulligan, Fauna & Flora International, Phnom Canada. Penh, Cambodia. • Pisuth Ek-Amnuay, Siam Insect Zoo & Museum, • Prof. Dr. Annemarie Ohler, Muséum national Chiang Mai, Thailand. d’Histoire naturelle, Paris, France. • Dr James Guest, University of New South Wales, • Dr Jodi Rowley, Australian Museum, Sydney, Sydney, Australia. Australia. • Dr Kristofer M. Helgen, Smithsonian Institute, • Dr Manuel Ruedi, Natural History Museum of Washington DC, USA. Geneva, Geneva, Switz erland. -

Ratanakiri, Cambodia*
Southeast Asian Studies, Vol. 47, No. 3, December 2009 Understanding Changes in Land and Forest Resource Management Systems: Ratanakiri, Cambodia* Jefferson FOX,** John B. VOGLER*** and Mark POFFENBERGER**** Abstract This paper draws on case studies from three communities in Ratanakiri to illustrate both the forces driving land-use and tenure change as well as how effective community stewardship can guide agricultural transi- tions. The study combines a time series of remotely sensed data from 1989 to 2006 to evaluate changes in land use, and relates this data to in-depth ground truth observations and social research from three villages. The methodology was designed to evaluate how indigenous communities who had historically managed forest lands as communal resources, are responding to market forces and pressures from land speculators. Krala Village received support from local non-government organizations (NGOs) to strengthen community, map its land, demarcate boundaries, strengthen resource use regulations, and develop land-use plans. The two other villages, Leu Khun and Tuy, each received successively less support from outside organizations for purposes of resource mapping and virtually no support for institutional strengthening. The remote sensing data indicates that in Krala, over the 16 year study period, protected forest areas remained virtually intact, while total forest cover declined at an annual rate of only 0.86% whereas in Leu Khun and Tuy the annual rates were 1.63 and 4.88% respectively. Keywords: land use, land cover, forest management, resource management systems, Cambodia I Introduction Over the past decade, Ratanakiri Province has experienced unprecedented changes in land use and tenure. This study analyzes remotely sensed images taken in 1989 and December 2006 to assess changes in vegetative cover in three areas near Banlung the provincial capital, and draws on in-depth case studies from three communities in the research area. -

Impacts of Economic Land Concessions on Project Target
Impacts of Economic Land Concessions on Project Target Communities Living Near Concession Areas in Virachey National Park and Lumphat Wildlife Sanctuary, Ratanakiri Province Impacts of Economic Land Concessions on Project Target Communities Living Near Concession Areas in Virachey National Park and Lumphat Wildlife Sanctuary, Ratanakiri Province Submitted by: Ngin Chanrith, Neth Baromey, and Heng Naret To: Save Cambodia’s Wildlife November 2016 Contact: Save Cambodia's Wildlife (SCW), E-Mail: [email protected] , Phone: +855 (0)23 882 035 #6Eo, St. 570, Sangkat Boeung Kak 2, Khan Tuol Kork, Phnom Penh, Cambodia www.facebook.com/SaveCambodiasWildlife, www.cambodiaswildlife.org Impacts of Economic Land Concessions on Project Target Communities Living Near Concession Areas in Virachey National Park and Lumphat Wildlife Sanctuary, Ratanakiri Province CONTENTS ACRONYMS i EXECUTIVE SUMMARY ii CHAPTER: Page 1. INTRODUCTION 1.1. Backgrounds and Rationale …………………………………………………..………...1 1.2. Aim and Objectives …………………………………………………………..………...2 2. METHODOLOGY 2.1. Data Collection Methods…………………………………………………..…………..3 2.2. Sampling Techniques and Sampling Frames……………………………………..…….. 4 2.3. Data Analysis Methods………………………………………………………..………..5 2.4. Limitations of the Study…………………………………………………………..….....5 3. STATUS OF INDIGENOUS COMMUNITY LIVELIHOODS IN RATANAKIRI 3.1. Profile and Characteristics of Ratanakiri Province……………………………..……....6 3.2. Livelihood Vulnerability of Indigenous Communities…………………………..……....8 3.3. Capital Assets of Indigenous Community Livelihoods………………………..………17 4. ELCs AND IMPACTS ON INDIGENOUS COMMUNITY LIVELIHOODS 4.1. Status of Economic Land Concessions in Ratanakiri Province………………..……....27 4.2. Impacts of ELCs on Indigenous Communities and Their Areas…………………..…. 29 4.3. ELC-Community Conflicts and Existing Conflict Resolution Actors …………..…… 36 5. LIVELIHOOD INTERVENTION PROGRAMS OF CONCERNED STAKEHOLDERS 5.1. Community Perceptions of Current Livelihood Interventions Mechanisms….……. -
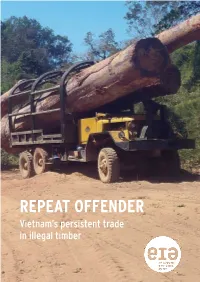
Repeat Offender: Vietnam's Persistent Trade in Illegal Timber
REPEAT OFFENDER Vietnam’s persistent trade in illegal timber ACKNOWLEDGEMENTS This report was written and edited by the Environmental Investigation Agency UK Ltd. This document has been produced with CONTENTS the financial assistance of UKaid and the Norwegian Agency for Development Cooperation (NORAD). The contents of this publication are the sole responsibility 2 INTRODUCTION of EIA. EIA expresses its gratitude to the individuals 3 VIETNAM’S TRADE IN STOLEN TIMBER who contributed to the production of this report and who for safety reasons must remain anonymous. 7 STATE-SANCTIONED TIMBER THEFT 16 REGULATING FOREST CRIME May 2017 © Environmental Investigation Agency 2017 18 CONCLUSIONS AND RECOMMENDATIONS All images © EIA unless otherwise stated Design: www.designsolutions.me.uk LAOS Dong Ha La Ley THAILAND Attapeu town Bo Y O’Tabok Pleiku Qui Nhon O’Tang Le Thanh CAMBODIA Phnom Penh VIETNAM Ho Chi Minh City ENVIRONMENTAL INVESTIGATION AGENCY (EIA) 62/63 Upper Street, London N1 0NY, UK Tel: +44 (0) 20 7354 7960 email: [email protected] www.eia-international.org EIA US P.O.Box 53343 Washington DC 20009 USA Tel: +1 202 483 6621 email: [email protected] COVER: Logs illegally cut in O’Tabok Community Protected Area, within Virachey National Park in Cambodia’s Ratanakiri province, await transportation to Vietnam, February 2017. INTRODUCTION This month, Vietnam and the European Union (EU) will initial an agreement to ensure only legally harvested and traded timber flows through Vietnam to the EU and beyond. But as both parties meet to secure corrupt Cambodian officials and With about 300,000m3 of logs having commitments, Government officials and security force personnel in the pay been smuggled out of Cambodia and security force personnel in Vietnam will of Vietnamese timber traders. -

Pdf IWGIA Book Land Alienation 2006 EN
Land Alienation in Indigenous Minority Communities - Ratanakiri Province, Cambodia Readers of this report are also directed toward the enclosed video documentary made on this topic in October 2005: “CRISIS – Indigenous Land Crisis in Ratanakiri”. Also relevant is the Report “Workshop to Seek Strategies to Prevent Indigenous Land Alienation” published by NGO Forum in collaboration with CARE Cambodia, 28-20 March 2005. - Final Draft- August 2006 Land Alienation in Indigenous Minority Communities - Ratanakiri Province, Cambodia Table of Contents Contents............................................................................................................................. 3 Executive Summary ............................................................................................................. 4 Recommendations .............................................................................................................. 5 Executive Summary – November 2004................................................................................. 6 Introduction ....................................................................................................................... 8 Methodology...................................................................................................................... 10 The Legal Situation.............................................................................................................. 11 The Situation in January 2006 ............................................................................................ -

Contested Land Restitution Processes in Cambodia
land Review Contested Land Restitution Processes in Cambodia Chanrith Ngin and Andreas Neef * Development Studies, School of Social Sciences, Faculty of Arts, The University of Auckland, 1142 Auckland, New Zealand; [email protected] * Correspondence: [email protected] Abstract: Cambodia has experienced rapid economic growth due partly to excessive natural resource extraction. Land conflicts have been pervasive between local communities and companies that invest in land and other natural resources. Despite substantial research into land conflict resolution, knowledge about how land is returned to wronged parties and what happens to the returned land is fragmented. This review aims to provide a holistic understanding of land restitution in Cambodia by examining different types of land conflict, actors involved, and restitution processes. It provides both a macro perspective on land restitution and conflict-specific perspectives regarding how actors engage in different processes that produce various outcomes for disputants. We find both complications and ambivalence of the actors involved, particularly concerning their roles and influences in resolution processes. Specifically, we find contentious and ambivalent roles that non- governmental organisations (NGOs), donor agencies, and government authorities played in mixed results of resolution mechanisms in the cases that have yielded outcomes in terms of land restitution. Our review also suggests that the neoliberal policy that favours commoditisation of resources and the authoritarian patronage state disguised in a hybrid democracy allowed some grassroots resistance, civil society space, and responses from other concerned economic and political actors in the resolution processes. However, the state controlled and manipulated their engagement to benefit and maintain its economic and political bases, and it never allowed any transformative approach that could tackle the root causes of the problems. -

Cambodia Municipality and Province Investment Information
Cambodia Municipality and Province Investment Information 2013 Council for the Development of Cambodia MAP OF CAMBODIA Note: While every reasonable effort has been made to ensure that the information in this publication is accurate, Japan International Cooperation Agency does not accept any legal responsibility for the fortuitous loss or damages or consequences caused by any error in description of this publication, or accompanying with the distribution, contents or use of this publication. All rights are reserved to Japan International Cooperation Agency. The material in this publication is copyrighted. CONTENTS MAP OF CAMBODIA CONTENTS 1. Banteay Meanchey Province ......................................................................................................... 1 2. Battambang Province .................................................................................................................... 7 3. Kampong Cham Province ........................................................................................................... 13 4. Kampong Chhnang Province ..................................................................................................... 19 5. Kampong Speu Province ............................................................................................................. 25 6. Kampong Thom Province ........................................................................................................... 31 7. Kampot Province ........................................................................................................................ -

Land Acquisitions in Northeastern Cambodia: Space and Time Matters
Land grabbing, conflict and agrarian‐environmental transformations: perspectives from East and Southeast Asia An international academic conference 5‐6 June 2015, Chiang Mai University Conference Paper No. 24 Land Acquisitions in Northeastern Cambodia: Space and Time matters Christophe Gironde and Amaury Peeters May 2015 BICAS www.plaas.org.za/bicas www.iss.nl/bicas In collaboration with: Demeter (Droits et Egalite pour une Meilleure Economie de la Terre), Geneva Graduate Institute University of Amsterdam WOTRO/AISSR Project on Land Investments (Indonesia/Philippines) Université de Montréal – REINVENTERRA (Asia) Project Mekong Research Group, University of Sydney (AMRC) University of Wisconsin-Madison With funding support from: Land Acquisitions in Northeastern Cambodia: Space and Time matters by Christophe Gironde and Amaury Peeters Published by: BRICS Initiatives for Critical Agrarian Studies (BICAS) Email: [email protected] Websites: www.plaas.org.za/bicas | www.iss.nl/bicas MOSAIC Research Project Website: www.iss.nl/mosaic Land Deal Politics Initiative (LDPI) Email: [email protected] Website: www.iss.nl/ldpi RCSD Chiang Mai University Faculty of Social Sciences, Chiang Mai University Chiang Mai 50200 THAILAND Tel. 6653943595/6 | Fax. 6653893279 Email : [email protected] | Website : http://rcsd.soc.cmu.ac.th Transnational Institute PO Box 14656, 1001 LD Amsterdam, The Netherlands Tel: +31 20 662 66 08 | Fax: +31 20 675 71 76 Email: [email protected] | Website: www.tni.org May 2015 Published with financial support from Ford Foundation, Transnational Institute, NWO and DFID. Abstract Over the last decade, the highlands of Ratanakiri province in northeastern Cambodia have witnessed massive land acquisitions and profound land use changes, mostly from forest covers to rubber plantation, which has contributed to rapidly and profoundly transform the livelihoods of smallholders relying primarily on family-based farming. -
National Assessment Report on Mercury in Cambodia
National Assessment Report on Mercury in Cambodia Prepared by: Department of Hazardous Substance Management, General Directorate of Environmental Protection, Ministry of Environment Supported by: United Nations for Environment Programme, Division of Technology, Industry and Economics, The International Environmental Technology Centre (IETC) August 2016 Acknowledgement The completion of this report could not have been possible without participation and assistance of many people whose names may not all be listed. Their contributions are sincerely appreciated and grateful acknowledged. However, The Department of Hazardous Substance Management, would like to express its deep appreciation and indebtedness particularly to following: His Excellency Say Samal, Minister of Environment, His Excellency Heng Nareth, Director General for Environmental Protection for their kind support in the preparation of this report and the implementation of Mercury Initial Assessment project United Nations for Environment Programme, Division of Technology, Industry and Economics, The International Environmental Technology Centre (IETC) for providing financial and technical support for implementation of Mercury Initial Assessment project which this report is part of. Executive Summary In October 2013, Cambodia endorsed the notification of signatory of Minamata Implementation Plan for the UNEP Global Mercury, currently under implementation process. This plan is an indication of a new effort by Cambodia to provide additional guidance in the form of specific goals, objectives and actions for the sound management of mercury. In the Kingdom of Cambodia, the use of hazardous substances, especially the mercury substances are not normally managed in an environmentally sound manner and there is no specific government institution responsible for mercury management. Therefore, management of mercury and mercury-containing wastes in Cambodia is a collaboration of various ministries within a government. -

2 Indigenous Peoples in Cambodia
UNITED NATIONS COMMITTEE ON THE ELIMINATION OF RACIAL DISCRIMINATION (76TH SESSION 2010) Submitted by Indigenous People NGO Network (IPNN) Coordinated by NGO Forum on Cambodia In cooperation with Asian Indigenous Peoples Pact (AIPP) February 2010 UNITED NATIONS COMMITTEE ON THE ELIMINATION OF RACIAL DISCRIMINATION (76TH SESSION 2010) THE RIGHTS OF INDIGENOUS PEOPLES IN CAMBODIA Submitted by Indigenous People NGO Network (IPNN) Coordinated by NGO Forum on Cambodia In cooperation with Asian Indigenous Peoples Pact (AIPP) Table of Contents 1 INTRODUCTION ...................................................................................................................................2 2 INDIGENOUS PEOPLES IN CAMBODIA ..........................................................................................2 3 OVERALL LEGAL FRAMEWORK ......................................................................................................3 4 EDUCATION ...........................................................................................................................................4 5 NATURAL RESOURCE MANAGEMENT...........................................................................................4 5.1 Forest Issues ...........................................................................................................................................5ry 5.2 Protected Areas..........................................................................................................................................6 5.3 LAND...............................................................................................................................................................7