Metacarpal and Metatarsal Fractures in Dogs
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Skeletal Foot Structure
Foot Skeletal Structure The disarticulated bones of the left foot, from above (The talus and calcaneus remain articulated) 1 Calcaneus 2 Talus 3 Navicular 4 Medial cuneiform 5 Intermediate cuneiform 6 Lateral cuneiform 7 Cuboid 8 First metatarsal 9 Second metatarsal 10 Third metatarsal 11 Fourth metatarsal 12 Fifth metatarsal 13 Proximal phalanx of great toe 14 Distal phalanx of great toe 15 Proximal phalanx of second toe 16 Middle phalanx of second toe 17 Distal phalanx of second toe Bones of the tarsus, the back part of the foot Talus Calcaneus Navicular bone Cuboid bone Medial, intermediate and lateral cuneiform bones Bones of the metatarsus, the forepart of the foot First to fifth metatarsal bones (numbered from the medial side) Bones of the toes or digits Phalanges -- a proximal and a distal phalanx for the great toe; proximal, middle and distal phalanges for the second to fifth toes Sesamoid bones Two always present in the tendons of flexor hallucis brevis Origin and meaning of some terms associated with the foot Tibia: Latin for a flute or pipe; the shin bone has a fanciful resemblance to this wind instrument. Fibula: Latin for a pin or skewer; the long thin bone of the leg. Adjective fibular or peroneal, which is from the Greek for pin. Tarsus: Greek for a wicker frame; the basic framework for the back of the foot. Metatarsus: Greek for beyond the tarsus; the forepart of the foot. Talus (astragalus): Latin (Greek) for one of a set of dice; viewed from above the main part of the talus has a rather square appearance. -

Canine Tarsus Stabilization Surgical Technique 1 2
Canine Tarsus Stabilization Surgical Technique 1 2 Place the patient in a dorsal recumbent position and Make a medial incision beginning just proximal to the administer general anesthesia. Perform a hanging limb medial malleolus extending distally to the level of the technique with aseptic preparation and appropriate proximal intertarsal joint. Inspect the medial structures limb draping. of the tarsal joint. Identify the origin of the long part of the medial collateral ligament (MCL) on the medial malleolus of the tibia. 3 4 Using the aiming guide, place the 0.049 inch (1.2 mm) Use the 2.0 mm cannulated drill over the guidewire to guidewire from the origin of the long part of the MCL create the tibial bone tunnel for suture passage. in a proximal and slight cranial direction such that the it emerges on the lateral tibia just cranial to the fibula. Make a small incision on the lateral side where the guidewire tents the skin. 5 As a surgical landmark, identify the talocentral tarsal joint on the medial side by either a palpation or by inserting a small needle into the joint space. Using the aiming guide, place a 0.049 inch (1.2 mm) guidewire starting at the medial aspect of the talar head oriented parallel to the talocentral tarsal joint in a slightly plantar direction to capture the calcaneus. The guidewire should emerge just plantar to the boney tubercle of the lateral portion of the distal calcaneus. Make a small incision where the guidewire tents the skin. 6 7 Use the 2.0 mm cannulated drill over the guidewire to Identify the insertion of the short part of the MCL on the create the distal talus bone tunnel for suture passage. -

Equine MRI, Edited by Rachel C
Chapter 17 The p roximal t arsal r egion Rachel Murray , Natasha Werpy , Fabrice Audigi é , Jean - Marie Denoix , Matthew Brokken and Thorben Schulze INTRODUCTION Imaging of the proximal tarsus can be achieved in both standing and anaes- thetized horses. The height of the horse and the amount of hind end mus- culature determines which magnet confi guration will produce the best images of this region. A horse with short limbs and wide, well - muscled quarters may be more diffi cult to fi t into the long, narrow bore of some high - fi eld magnets under general anaesthesia. In the same way, the side of the lateral recumbency should be considered because it is generally easier to bring the proximal tarsus of the lower hind limb closer to the isocentre of the magnet compared with the upper one. Well developed hind limb musculature can prevent the limb from being placed far enough into the bore to allow the tarsus to be positioned at the isocentre of the magnet. The tarsus of a horse with this body type (or stature) is more easily positioned in a standing system. In contrast, for a narrow horse with long limbs, the height of the tarsus and width between the limbs may make it more diffi cult to image this region within a standing system. The degree of sway in the proximal aspect of the limbs in a standing, sedated horse is often substan- tially greater than in the distal aspect of the limbs. This degree of sway can produce signifi cant motion artefact and can make it frustrating to acquire images of the proximal tarsus. -

Four Unusual Cases of Congenital Forelimb Malformations in Dogs
animals Article Four Unusual Cases of Congenital Forelimb Malformations in Dogs Simona Di Pietro 1 , Giuseppe Santi Rapisarda 2, Luca Cicero 3,* , Vito Angileri 4, Simona Morabito 5, Giovanni Cassata 3 and Francesco Macrì 1 1 Department of Veterinary Sciences, University of Messina, Viale Palatucci, 98168 Messina, Italy; [email protected] (S.D.P.); [email protected] (F.M.) 2 Department of Veterinary Prevention, Provincial Health Authority of Catania, 95030 Gravina di Catania, Italy; [email protected] 3 Institute Zooprofilattico Sperimentale of Sicily, Via G. Marinuzzi, 3, 90129 Palermo, Italy; [email protected] 4 Veterinary Practitioner, 91025 Marsala, Italy; [email protected] 5 Ospedale Veterinario I Portoni Rossi, Via Roma, 57/a, 40069 Zola Predosa (BO), Italy; [email protected] * Correspondence: [email protected] Simple Summary: Congenital limb defects are sporadically encountered in dogs during normal clinical practice. Literature concerning their diagnosis and management in canine species is poor. Sometimes, the diagnosis and description of congenital limb abnormalities are complicated by the concurrent presence of different malformations in the same limb and the lack of widely accepted classification schemes. In order to improve the knowledge about congenital limb anomalies in dogs, this report describes the clinical and radiographic findings in four dogs affected by unusual congenital forelimb defects, underlying also the importance of reviewing current terminology. Citation: Di Pietro, S.; Rapisarda, G.S.; Cicero, L.; Angileri, V.; Morabito, Abstract: Four dogs were presented with thoracic limb deformity. After clinical and radiographic S.; Cassata, G.; Macrì, F. Four Unusual examinations, a diagnosis of congenital malformations was performed for each of them. -

The Ossification of the Metacarpal and Phalangeal Bones in Human Foetuses
Folia Morphol. Vol. 63, No. 3, pp. 329–332 Copyright © 2004 Via Medica O R I G I N A L A R T I C L E ISSN 0015–5659 www.fm.viamedica.pl The ossification of the metacarpal and phalangeal bones in human foetuses Florian Czerwiński1, Ewa Tomasik1, Małgorzata Tomasik2, Aldona Mahaczek-Kordowska1 1Department of Anatomy, Pomeranian Academy of Medicine, Szczecin, Poland 2Department of General Dentistry, Pomeranian Academy of Medicine, Szczecin, Poland [Received 4 November 2002; Revised 17 February 2004; Accepted 17 February 2004] An evaluation was made of the ossification level of the metacarpal and pha- langeal bones in human foetuses of both sexes from the 4th to the 9th month of gestation. Our results indicate that ossification of phalangeal bones 1 to 5 al- ways started at the distal end of the phalanx and endochondral ossification prevailed in the proximal phalanx of the thumb. Key words: human foetus, metacarpal bones, phalangeal bones, ossification INTRODUCTION Most human skeletal bones are ossified on a car- tilaginous base [5, 14]. This is a complex process pro- gressing dynamically in time and ossification consti- tutes the final phase of this complex process [3]. Thorough observation of the ossification of the foe- tal skeleton is made possible by means of the radio- logical method and evaluation of histological speci- mens [9]. This study presents the ossification of the metacarpal and phalangeal bones in human foetus- es at different stages of gestation. MATERIAL AND METHOD Eighty-six hands were examined taken from hu- man foetuses of both sexes aged from 4 to 9 months of gestation. -
The Occurrence of Tarsal Injuries in Male Mice of C57BL/6N Substrains in Multiple
bioRxiv preprint doi: https://doi.org/10.1101/2020.02.25.964254; this version posted February 25, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. 1 Long title: The occurrence of tarsal injuries in male mice of C57BL/6N substrains in multiple 2 international mouse facilities 3 4 Short title: Tarsal injury in C57BL/6N male mice 5 6 Eleanor Herbert2, Michelle Stewart1, Marie Hutchison1, Ann M. Flenniken4,5, Dawei Qu4,5, 7 Lauryl M. J. Nutter4,6, Colin McKerlie4,6, Liane Hobson1, Brenda Kick3, Bonnie Lyons3, Jean- 8 Paul Wiegand3, Rosalinda Doty3, Juan Antonio Aguilar-Pimentel7, Martin Hrabe de Angelis7,8,9, 9 Mary Dickinson10, John Seavitt10, Jacqueline K. White3, Cheryl L Scudamore1, Sara Wells1* 10 11 12 13 Affiliations 14 1 Mary Lyon Centre, MRC Harwell Institute, Harwell Campus, Oxfordshire, OX11 0RD, UK 15 2 Department of Pathobiology and Population Sciences, Royal Veterinary College, Hertfordshire, 16 UK AL9 7TA, UK 17 3 The Jackson Laboratory, 600 Main Street, Bar Harbor, Maine 04609, USA 18 4 The Centre for Phenogenomics, Toronto, ON, Canada, M5T 3H7 19 5 Lunenfeld-Tanenbaum Research Institute, Sinai Health, 600 University Avenue, Toronto, 20 ON, Canada, M5G 1X5 21 6 The Hospital for Sick Children, 555 University Avenue, Toronto, ON, Canada, M5G 1X8 22 7German Mouse Clinic, Institute of Experimental Genetics, Helmholtz Zentrum München, 23 Ingolstädter Landstraße 1, 85764 Neuherberg, Germany 24 8School of Life Science Weihenstephan, Technische Universität München, Alte Akademie 8, 25 85354 Freising, Germany 26 9German Center for Diabetes Research (DZD), Ingolstädter Landstr. -

Metacarpal Fractures: Practical Methods for Measurement of Shortening, Angulation, and Malrotation
J Orthop Spine Trauma. 2020 March; 6(1): 9-13. DOI: http://dx.doi.org/10.18502/jost.v6i1.4535 Educational Corner Metacarpal Fractures: Practical Methods for Measurement of Shortening, Angulation, and Malrotation Rohollah Khajeh 1, Behzad Enayati1, Farzad Vosughi2, Seyed Mohammad Javad Mortazavi 3,* 1 Fellowship of Hand Surgery, Joint Reconstruction Research Center, Tehran University of Medical Sciences, Tehran, Iran 2 Resident, Department of Orthopedics, Joint Reconstruction Research Center, Tehran University of Medical Sciences, Tehran, Iran 3 Professor, Department of Orthopedic Surgery, Joint Reconstruction Research Center, Tehran University of Medical Sciences, Tehran, Iran *Corresponding author: Seyed Mohammad Javad Mortazavi; Department of Orthopedic Surgery, Joint Reconstruction Research Center, Tehran University of Medical Sciences, Tehran, Iran. Tel: +98-2161192767, Email: [email protected] Received: 09 October 2019; Revised: 15 December 2019; Accepted: 17 January 2020 Keywords: Metacarpus; Fractures, Bone; Hand Deformities, Acquired Citation: Khajeh R, Enayati B, Vosughi F, Mortazavi SMJ. Metacarpal Fractures: Practical Methods for Measurement of Shortening, Angulation, and Malrotation. J Orthop Spine Trauma 2020; 6(1): 9-13. Background different metacarpal fractures. Articular fractures involving less than 20% of the joint Phalangeal, distal radius, and metacarpal fractures are surface and nondisplaced or minimally displaced shaft the most frequent upper limb fractures, respectively (1). fractures, without significant angulation, malrotation, or The incidence of metacarpal fractures in the United States shortening are treated with immobilization in the of America (USA) is 13.6 among every 100000 population intrinsic plus position (6). Bony apposition of at least 50% annually (2). Metacarpal fractures compose 30-40 percent and maximal bone shortening of 5 mm is acceptable. -

Radiography and Radiographic Interpretation of the Tarsus (VET-473) Western Veterinary Conference 2004 Timothy R
Radiography and Radiographic Interpretation of the Tarsus (VET-473) Western Veterinary Conference 2004 Timothy R. O'Brien, DVM, PhD, DACVR University of California, Davis Davis, CA, USA 18276161 I. Introduction Tarsal diseases are a common cause of hind limb lameness in the horse. The clinical signs of tarsal disease often resemble those of stifle disease particularly the response to flexion tests. As a result both the stifle and tarsus are commonly radiographed to identify pathologic change in the horse with a hind limb lameness and during purchase evaluations. It seems prudent for purchase evaluations to radiograph these anatomical areas in both limbs. Radiographic interpretation of the tarsus is considered difficult by most equine practitioners. There seems to be three major causes of this difficulty. These causes relate to the numerous bones comprising the tarsus, variety of shapes of the tarsal bones, and veterinarians tend to be less familiar with the radiographic anatomy and pathology of the tarsus than most other anatomical regions, particularly regions of the forelimb. I am going to make some general statements in an attempt to simplify the radiographic interpretation of the tarsus. These general statements are: Most radiographic findings are located at the dorsum of the tarsus. Pathologic abnormalities of the tarsus tend to be in specific anatomical areas. Soft tissue swelling (STS) is a key for assisting to localize the abnormality. There are only a few radiographic diagnoses for the tarsus. The diagnoses of abnormalities of the tarsus identified with radiology can be classified in the following way: 1. Soft tissue swelling without bony change 2. -

Bones of the Hindlimb
BONES OF THE HINDLIMB Andrea Heinzlmann University of Veterinary Medicine Budapest Department of Anatomy and Histology 1st Oktober 2019 BONES OF THE HINDLIMB COMPOSED OF: 1. PELVIC GIRDLE (CINGULUM MEMBRI PELVINI) 2. THIGH 3. LEG (CRUS) 4. FOOT (PES) BONES OF THE PELVIC LIMB (OSSA MEMBRI PELVINI) PELVIC GIRDLE (CINGULUM MEMBRI PELVINI): - connection between the pelvic limb and the trunk consists of: 1. two HIP BONES (OSSA COXARUM) Hip bones of a pig, dorsal aspect Hip bones of a pig, ventral aspect PELVIC GIRDLE (CINGULUM MEMBRI PELVINI) HIP BONE (OS COXAE): - in young animals each hip bone comprises three bones: 1. ILIUM (OS ILII) – craniodorsal 2. PUBIS (OS PUBIS) – cranioventral 3. ISHIUM (OS ISCHI) – caudoventral - all three bones united by a synchondrosis - the synchondrosis ossifies later in life Hip bones of an ox, left lateral aspect Hip bones of an ox, ventrocranial aspect PELVIC GIRDLE (CINGULUM MEMBRI PELVINI) HIP BONE (OS COXAE): ACETABULUM: - ilium, pubis and ischium meet at the acetabulum Left acetabulum of a horse, lateral aspect Hip bones of a dog, right lateral aspect Left acetabulum of an ox, lateral aspect PELVIC GIRDLE (CINGULUM MEMBRI PELVINI) HIP BONE (OS COXAE): SYMPHYSIS PELVINA: - the two hip bones united ventrally at the symphysis pelvina by a fibrocartilaginous joint ossified with advancing age - in females the fibrocartilage of the symphysis becomes loosened during pregnancy by action of hormones Hip bones of a horse, ventrocranial aspect Hip bones of an ox, ventrocranial aspect PELVIC GIRDLE (CINGULUM MEMBRI PELVINI) HIP BONE (OS COXAE): SYMPHYSIS PELVINA: - in females the fibrocartilage of the symphysis becomes loosened during pregnancy by action of hormones http://pchorse.se/index.php/en/articles/topic-of-the-month/topics-topics/4395-mars2017-eng PELVIC GIRDLE (CINGULUM MEMBRI PELVINI) HIP BONE (OS COXAE): SYMPHYSIS PELVINA divided into: 1. -

How to Interpret Radiographs of the Carpus and Tarsus of the Young Performance Horse
HOW TO TAKE AND INTERPRET RADIOGRAPHS OF THE YOUNG PERFORMANCE HORSE How to Interpret Radiographs of the Carpus and Tarsus of the Young Performance Horse Elizabeth M. Santschi, DVM, Diplomate ACVS Author’s address: Department of Veterinary Clinical Sciences, The Ohio State University, 601 Vernon L. Tharp Street, Columbus, OH 43210; [email protected]. © 2013 AAEP. 1. Introduction there are areas that are more commonly affected by Routine radiographic evaluation of young perfor- RA, and they should receive the closest scrutiny. mance horses has become commonplace in Thor- These will be denoted by black circles on the radio- oughbreds but also occurs in other performance graphic images included in these proceedings. RA breeds. This practice has resulted in the frequent best detected on a specific projection will be listed in discovery of radiographic abnormalities (RA) that bold, but should be confirmed on other projections are often clinically silent but can cause concern in when possible. Finally, readers should always con- buyers and sellers of young performance stock. sider three general factors when reviewing radio- The prevalence of radiographic developmental or- graphic images: thopedic disease in 6-month-old horses has been re- (1) Make sure that the films are of the correct ported to be 25% in Warmbloods, 41% in horse. Standardbreds, and 34% in Thoroughbreds.1 In (2) Make sure the date is appropriate and Thoroughbred yearlings intended for racing, 86.3% consistent. exhibit RA2; in young Standardbreds, 42%3; in year- (3) Make sure all required views are present and ling Warmblood horses, 69.5%4; and in 1- and of acceptable quality. -

Macroanatomy of the Bones of Thoracic Limb of an Asian Elephant (Elephas Maximus)
Int. J. Morphol., 34(3):909-917, 2016. Macroanatomy of the Bones of Thoracic Limb of an Asian Elephant (Elephas maximus) Macroanatomía de los Huesos del Miembro Torácico de un Elefante Asiático (Elephas maximus) A. S. M. Lutful Ahasan*; Md. Abul Quasem*; Mohammad Lutfur Rahman*; Rubyath Binte Hasan*; A. S. M. Golam Kibria* & Subrata Kumar Shil* AHASAN, A. M. S. L.; QUASEM, M. A.; RAHMAN, M. L.; HASAN, R. B.; KIBRIA, A. S. M. G. & SHIL, S. K. Macroanatomy of the bones of thoracic limb of an Asian Elephant (Elephas maximus). Int. J. Morphol., 34(3):909-917, 2016. SUMMARY: Bones of forelimb were studied from a prepared skeleton of an adult female Asian elephant (Elephas maximus) in Anatomy Museum of Chittagong Veterinary and Animal Sciences University to understand the morphological form and structure of Asian elephant forelimb. The angle was approximately 123º between caudal border of scapula and caudal border of humerus. The scapula, humerus and bones of the antebrachium (particularly the ulna) were massive bones. The bones of manus were the short and relatively small. The dorsal border of scapula extended from the level of proximal extremity of first rib to the middle of the 6th rib. Ventral angle of scapula articulated with humerus by elongated shaped glenoid cavity (cavitas glenoidalis) of scapula and head of humerus (caput humeri). The major tubercle (tuberculum majus) of humerus was situated laterally to the head, which had smaller cranial part with large caudal part and extended cranially to the head. The crest of minor tubercle (tuberculum minus) was present as the rough line on the mediocaudal surface of humerus that ends in a slight depressed or elevated area, known as teres major tuberosity (tuberositas teres major). -
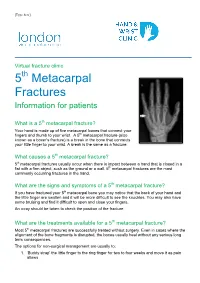
5Th Metacarpal Fractures Information for Patients
[Type here] Virtual fracture clinic 5th Metacarpal Fractures Information for patients What is a 5th metacarpal fracture? Your hand is made up of five metacarpal bones that connect your fingers and thumb to your wrist. A 5th metacarpal fracture (also known as a boxer’s fracture) is a break in the bone that connects your little finger to your wrist. A break is the same as a fracture. What causes a 5th metacarpal fracture? 5th metacarpal fractures usually occur when there is impact between a hand that is closed in a fist with a firm object, such as the ground or a wall. 5th metacarpal fractures are the most commonly occurring fractures in the hand. What are the signs and symptoms of a 5th metacarpal fracture? If you have fractured your 5th metacarpal bone you may notice that the back of your hand and the little finger are swollen and it will be more difficult to see the knuckles. You may also have some bruising and find it difficult to open and close your fingers. An x-ray should be taken to check the position of the fracture. What are the treatments available for a 5th metacarpal fracture? Most 5th metacarpal fractures are successfully treated without surgery. Even in cases where the alignment of the bone fragments is disrupted, the bones usually heal without any serious long term consequences. The options for non-surgical management are usually to: 1. ‘Buddy strap’ the little finger to the ring finger for two to four weeks and move it as pain allows 2.