The Appendicular Skeleton
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Total Volar Extrusion of the Lunate and Scaphoid Proximal Pole with Concurrent Scapholunate Dissociation
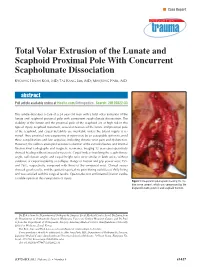
n Case Report Total Volar Extrusion of the Lunate and Scaphoid Proximal Pole With Concurrent Scapholunate Dissociation KYOUNG HWAN KOH, MD; TAE KANG LIM, MD; MIN JONG PARK, MD abstract Full article available online at Healio.com/Orthopedics. Search: 20120822-33 This article describes a case of a 24-year-old man with a total volar extrusion of the lunate and scaphoid proximal pole with concurrent scapholunate dissociation. The viability of the lunate and the proximal pole of the scaphoid are at high risk in this type of injury. Scaphoid nonunion, avascular necrosis of the lunate and proximal pole of the scaphoid, and carpal instability are inevitable unless the blood supply is re- stored. Thus, proximal row carpectomy at injury may be an acceptable option to avoid these complications and late sequelae, including chronic wrist pain and dysfunction. However, the authors attempted accurate reduction of the extruded bones and internal fixation.Final radiographs and magnetic resonance imaging 12 years postoperatively showed healing without avascular necrosis. Carpal indices involving the scapholunate angle, radiolunate angle, and carpal height ratio were similar in both wrists without evidence of carpal instability or collapse. Range of motion and grip power were 75% and 76%, respectively, compared with those of the uninjured wrist. Clinical scores showed good results, and the patient reported no pain during activities of daily living and was satisfied with his surgical results. Open reduction and internal fixation can be a viable option in this rare pattern of injury. Figure: Intraoperative photograph showing the me- dian nerve (arrow), which was compressed by the displaced lunate (asterisk) and scaphoid fracture. -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -

Parts of the Body 1) Head – Caput, Capitus 2) Skull- Cranium Cephalic- Toward the Skull Caudal- Toward the Tail Rostral- Toward the Nose 3) Collum (Pl
BIO 3330 Advanced Human Cadaver Anatomy Instructor: Dr. Jeff Simpson Department of Biology Metropolitan State College of Denver 1 PARTS OF THE BODY 1) HEAD – CAPUT, CAPITUS 2) SKULL- CRANIUM CEPHALIC- TOWARD THE SKULL CAUDAL- TOWARD THE TAIL ROSTRAL- TOWARD THE NOSE 3) COLLUM (PL. COLLI), CERVIX 4) TRUNK- THORAX, CHEST 5) ABDOMEN- AREA BETWEEN THE DIAPHRAGM AND THE HIP BONES 6) PELVIS- AREA BETWEEN OS COXAS EXTREMITIES -UPPER 1) SHOULDER GIRDLE - SCAPULA, CLAVICLE 2) BRACHIUM - ARM 3) ANTEBRACHIUM -FOREARM 4) CUBITAL FOSSA 6) METACARPALS 7) PHALANGES 2 Lower Extremities Pelvis Os Coxae (2) Inominant Bones Sacrum Coccyx Terms of Position and Direction Anatomical Position Body Erect, head, eyes and toes facing forward. Limbs at side, palms facing forward Anterior-ventral Posterior-dorsal Superficial Deep Internal/external Vertical & horizontal- refer to the body in the standing position Lateral/ medial Superior/inferior Ipsilateral Contralateral Planes of the Body Median-cuts the body into left and right halves Sagittal- parallel to median Frontal (Coronal)- divides the body into front and back halves 3 Horizontal(transverse)- cuts the body into upper and lower portions Positions of the Body Proximal Distal Limbs Radial Ulnar Tibial Fibular Foot Dorsum Plantar Hallicus HAND Dorsum- back of hand Palmar (volar)- palm side Pollicus Index finger Middle finger Ring finger Pinky finger TERMS OF MOVEMENT 1) FLEXION: DECREASE ANGLE BETWEEN TWO BONES OF A JOINT 2) EXTENSION: INCREASE ANGLE BETWEEN TWO BONES OF A JOINT 3) ADDUCTION: TOWARDS MIDLINE -

Lunate Flattening in Rheumatoid Wrists
Central Annals of Orthopedics & Rheumatology Research Article *Corresponding author Ryogo Nakamura, Nagoya Hand Center, Chunichi Hospital, 3-12-3 Marunouchi, Naka-ku, Nagoya 460- Lunate Flattening in 0002, Japan, Email: Submitted: 04 February 2014 Accepted: 28 May 2014 Rheumatoid Wrists Published: 30 May 2014 Ryogo Nakamura1, Satoshi Niwa1, Sayako Takahashi1, Etushiro Copyright © 2014 Nakamura et al. Naka1 and Masahiro Tatebe2* 1Nagoya Hand Center Chunichi Hospital, Nagoya, Japan OPEN ACCESS 2Hand and Microsurgery Center Anjo Kosei Hospital, Japan Abstract Lunate flattening was studied in 36 patients (62 wrists) with rheumatoid arthritis (RA) who were age- and gender-matched to people with normal wrists. The carpal height ratio (CHR) and lunate compression ratio (LCR; lunate height/ lunate diameter×100, Ståhl index) were measured from wrist radiographs of both groups and the lunate flattening ratio (LFR) was calculated by dividing the LCR by the CHR. The LFR reflects lunate flattening compared to carpal collapse. Twenty-four wrists underwent MRI study. T1-weighted images were evaluated for bone necrosis of the lunate. Results: the normal LFR value obtained from normal wrists ranged from 79.9 to 113.5 (mean±2SD). Lunates with RA could be classified into three groups by LFR values- lunates with a LFR above 113.5 (10 wrists, 16%), lunates with a LFR within the normal range (34 wrists, 55%), and lunates with a LFR lower than 79.9 (18 wrists, 29%). Twelve (50%) of the 24 wrists that underwent MRI study showed a low signal of the lunate in T1-weighted images showing osteonecrosis. Although a satisfactory cor- relation was not confirmed between a LFR value and a low signal on T1-weighted im- ages, lunate avascular necrosis was suspected to play a role in flattening of the lunate. -

A Thesis Entitled the Effects of Radial Core Decompression on Lunate
A Thesis entitled The Effects of Radial Core Decompression on Lunate and Scaphoid Kinematics by Andrew E. Smith Submitted to the Graduate Faculty as partial fulfillment of the requirements for the Master of Science in Mechanical Engineering Dr. Mohamed Samir Hefzy, Committee Chair Dr. Vijay Goel, Committee Member Dr. Michael Dennis, Committee Member Dr. Abdul-Azim Mustapha, Committee Member Dr. Patricia R. Komuniecki, Dean College of Graduate Studies The University of Toledo May 2012 Copyright 2012, Andrew E. Smith This document is copyrighted material. Under copyright law, no parts of this document may be reproduced without the expressed permission of the author. An Abstract of The Effects of Radial Core Decompression on Lunate and Scaphoid Kinematics by Andrew E. Smith Submitted to the Graduate Faculty as partial fulfillment of the requirements for the Master of Science in Mechanical Engineering The University of Toledo May 2012 Kienbocks disease causes degeneration of the lunate bone in the wrist leading to pain and reduced function of the joint. Clinical studies have found a new technique, radial core decompression (RCD) to be clinically effective in improving early stage Kienbock's disease. However, there have been no biomechanical studies characterizing the changes in wrist kinematics following the RCD procedure. The purpose of this study is to determine the changes in lunate and scaphoid motions following the RCD procedure. This study employs an electromagnetic 3-dimensional tracking system, Polhemus 3-SPACE to measure the motions of the lunate, scaphoid, and third metacarpal in four cadaveric specimens. Specimens were partially dissected and sutures were attached to five major tendons used for wrist motion. -

The Appendicular Skeleton the Appendicular Skeleton
The Appendicular Skeleton Figure 8–1 The Appendicular Skeleton • Allows us to move and manipulate objects • Includes all bones besides axial skeleton: – the limbs – the supportive girdles 1 The Pectoral Girdle Figure 8–2a The Pectoral Girdle • Also called the shoulder girdle • Connects the arms to the body • Positions the shoulders • Provides a base for arm movement 2 The Clavicles Figure 8–2b, c The Clavicles • Also called collarbones • Long, S-shaped bones • Originate at the manubrium (sternal end) • Articulate with the scapulae (acromial end) The Scapulae Also called shoulder blades Broad, flat triangles Articulate with arm and collarbone 3 The Scapula • Anterior surface: the subscapular fossa Body has 3 sides: – superior border – medial border (vertebral border) – lateral border (axillary border) Figure 8–3a Structures of the Scapula Figure 8–3b 4 Processes of the Glenoid Cavity • Coracoid process: – anterior, smaller •Acromion: – posterior, larger – articulates with clavicle – at the acromioclavicular joint Structures of the Scapula • Posterior surface Figure 8–3c 5 Posterior Features of the Scapula • Scapular spine: – ridge across posterior surface of body • Separates 2 regions: – supraspinous fossa – infraspinous fossa The Humerus Figure 8–4 6 Humerus • Separated by the intertubercular groove: – greater tubercle: • lateral • forms tip of shoulder – lesser tubercle: • anterior, medial •Head: – rounded, articulating surface – contained within joint capsule • Anatomical neck: – margin of joint capsule • Surgical neck: – the narrow -

Skeletal System -Appendicular System
Skeletal System -Appendicular System Chapter 8 Part B Skeleton - Divisions Total number of bones: 206 Divided into two major subdivisions: Axial system….blue Appendicular system….tan Axial system: Composed of bones that form the axis of the body. 80 bones. Appendicular system: Composed of bones that form The limbs. The bones that attach the limbs to the axial. 126 bones. Practice…Practice…Practice…Practice…Practice!! Appendicular Skeleton Appendicular system: Pectoral girdle 4 bones Upper extremity 60 bones Pelvic girdle 2 bones Lower extremity 60 bones 126 bones Appendicular Skeleton Appendicular system: Pectoral girdle 4 bones Upper extremity 60 bones Pelvic girdle 2 bones Lower extremity 60 bones 126 bones Upper Extremity/Limb Upper limbs/extremities are composed of 60 bones…30 bones in each limb: Upperarm – Humerus Forearm – Radius and Ulna Wrist – Carpals Hand – Metacarpals in palm – Phalanges in fingers and thumb Upper Extremity/Limb - Humerus Body/Shaft Humerus: long bone. Has 3 regions: Proximal end articulates with glenoid cavity of scapula. Distal end articulates with radius and ulna. Body/Shaft: diaphysis between proximal and distal ends. Has rough surface – deltoid tuberosity…for deltoid muscle attachment. Upper Extremity/Limb - Humerus Body/Shaft Humerus - Proximal end: Head: rounded projection fits into glenoid cavity of scapula. Greater and lesser tubercles: projections next to the head for muscle attachment. Intertubercular sulcus: groove between the tubercles accommodates tendon of an arm muscle. Upper Extremity/Limb - Humerus Body/Shaft Humerus - Distal end: Anterior surface: Capitulum: small, rounded knob articulates with proximal end of radius of forearm. Trochlea: spool-shaped structure articulates with proximal end of ulna of forearm. -

Ulnar Variance and the Shape of the Lunate Bone a Radiological Investigation
ULNAR VARIANCE AND THE SHAPE OF THE LUNATE BONE A RADIOLOGICAL INVESTIGATION A. H. SCHUURMAN1, M. MAAS2, P. F. DIJKSTRA2, J. M. G. KAUER3 The authors designed a study to test the hypothesis Ulnar variance is the roentgenographic difference that the length of the ulna might affect the shape of of the length of the ulna relative to the radius. the lunate bone because of long-term molding during Positive ulna variance or ulna plus refers to an ulna life. This might then be useful to predict the presence longer than the radius, while the opposite is true in or absence of a dynamic or static ulna plus by the the ulna minus or negative ulnar variance. shape of the lunate bone. Obermann (6) correlated lunate shape and ulnar In a prospective study, posterior-anterior wrist xrays length in 68 patients. Although he found a 13% were taken in a standard fashion in 68 patients with a mean age of 34.5 years. Dominance, grip strength, incidence of type 1, 62% type 2 and 25% type 3, he ulnar variance and the shape of the lunate were found no correlation between type 1 and ulna recorded. length (even distribution in all). Type 2 was found Lunate shape, type 1, which is the least molded, was less often in the ulna minus group and type 3 was seen most frequently on both the left and right side most often found in the ulna plus group. Unfortu- and did not correlate with the dominant side. The nately no statistical analysis was performed. -

Multifocal Avascular Necrosis of the Lunate and Triquetrum in a Child
ISSN: 2469-5726 Roberts et al. J Rheum Dis Treat 2018, 4:063 DOI: 10.23937/2469-5726/1510063 Volume 4 | Issue 2 Journal of Open Access Rheumatic Diseases and Treatment CASE REPORT Multifocal Avascular Necrosis of the Lunate and Triquetrum in a Child with Systemic Lupus Erythematosus Roberts DC1*, Jester A1, Southwood T2, Johnson K3 and Oestreich K1 1 Department of Hand, Plastic and Reconstructive Surgery, Birmingham Children’s Hospital, UK Check for 2Department of Rheumatology, Birmingham Children’s Hospital, UK updates 3Department of Radiology, Birmingham Children’s Hospital, UK *Corresponding author: Darren Roberts, Department of Hand, Plastic and Reconstructive Surgery, Birmingham Children’s Hospital, UK, E-mail: [email protected] We present, to our knowledge, the first case of syn- Abstract chronous lunate and triquetral AVN in a child with SLE. Avascular necrosis is a known complication of systemic lu- The aetiology and management of carpal AVN in child- pus erythematosus. We report an unusual case of avas- cular necrosis affecting both the lunate and triquetrum in a hood SLE are also discussed based on the available lit- child with this condition. Vasculitis, synovitis and IgM anti- erature. cardiolipin antibodies were probable predisposing factors. The use of arthroscopic synovial debridement improves Case Report symptoms even in the presence of carpal chondromalacia and potentially delays the need for salvage surgery. A 14-year-old girl, diagnosed with SLE five years pre- viously, presented with a two-year history of non-trau- Introduction matic pain and stiffness of her right dominant wrist. She was able to write and self-care, however she was unable Avascular necrosis (AVN) of the carpus typically af- to partake in hand-held ball and racquet sports at school. -

Arm and Cubital Fossa
Two Minute History M1 - Anatomy Dissection: • 300 B.C Arm and Cubital Alexandrian Egypt: King Ptolemy I, its ok Fossa to dissect cadavers of executed, mummies etc… •Herophilus “Father of Anatomy” accused by a rival of DG Simpson, Ph.D. dissecting 600 criminals…..live criminals VCU Department of Anatomy •1300 AD Europe Pope Boniface VIII edict to stop dissection to reduce the flow of bodies “parted out and boiled” from the crusades. Unclear if this is broad ban or very narrow. 1 2 Dissection: Dissection: •1540 parliament passes “The United Company of Barbers and •1700’s with the expansion of medical Surgeons, dissect 4-6 executed schools cadavers are used as tuition criminals/yr (not enough even then) •Competition is very high and medical •1600’s Britain. The executed are schools actively advertise that training includes dissections etc.. dissected in public as punishment • 1628 William Harvey •1828 London had 10 full time (cardiovascular fame). Autopsy & 200 part time body snatchers (“seasonal work” at 312 bodies/yr) of live and dead…. Medicine expands and shortages develop •Inventions to foil grave robbers Harvey dissects father and sister •1828 Robert Knox….and the rest • 1740’s Lots of private medical is amazing history. schools competing for students, William Hogarth The Reward of Cruelty 3 4 market forces develop 1750-1751 Dissection: •Burke was hanged: 25,000 watched. Hare was granted immunity as crowd called “Burke Hare” •1828, knock on the •Burke dissected: 30,000 came to see the open lab door, Knox’s assistant purchases a cadaver -

Intraosseous Ganglion Cyst of the Lunate Bone: Two Case Reports with Literature Review Georgi P
ISSN: 2474-7564 Case Report Mathews Journal of Orthopedics Intraosseous Ganglion Cyst of The Lunate Bone: Two Case Reports with Literature Review Georgi P. Georgiev1, Iva N. Dimitrova2, Alexandar Iliev3, Georgi Kotov3, Boycho Landzhov3 1Department of Orthopaedics and Traumatology, University Hospital Queen Giovanna - ISUL, Medical University of Sofia, Bulgaria. 2Department of Cardiology, University Hospital St. Ekaterina, Medical University of Sofia, Bulgaria. 3Department of Anatomy, Histology and Embryology, Medical University of Sofia, Bulgaria. Corresponding Author: Georgi P. Georgiev, Department of Orthopaedics and Traumatology, University Hospital Queen Giovanna -ISUL, Medical University-Sofia, 8 Bialo more str., BG 1527, Sofia, Bulgaria, Tel: +359884 493523; Email: [email protected] Received Date: 04 Dec 2016 Copyright © 2016 Georgiev GP Accepted Date: 13 Dec 2016 Citation: Georgiev GP, Dimitrova IN, Iliev A, Kotov G, et al. Published Date: 14 Dec 2016 (2016). Intraosseous Ganglion Cyst of The Lunate Bone: Two Case Reports With Literature Review. M J Orth. 1(2): 012. ABSTRACT Intraosseous ganglia of the carpal bones are infrequent, benign, non-neoplastic bone lesions, which are observed pre- dominantly in young and middle-aged adults. The most commonly affected bones are the lunate and scaphoid, followed by the capitate, triquetrum and trapezoid bones. Carpal intraosseous ganglia are uncommon causes of chronic wrist pain. They have a broad and complex differential diagnosis based on various imaging modalities and histological examination. Treatment of such lesions involves several techniques and is associated with complete cure of the symptoms and low rate of recurrence. In this study, we present two cases with an intraosseous ganglion cyst of the lunate bone. -

Secondary Abutment Syndromes of the Wrist in Trauma: a Pictorial Essay
Mespreuve, M, et al. Secondary Abutment Syndromes of the Wrist in Trauma: A Pictorial Essay. Journal of the Belgian Society of Radiology. 2018; 102(1): 54, 1–8. DOI: https://doi.org/10.5334/jbsr.1558 PICTORIAL ESSAY Secondary Abutment Syndromes of the Wrist in Trauma: A Pictorial Essay Marc Mespreuve*,†, Karl Waked‡ and Koenraad Verstraete† Traumatic lesions of the wrist occur frequently and may give rise to underdiagnosed secondary abutment syndromes. The latter are a common cause of incapacitating pain and limited range of motion, despite minimal or even absent alterations on radiographs. Moreover, the complex wrist anatomy often results in ignorance or underappreciation of these syndromes. This paper presents a pictorial review of frequent and rare secondary abutment syndromes at the wrist joint, which – in contrast to primary abutment syndromes – are not based on anatomical variants or congenitaldeformations.Themeritofeachimagingmodalityisbrieflymentioned. Keywords: wrist; abutment; trauma; radiographs; MRI Introduction surfaces chondromalacia, subchondral cyst formation, and Traumatic wrist lesions occur frequently. Subsequently, surrounding synovitis. secondary abutment syndromes (SAS), a common cause of incapacitating pain and limited range of motion in spite Clinical manifestation of minimal or absent alterations on radiographs, may SAS may give rise to complaints, sometimes appearing years arise. They are often underappreciated due to the complex after trauma. The predominant symptoms are restricted wrist anatomy and call for a thorough analysis of all wrist motion and incapacitating pain, exacerbated by activity. components. SAS may have a negative impact on the three-dimensional The aim of this pictorial review is to present an overview hand positioning during daily activities [5].