THE WRIST JOINT by R
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Total Volar Extrusion of the Lunate and Scaphoid Proximal Pole with Concurrent Scapholunate Dissociation
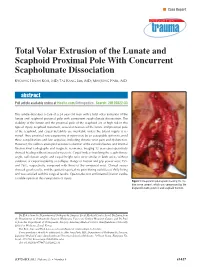
n Case Report Total Volar Extrusion of the Lunate and Scaphoid Proximal Pole With Concurrent Scapholunate Dissociation KYOUNG HWAN KOH, MD; TAE KANG LIM, MD; MIN JONG PARK, MD abstract Full article available online at Healio.com/Orthopedics. Search: 20120822-33 This article describes a case of a 24-year-old man with a total volar extrusion of the lunate and scaphoid proximal pole with concurrent scapholunate dissociation. The viability of the lunate and the proximal pole of the scaphoid are at high risk in this type of injury. Scaphoid nonunion, avascular necrosis of the lunate and proximal pole of the scaphoid, and carpal instability are inevitable unless the blood supply is re- stored. Thus, proximal row carpectomy at injury may be an acceptable option to avoid these complications and late sequelae, including chronic wrist pain and dysfunction. However, the authors attempted accurate reduction of the extruded bones and internal fixation.Final radiographs and magnetic resonance imaging 12 years postoperatively showed healing without avascular necrosis. Carpal indices involving the scapholunate angle, radiolunate angle, and carpal height ratio were similar in both wrists without evidence of carpal instability or collapse. Range of motion and grip power were 75% and 76%, respectively, compared with those of the uninjured wrist. Clinical scores showed good results, and the patient reported no pain during activities of daily living and was satisfied with his surgical results. Open reduction and internal fixation can be a viable option in this rare pattern of injury. Figure: Intraoperative photograph showing the me- dian nerve (arrow), which was compressed by the displaced lunate (asterisk) and scaphoid fracture. -

Capitate Metastases in Adenocarcinoma Lung: a Rare
Case Report Capitate Metastases in Adenocarcinoma PROVISIONAL PDF Lung: A Rare Occurrence Jaspreet KAUR1, Renu MADAN1, Maneesh Kumar VIJAY2, Pramod Kumar JULKA1, Goura Kishore RATH1 Submitted: 21 May 2014 1 Department of Radiation Oncology, DR BRA Institute Rotary Cancer Accepted: 19 Nov 2014 Hospital, All India Institute of Medical Sciences, New Delhi 110029, India 2 Department of Pathology, All India Institute of Medical Sciences, New Delhi 110029, India Abstract Metastatic carcinoma is the most common malignancy of the bone. Metastases to the upper limbs of the skeleton are extremely uncommon, with only 10–15% occurring in this region. Metastases to the hand and wrist comprise about 0.15% of all hand tumours, and only 0.1% of all metastases. Carpal bone metastases are much rarer than those to the metacarpal and phalangeal bones. They usually masquerade as more common hand pathology such as arthritis or osteomyelitis. Given the bleak prognosis of carpal metastatic disease in lung cancer, treatment of a metastasis to the hand is usually palliative. Contrary to earlier beliefs, palliative radiotherapy plays a significant role in pain relief and improving hand mobility in patients diagnosed with metastatic disease of the hand. We report a case of adenocarcinoma of the lung with metastases to the capitate bone of the carpus treated with palliative radiotherapy. Keywords: carpal bone, metastases, lung cancer, palliative, radiotherapy Introduction Case report Metastatic carcinoma is the most common A 52-year-old male presented with fever, left- malignancy of the bone. The skeleton is the sided chest pain and pain in the right wrist for two third most common site of metastases after months. -

The Cobbler's Shoes: Techniques for the Wrist and Carpal Bones
The Cobbler’s Shoes: Techniques for the Wrist and Carpal Bones. © 2008 Til Luchau, AdvancedTrainings.com (This article originally appeared in Massage and Bodywork magazine.) Just like the cobbler’s shoeless rists are amazing structures. They mediate the children, as hands‐on body therapists W relationship between our stable larger‐boned arms, we can tend to neglect our own hand and the highly mobile, sensitive dexterity of our hands. and wrist mobility. Since we use our Additionally, key structures pass through the wrists from hands so much in our work, we are arms to hands: tendons, nerves, and vessels. In this issue’s particularly prone to loosing article, I’ll talk about two effective techniques for working adaptability in our own carpal joints. with the wrist, drawing on the myofascial work as taught in Advanced‐Trainings.com’s “Advanced Myofascial Receiving the kind of work described Techniques” workshop and DVD series. As always, you here is great preventative can see video related to these techniques by visiting maintenance, and it can even increase Massage and Bodywork’s digital edition, which features a the quality of your work. Although lost clip from Advanced‐Trainings.com’s “Advanced mobility may or may not cause overt Myofascial Techniques for the Arm, Wrist, and Shoulder” symptoms, it will cause your touch to DVD set. Link available on ABMP.com and feel harder, more rigid, and less Massageandbodywork.com comfortable to your clients. It can also take a toll on your sensitivity and The carpus is the name of the boney structure formed by dexterity. -

Aneurysmal Bone Cyst of the Capitate: a Rare Case Report
)1DMG0D]KDU=0RJKLPL+<DK\D]DGHKHWDO Case Report Aneurysmal Bone Cyst of the Capitate: A rare case report )DULG1DMG0D]KDU0'1, Zahra Moghimi MD2, HoomanYahyazadeh MD2, Sareh Shahverdi MD2 Abstract Primary aneurysmal bone cyst (ABC) in the hands is rare. It occurs more commonly in metacarpal bones and involvement of carpal bones is very uncommon. We report the third case of ABC in the capitate, its clinical presentation, LPDJLQJ¿QGLQJVDQGWUHDWPHQW Keywords: Aneurysmal bone cyst, capitate, carpal bone, hand Cite this article as: Najd Mazhar F, Moghimi Z, Yahyazadeh H, Shahverdi S. Aneurysmal Bone Cyst of the Capitate: A rare case report. Arch Iran Med. 2014; 17(3): 211 – 214. Introduction measuring 15x 8x 9 mm in the capitate, without soft tissue inva- sion. Signal of the lesion was high-intensity on T2-weighted and neurysmal bone cyst (ABC) known as a benign bony le- low- intensity on T1-weighted (Figure 4 a – b). VLRQ ZDV ¿UVW LQWURGXFHG E\ Jaffe and Lichtenstein in $FFRUGLQJWRWKHLPDJLQJ¿QGLQJVa cystic lesion like aneurys- A 1942.1 ABCs may affect any part of the skeleton, but most mal bone cyst was at the top of the differential diagnosis list. We commonly involve the metaphysis RIORQJERQHVÀDWERQHVDQG approached to the lesion through a dorsal longitudinal incision. vertebral column.2 The occurrence of ABC in the hand are not Dorsal cortex was very thin and the capitate was occupied by a common, accounting for nearly 3 % to 5 % of all ABCs and are EORRG¿OOHGcystic lesion (Figure 5). The lesion was completely often occurred in the metacarpal bones.3 ABC rarely involves car- evacuated by thorough curettage and specimen sent to the histo- pal bones and only 2 cases of this tumor have been reported in the logic examination (Figure :H¿OOHGDQGLPSDFWHGWKHYRLGDUHD capitate.3 We report the third case of this tumor in the capitate with cancellous bone graft which was harvested from the ipsilat- along with its FOLQLFDO SUHVHQWDWLRQ LPDJLQJ ¿QGLQJV DQG WUHDW- eral iliac crest. -

Lunate Flattening in Rheumatoid Wrists
Central Annals of Orthopedics & Rheumatology Research Article *Corresponding author Ryogo Nakamura, Nagoya Hand Center, Chunichi Hospital, 3-12-3 Marunouchi, Naka-ku, Nagoya 460- Lunate Flattening in 0002, Japan, Email: Submitted: 04 February 2014 Accepted: 28 May 2014 Rheumatoid Wrists Published: 30 May 2014 Ryogo Nakamura1, Satoshi Niwa1, Sayako Takahashi1, Etushiro Copyright © 2014 Nakamura et al. Naka1 and Masahiro Tatebe2* 1Nagoya Hand Center Chunichi Hospital, Nagoya, Japan OPEN ACCESS 2Hand and Microsurgery Center Anjo Kosei Hospital, Japan Abstract Lunate flattening was studied in 36 patients (62 wrists) with rheumatoid arthritis (RA) who were age- and gender-matched to people with normal wrists. The carpal height ratio (CHR) and lunate compression ratio (LCR; lunate height/ lunate diameter×100, Ståhl index) were measured from wrist radiographs of both groups and the lunate flattening ratio (LFR) was calculated by dividing the LCR by the CHR. The LFR reflects lunate flattening compared to carpal collapse. Twenty-four wrists underwent MRI study. T1-weighted images were evaluated for bone necrosis of the lunate. Results: the normal LFR value obtained from normal wrists ranged from 79.9 to 113.5 (mean±2SD). Lunates with RA could be classified into three groups by LFR values- lunates with a LFR above 113.5 (10 wrists, 16%), lunates with a LFR within the normal range (34 wrists, 55%), and lunates with a LFR lower than 79.9 (18 wrists, 29%). Twelve (50%) of the 24 wrists that underwent MRI study showed a low signal of the lunate in T1-weighted images showing osteonecrosis. Although a satisfactory cor- relation was not confirmed between a LFR value and a low signal on T1-weighted im- ages, lunate avascular necrosis was suspected to play a role in flattening of the lunate. -

A Thesis Entitled the Effects of Radial Core Decompression on Lunate
A Thesis entitled The Effects of Radial Core Decompression on Lunate and Scaphoid Kinematics by Andrew E. Smith Submitted to the Graduate Faculty as partial fulfillment of the requirements for the Master of Science in Mechanical Engineering Dr. Mohamed Samir Hefzy, Committee Chair Dr. Vijay Goel, Committee Member Dr. Michael Dennis, Committee Member Dr. Abdul-Azim Mustapha, Committee Member Dr. Patricia R. Komuniecki, Dean College of Graduate Studies The University of Toledo May 2012 Copyright 2012, Andrew E. Smith This document is copyrighted material. Under copyright law, no parts of this document may be reproduced without the expressed permission of the author. An Abstract of The Effects of Radial Core Decompression on Lunate and Scaphoid Kinematics by Andrew E. Smith Submitted to the Graduate Faculty as partial fulfillment of the requirements for the Master of Science in Mechanical Engineering The University of Toledo May 2012 Kienbocks disease causes degeneration of the lunate bone in the wrist leading to pain and reduced function of the joint. Clinical studies have found a new technique, radial core decompression (RCD) to be clinically effective in improving early stage Kienbock's disease. However, there have been no biomechanical studies characterizing the changes in wrist kinematics following the RCD procedure. The purpose of this study is to determine the changes in lunate and scaphoid motions following the RCD procedure. This study employs an electromagnetic 3-dimensional tracking system, Polhemus 3-SPACE to measure the motions of the lunate, scaphoid, and third metacarpal in four cadaveric specimens. Specimens were partially dissected and sutures were attached to five major tendons used for wrist motion. -

The Appendicular Skeleton the Appendicular Skeleton
The Appendicular Skeleton Figure 8–1 The Appendicular Skeleton • Allows us to move and manipulate objects • Includes all bones besides axial skeleton: – the limbs – the supportive girdles 1 The Pectoral Girdle Figure 8–2a The Pectoral Girdle • Also called the shoulder girdle • Connects the arms to the body • Positions the shoulders • Provides a base for arm movement 2 The Clavicles Figure 8–2b, c The Clavicles • Also called collarbones • Long, S-shaped bones • Originate at the manubrium (sternal end) • Articulate with the scapulae (acromial end) The Scapulae Also called shoulder blades Broad, flat triangles Articulate with arm and collarbone 3 The Scapula • Anterior surface: the subscapular fossa Body has 3 sides: – superior border – medial border (vertebral border) – lateral border (axillary border) Figure 8–3a Structures of the Scapula Figure 8–3b 4 Processes of the Glenoid Cavity • Coracoid process: – anterior, smaller •Acromion: – posterior, larger – articulates with clavicle – at the acromioclavicular joint Structures of the Scapula • Posterior surface Figure 8–3c 5 Posterior Features of the Scapula • Scapular spine: – ridge across posterior surface of body • Separates 2 regions: – supraspinous fossa – infraspinous fossa The Humerus Figure 8–4 6 Humerus • Separated by the intertubercular groove: – greater tubercle: • lateral • forms tip of shoulder – lesser tubercle: • anterior, medial •Head: – rounded, articulating surface – contained within joint capsule • Anatomical neck: – margin of joint capsule • Surgical neck: – the narrow -

Section 1 Upper Limb Anatomy 1) with Regard to the Pectoral Girdle
Section 1 Upper Limb Anatomy 1) With regard to the pectoral girdle: a) contains three joints, the sternoclavicular, the acromioclavicular and the glenohumeral b) serratus anterior, the rhomboids and subclavius attach the scapula to the axial skeleton c) pectoralis major and deltoid are the only muscular attachments between the clavicle and the upper limb d) teres major provides attachment between the axial skeleton and the girdle 2) Choose the odd muscle out as regards insertion/origin: a) supraspinatus b) subscapularis c) biceps d) teres minor e) deltoid 3) Which muscle does not insert in or next to the intertubecular groove of the upper humerus? a) pectoralis major b) pectoralis minor c) latissimus dorsi d) teres major 4) Identify the incorrect pairing for testing muscles: a) latissimus dorsi – abduct to 60° and adduct against resistance b) trapezius – shrug shoulders against resistance c) rhomboids – place hands on hips and draw elbows back and scapulae together d) serratus anterior – push with arms outstretched against a wall 5) Identify the incorrect innervation: a) subclavius – own nerve from the brachial plexus b) serratus anterior – long thoracic nerve c) clavicular head of pectoralis major – medial pectoral nerve d) latissimus dorsi – dorsal scapular nerve e) trapezius – accessory nerve 6) Which muscle does not extend from the posterior surface of the scapula to the greater tubercle of the humerus? a) teres major b) infraspinatus c) supraspinatus d) teres minor 7) With regard to action, which muscle is the odd one out? a) teres -

Ulnar Variance and the Shape of the Lunate Bone a Radiological Investigation
ULNAR VARIANCE AND THE SHAPE OF THE LUNATE BONE A RADIOLOGICAL INVESTIGATION A. H. SCHUURMAN1, M. MAAS2, P. F. DIJKSTRA2, J. M. G. KAUER3 The authors designed a study to test the hypothesis Ulnar variance is the roentgenographic difference that the length of the ulna might affect the shape of of the length of the ulna relative to the radius. the lunate bone because of long-term molding during Positive ulna variance or ulna plus refers to an ulna life. This might then be useful to predict the presence longer than the radius, while the opposite is true in or absence of a dynamic or static ulna plus by the the ulna minus or negative ulnar variance. shape of the lunate bone. Obermann (6) correlated lunate shape and ulnar In a prospective study, posterior-anterior wrist xrays length in 68 patients. Although he found a 13% were taken in a standard fashion in 68 patients with a mean age of 34.5 years. Dominance, grip strength, incidence of type 1, 62% type 2 and 25% type 3, he ulnar variance and the shape of the lunate were found no correlation between type 1 and ulna recorded. length (even distribution in all). Type 2 was found Lunate shape, type 1, which is the least molded, was less often in the ulna minus group and type 3 was seen most frequently on both the left and right side most often found in the ulna plus group. Unfortu- and did not correlate with the dominant side. The nately no statistical analysis was performed. -
Carpal Boss in Chronic Wrist Pain and Its Association with Partial Osseous
MUSCULOSKELETAL RADIOLOGY Carpal boss in chronic wrist pain and its association with partial osseous coalition and osteoarthritis ‑ A case report with focus on MRI findings Feng Poh Department of Diagnostic Radiology, Singapore General Hospital, Singapore Address for correspondence: Dr. Feng Poh, Department of Diagnostic Radiology, Singapore General Hospital, Outram Road ‑ 168 751, Singapore. E‑mail: [email protected] ABSTRACT The carpal boss is a bony prominence at the dorsal aspect of the 2nd and/or 3rd carpometacarpal joint, which has been linked to various etiologies, including trauma, os styloideum, osteophyte formation, and partial osseous coalition. It may result in symptoms through secondary degeneration, ganglion formation, bursitis, or extensor tendon abnormalities by altered biomechanics of wrist motion. We present a case of symptomatic carpal boss with the finding of a partial osseous coalition at the 2nd carpometacarpal (metacarpal– trapezoid) joint and highlight the magnetic resonance imaging (MRI) findings of carpal boss impingement and secondary osteoarthritis. To the best of our knowledge, there is no report in the literature describing the imaging findings of partial osseous coalition and degenerative osteoarthritis in relation to carpal boss. Key words: Carpal boss; carpal coalition; chronic wrist pain; os styloideum; osteoarthritis Introduction A persistent os styloideum is the widely accepted theory behind the carpal boss and has been described as the ninth Carpal boss, also known as “carpe bossu,” is a bony carpal bone.[4,5] It represents an un‑united ossicle over prominence at the dorsal aspect of the 2nd and/or the dorsal aspect of the wrist at the base of the 2nd and 3rd carpometacarpal joint and was first described by Fiolle.[1] 3rd metacarpals. -

Fracture of the Body's Hamate Bone
THIEME 126 Case Report | Caso Cínico Fracture of the Body’sHamateBone:Open Reduction Internal Fixation by Double Approach—ACaseReport Fractura del cuerpo del ganchoso: Reducción abierta y fijación interna mediante doble abordaje—Apropósito de un caso. Jorge Salvador Marín1 Antonia Brotons Baile1 Nuria Cardona Vives1 Jaime Francisco Vargas Prieto1 José Manuel Pérez Alba1 José Fernando Martínez López1 1 Orthopedic Surgery and Trauma Service, Hospital Universitari de Address for correspondence Jorge Salvador Marín, MD, MSc, Hospital Sant Joan d’Alacant, Alicante, Spain Universitari de Sant Joan d’Alacant Ctra. Nnal. 332, Alacant-Valencia, s/n, 03550 Sant Joan d’Alacant, Alicante, Spain Rev Iberam Cir Mano 2018;46:126–130. (e-mail: [email protected]). Abstract Hamate fractures are rare. Their treatment depends on the displacement and type of fracture. We present the case and surgical technique of a 33-year-old male patient, who is a manual worker, with a displaced fracture of the body of the hamate bone associated with dislocation of the fourth and fifth metacarpal (MC) bones. The patient was Keywords operated on with a double palmar and dorsal approach directly over the hamate and ► carpal fracture the body hook, respectively, which was performed to improve the control reduction ► carpometacarpal and avoid damaging the neighboring vascular and nerve structures. The open dislocation reduction internal fixation (ORIF) was performed by inserting mini-screws in a dorsal ► double dorsal and to palmar direction. Later, the dislocations were reduced and fixed with Kirschner wires palmar approach between the fourth and fifth MC bases, and between the fourth MC base and the ► hamate fracture capitate bone. -

Multifocal Avascular Necrosis of the Lunate and Triquetrum in a Child
ISSN: 2469-5726 Roberts et al. J Rheum Dis Treat 2018, 4:063 DOI: 10.23937/2469-5726/1510063 Volume 4 | Issue 2 Journal of Open Access Rheumatic Diseases and Treatment CASE REPORT Multifocal Avascular Necrosis of the Lunate and Triquetrum in a Child with Systemic Lupus Erythematosus Roberts DC1*, Jester A1, Southwood T2, Johnson K3 and Oestreich K1 1 Department of Hand, Plastic and Reconstructive Surgery, Birmingham Children’s Hospital, UK Check for 2Department of Rheumatology, Birmingham Children’s Hospital, UK updates 3Department of Radiology, Birmingham Children’s Hospital, UK *Corresponding author: Darren Roberts, Department of Hand, Plastic and Reconstructive Surgery, Birmingham Children’s Hospital, UK, E-mail: [email protected] We present, to our knowledge, the first case of syn- Abstract chronous lunate and triquetral AVN in a child with SLE. Avascular necrosis is a known complication of systemic lu- The aetiology and management of carpal AVN in child- pus erythematosus. We report an unusual case of avas- cular necrosis affecting both the lunate and triquetrum in a hood SLE are also discussed based on the available lit- child with this condition. Vasculitis, synovitis and IgM anti- erature. cardiolipin antibodies were probable predisposing factors. The use of arthroscopic synovial debridement improves Case Report symptoms even in the presence of carpal chondromalacia and potentially delays the need for salvage surgery. A 14-year-old girl, diagnosed with SLE five years pre- viously, presented with a two-year history of non-trau- Introduction matic pain and stiffness of her right dominant wrist. She was able to write and self-care, however she was unable Avascular necrosis (AVN) of the carpus typically af- to partake in hand-held ball and racquet sports at school.