A Simple Method for Bone Age Assessment: the Capitohamate Planimetry
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Capitate Metastases in Adenocarcinoma Lung: a Rare
Case Report Capitate Metastases in Adenocarcinoma PROVISIONAL PDF Lung: A Rare Occurrence Jaspreet KAUR1, Renu MADAN1, Maneesh Kumar VIJAY2, Pramod Kumar JULKA1, Goura Kishore RATH1 Submitted: 21 May 2014 1 Department of Radiation Oncology, DR BRA Institute Rotary Cancer Accepted: 19 Nov 2014 Hospital, All India Institute of Medical Sciences, New Delhi 110029, India 2 Department of Pathology, All India Institute of Medical Sciences, New Delhi 110029, India Abstract Metastatic carcinoma is the most common malignancy of the bone. Metastases to the upper limbs of the skeleton are extremely uncommon, with only 10–15% occurring in this region. Metastases to the hand and wrist comprise about 0.15% of all hand tumours, and only 0.1% of all metastases. Carpal bone metastases are much rarer than those to the metacarpal and phalangeal bones. They usually masquerade as more common hand pathology such as arthritis or osteomyelitis. Given the bleak prognosis of carpal metastatic disease in lung cancer, treatment of a metastasis to the hand is usually palliative. Contrary to earlier beliefs, palliative radiotherapy plays a significant role in pain relief and improving hand mobility in patients diagnosed with metastatic disease of the hand. We report a case of adenocarcinoma of the lung with metastases to the capitate bone of the carpus treated with palliative radiotherapy. Keywords: carpal bone, metastases, lung cancer, palliative, radiotherapy Introduction Case report Metastatic carcinoma is the most common A 52-year-old male presented with fever, left- malignancy of the bone. The skeleton is the sided chest pain and pain in the right wrist for two third most common site of metastases after months. -

The Cobbler's Shoes: Techniques for the Wrist and Carpal Bones
The Cobbler’s Shoes: Techniques for the Wrist and Carpal Bones. © 2008 Til Luchau, AdvancedTrainings.com (This article originally appeared in Massage and Bodywork magazine.) Just like the cobbler’s shoeless rists are amazing structures. They mediate the children, as hands‐on body therapists W relationship between our stable larger‐boned arms, we can tend to neglect our own hand and the highly mobile, sensitive dexterity of our hands. and wrist mobility. Since we use our Additionally, key structures pass through the wrists from hands so much in our work, we are arms to hands: tendons, nerves, and vessels. In this issue’s particularly prone to loosing article, I’ll talk about two effective techniques for working adaptability in our own carpal joints. with the wrist, drawing on the myofascial work as taught in Advanced‐Trainings.com’s “Advanced Myofascial Receiving the kind of work described Techniques” workshop and DVD series. As always, you here is great preventative can see video related to these techniques by visiting maintenance, and it can even increase Massage and Bodywork’s digital edition, which features a the quality of your work. Although lost clip from Advanced‐Trainings.com’s “Advanced mobility may or may not cause overt Myofascial Techniques for the Arm, Wrist, and Shoulder” symptoms, it will cause your touch to DVD set. Link available on ABMP.com and feel harder, more rigid, and less Massageandbodywork.com comfortable to your clients. It can also take a toll on your sensitivity and The carpus is the name of the boney structure formed by dexterity. -

Aneurysmal Bone Cyst of the Capitate: a Rare Case Report
)1DMG0D]KDU=0RJKLPL+<DK\D]DGHKHWDO Case Report Aneurysmal Bone Cyst of the Capitate: A rare case report )DULG1DMG0D]KDU0'1, Zahra Moghimi MD2, HoomanYahyazadeh MD2, Sareh Shahverdi MD2 Abstract Primary aneurysmal bone cyst (ABC) in the hands is rare. It occurs more commonly in metacarpal bones and involvement of carpal bones is very uncommon. We report the third case of ABC in the capitate, its clinical presentation, LPDJLQJ¿QGLQJVDQGWUHDWPHQW Keywords: Aneurysmal bone cyst, capitate, carpal bone, hand Cite this article as: Najd Mazhar F, Moghimi Z, Yahyazadeh H, Shahverdi S. Aneurysmal Bone Cyst of the Capitate: A rare case report. Arch Iran Med. 2014; 17(3): 211 – 214. Introduction measuring 15x 8x 9 mm in the capitate, without soft tissue inva- sion. Signal of the lesion was high-intensity on T2-weighted and neurysmal bone cyst (ABC) known as a benign bony le- low- intensity on T1-weighted (Figure 4 a – b). VLRQ ZDV ¿UVW LQWURGXFHG E\ Jaffe and Lichtenstein in $FFRUGLQJWRWKHLPDJLQJ¿QGLQJVa cystic lesion like aneurys- A 1942.1 ABCs may affect any part of the skeleton, but most mal bone cyst was at the top of the differential diagnosis list. We commonly involve the metaphysis RIORQJERQHVÀDWERQHVDQG approached to the lesion through a dorsal longitudinal incision. vertebral column.2 The occurrence of ABC in the hand are not Dorsal cortex was very thin and the capitate was occupied by a common, accounting for nearly 3 % to 5 % of all ABCs and are EORRG¿OOHGcystic lesion (Figure 5). The lesion was completely often occurred in the metacarpal bones.3 ABC rarely involves car- evacuated by thorough curettage and specimen sent to the histo- pal bones and only 2 cases of this tumor have been reported in the logic examination (Figure :H¿OOHGDQGLPSDFWHGWKHYRLGDUHD capitate.3 We report the third case of this tumor in the capitate with cancellous bone graft which was harvested from the ipsilat- along with its FOLQLFDO SUHVHQWDWLRQ LPDJLQJ ¿QGLQJV DQG WUHDW- eral iliac crest. -

The Appendicular Skeleton the Appendicular Skeleton
The Appendicular Skeleton Figure 8–1 The Appendicular Skeleton • Allows us to move and manipulate objects • Includes all bones besides axial skeleton: – the limbs – the supportive girdles 1 The Pectoral Girdle Figure 8–2a The Pectoral Girdle • Also called the shoulder girdle • Connects the arms to the body • Positions the shoulders • Provides a base for arm movement 2 The Clavicles Figure 8–2b, c The Clavicles • Also called collarbones • Long, S-shaped bones • Originate at the manubrium (sternal end) • Articulate with the scapulae (acromial end) The Scapulae Also called shoulder blades Broad, flat triangles Articulate with arm and collarbone 3 The Scapula • Anterior surface: the subscapular fossa Body has 3 sides: – superior border – medial border (vertebral border) – lateral border (axillary border) Figure 8–3a Structures of the Scapula Figure 8–3b 4 Processes of the Glenoid Cavity • Coracoid process: – anterior, smaller •Acromion: – posterior, larger – articulates with clavicle – at the acromioclavicular joint Structures of the Scapula • Posterior surface Figure 8–3c 5 Posterior Features of the Scapula • Scapular spine: – ridge across posterior surface of body • Separates 2 regions: – supraspinous fossa – infraspinous fossa The Humerus Figure 8–4 6 Humerus • Separated by the intertubercular groove: – greater tubercle: • lateral • forms tip of shoulder – lesser tubercle: • anterior, medial •Head: – rounded, articulating surface – contained within joint capsule • Anatomical neck: – margin of joint capsule • Surgical neck: – the narrow -

Section 1 Upper Limb Anatomy 1) with Regard to the Pectoral Girdle
Section 1 Upper Limb Anatomy 1) With regard to the pectoral girdle: a) contains three joints, the sternoclavicular, the acromioclavicular and the glenohumeral b) serratus anterior, the rhomboids and subclavius attach the scapula to the axial skeleton c) pectoralis major and deltoid are the only muscular attachments between the clavicle and the upper limb d) teres major provides attachment between the axial skeleton and the girdle 2) Choose the odd muscle out as regards insertion/origin: a) supraspinatus b) subscapularis c) biceps d) teres minor e) deltoid 3) Which muscle does not insert in or next to the intertubecular groove of the upper humerus? a) pectoralis major b) pectoralis minor c) latissimus dorsi d) teres major 4) Identify the incorrect pairing for testing muscles: a) latissimus dorsi – abduct to 60° and adduct against resistance b) trapezius – shrug shoulders against resistance c) rhomboids – place hands on hips and draw elbows back and scapulae together d) serratus anterior – push with arms outstretched against a wall 5) Identify the incorrect innervation: a) subclavius – own nerve from the brachial plexus b) serratus anterior – long thoracic nerve c) clavicular head of pectoralis major – medial pectoral nerve d) latissimus dorsi – dorsal scapular nerve e) trapezius – accessory nerve 6) Which muscle does not extend from the posterior surface of the scapula to the greater tubercle of the humerus? a) teres major b) infraspinatus c) supraspinatus d) teres minor 7) With regard to action, which muscle is the odd one out? a) teres -
Carpal Boss in Chronic Wrist Pain and Its Association with Partial Osseous
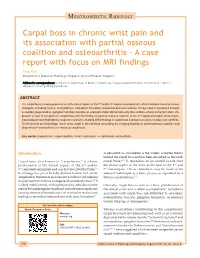
MUSCULOSKELETAL RADIOLOGY Carpal boss in chronic wrist pain and its association with partial osseous coalition and osteoarthritis ‑ A case report with focus on MRI findings Feng Poh Department of Diagnostic Radiology, Singapore General Hospital, Singapore Address for correspondence: Dr. Feng Poh, Department of Diagnostic Radiology, Singapore General Hospital, Outram Road ‑ 168 751, Singapore. E‑mail: [email protected] ABSTRACT The carpal boss is a bony prominence at the dorsal aspect of the 2nd and/or 3rd carpometacarpal joint, which has been linked to various etiologies, including trauma, os styloideum, osteophyte formation, and partial osseous coalition. It may result in symptoms through secondary degeneration, ganglion formation, bursitis, or extensor tendon abnormalities by altered biomechanics of wrist motion. We present a case of symptomatic carpal boss with the finding of a partial osseous coalition at the 2nd carpometacarpal (metacarpal– trapezoid) joint and highlight the magnetic resonance imaging (MRI) findings of carpal boss impingement and secondary osteoarthritis. To the best of our knowledge, there is no report in the literature describing the imaging findings of partial osseous coalition and degenerative osteoarthritis in relation to carpal boss. Key words: Carpal boss; carpal coalition; chronic wrist pain; os styloideum; osteoarthritis Introduction A persistent os styloideum is the widely accepted theory behind the carpal boss and has been described as the ninth Carpal boss, also known as “carpe bossu,” is a bony carpal bone.[4,5] It represents an un‑united ossicle over prominence at the dorsal aspect of the 2nd and/or the dorsal aspect of the wrist at the base of the 2nd and 3rd carpometacarpal joint and was first described by Fiolle.[1] 3rd metacarpals. -

Fracture of the Body's Hamate Bone
THIEME 126 Case Report | Caso Cínico Fracture of the Body’sHamateBone:Open Reduction Internal Fixation by Double Approach—ACaseReport Fractura del cuerpo del ganchoso: Reducción abierta y fijación interna mediante doble abordaje—Apropósito de un caso. Jorge Salvador Marín1 Antonia Brotons Baile1 Nuria Cardona Vives1 Jaime Francisco Vargas Prieto1 José Manuel Pérez Alba1 José Fernando Martínez López1 1 Orthopedic Surgery and Trauma Service, Hospital Universitari de Address for correspondence Jorge Salvador Marín, MD, MSc, Hospital Sant Joan d’Alacant, Alicante, Spain Universitari de Sant Joan d’Alacant Ctra. Nnal. 332, Alacant-Valencia, s/n, 03550 Sant Joan d’Alacant, Alicante, Spain Rev Iberam Cir Mano 2018;46:126–130. (e-mail: [email protected]). Abstract Hamate fractures are rare. Their treatment depends on the displacement and type of fracture. We present the case and surgical technique of a 33-year-old male patient, who is a manual worker, with a displaced fracture of the body of the hamate bone associated with dislocation of the fourth and fifth metacarpal (MC) bones. The patient was Keywords operated on with a double palmar and dorsal approach directly over the hamate and ► carpal fracture the body hook, respectively, which was performed to improve the control reduction ► carpometacarpal and avoid damaging the neighboring vascular and nerve structures. The open dislocation reduction internal fixation (ORIF) was performed by inserting mini-screws in a dorsal ► double dorsal and to palmar direction. Later, the dislocations were reduced and fixed with Kirschner wires palmar approach between the fourth and fifth MC bases, and between the fourth MC base and the ► hamate fracture capitate bone. -

Secondary Abutment Syndromes of the Wrist in Trauma: a Pictorial Essay
Mespreuve, M, et al. Secondary Abutment Syndromes of the Wrist in Trauma: A Pictorial Essay. Journal of the Belgian Society of Radiology. 2018; 102(1): 54, 1–8. DOI: https://doi.org/10.5334/jbsr.1558 PICTORIAL ESSAY Secondary Abutment Syndromes of the Wrist in Trauma: A Pictorial Essay Marc Mespreuve*,†, Karl Waked‡ and Koenraad Verstraete† Traumatic lesions of the wrist occur frequently and may give rise to underdiagnosed secondary abutment syndromes. The latter are a common cause of incapacitating pain and limited range of motion, despite minimal or even absent alterations on radiographs. Moreover, the complex wrist anatomy often results in ignorance or underappreciation of these syndromes. This paper presents a pictorial review of frequent and rare secondary abutment syndromes at the wrist joint, which – in contrast to primary abutment syndromes – are not based on anatomical variants or congenitaldeformations.Themeritofeachimagingmodalityisbrieflymentioned. Keywords: wrist; abutment; trauma; radiographs; MRI Introduction surfaces chondromalacia, subchondral cyst formation, and Traumatic wrist lesions occur frequently. Subsequently, surrounding synovitis. secondary abutment syndromes (SAS), a common cause of incapacitating pain and limited range of motion in spite Clinical manifestation of minimal or absent alterations on radiographs, may SAS may give rise to complaints, sometimes appearing years arise. They are often underappreciated due to the complex after trauma. The predominant symptoms are restricted wrist anatomy and call for a thorough analysis of all wrist motion and incapacitating pain, exacerbated by activity. components. SAS may have a negative impact on the three-dimensional The aim of this pictorial review is to present an overview hand positioning during daily activities [5]. -
Appendicular Muscles 355
MUSCULAR SYSTEM OUTLINE 12.1 Muscles That Move the Pectoral Girdle and Upper Limb 355 12.1a Muscles That Move the Pectoral Girdle 355 12 12.1b Muscles That Move the Glenohumeral Joint/Arm 360 12.1c Arm and Forearm Muscles That Move the Elbow Joint/Forearm 363 12.1d Forearm Muscles That Move the Wrist Joint, Appendicular Hand, and Fingers 366 12.1e Intrinsic Muscles of the Hand 374 12.2 Muscles That Move the Pelvic Girdle and Lower Limb 377 Muscles 12.2a Muscles That Move the Hip Joint/Thigh 377 12.2b Thigh Muscles That Move the Knee Joint/Leg 381 12.2c Leg Muscles 385 12.2d Intrinsic Muscles of the Foot 391 MODULE 6: MUSCULAR SYSTEM mck78097_ch12_354-396.indd 354 2/14/11 3:25 PM Chapter Twelve Appendicular Muscles 355 he appendicular muscles control the movements of the upper 2. Identify the muscles that move the scapula and their actions. T and lower limbs, and stabilize and control the movements 3. Name the muscles of the glenohumeral joint, and explain of the pectoral and pelvic girdles. These muscles are organized how each moves the humerus. into groups based on their location in the body or the part of 4. Locate and name the muscles that move the elbow joint. the skeleton they move. Beyond their individual activities, these 5. Identify the muscles of the forearm, wrist joint, fingers, muscles also work in groups that are either synergistic or antago- and thumb. nistic. Refer to figure 10.14 to review how muscles are named, and Muscles that move the pectoral girdle and upper limbs are recall the first Study Tip! from chapter 11 that gives suggestions organized into specific groups: (1) muscles that move the pectoral for learning the muscles. -

Chondroblastoma with Secondary Aneurysmal Bone Cyst of the Capitate
n Case Report Chondroblastoma With Secondary Aneurysmal Bone Cyst of the Capitate EIICHI SATO, MD, PHD; JIRO ICHIKAWA, MD, PHD; TAKASHI ANDO, MD, PHD; NOBUTAKA SATO, MD; TOMONORI KAWASAKI, MD, PHD; HIROTAKA HARO, MD, PHD abstract Full article available online at Healio.com/Orthopedics Chondroblastoma is a benign tumor that typically arises in the epiphysis of a long bone. There have been only 2 reported cases of chondroblastoma involving the cap- itate. This is the first report of chondroblastoma with secondary aneurysmal bone cyst involving the capitate. A 33-year-old man presented with a 3-year history of pain and swelling of the right wrist. Radiography as well as computed tomography Figure: Radiograph showing a lytic lesion in the showed a radiolucent area and no matrix calcification within the capitate. Magnetic capitate. resonance imaging revealed a homogeneous signal that was low on T1-weighted images and high on T2-weighted images and showed only slight enhancement. On the basis of imaging findings, the authors chose excisional biopsy. The bone tumor in the capitate was explored through a dorsal approach by dividing the extensor tendons. After repeated curettages, bone graft substitute using allograft bone was packed into the capitate. Histologically, the authors diagnosed this tumor as a chon- droblastoma with a secondary aneurysmal bone cyst. At the final 2-year follow-up, there was evidence of bone union, full range of motion, and recovery and no evi- dence of recurrence. Although the recurrence of chondroblastoma is occasionally reported, the principal treatment is intralesional curettage and bone graft. High- speed burring, phenol, bone cement, and cryosurgery have been reported to reduce local recurrence. -

Homologies of the Carpal Bones in Flying Squirrels (Pteromyinae): a Review
Mammal Study 26: 61-68 (2001) •. R . © the Mammalogical Society of Japan ' ,u" •XCTrc" Homologies of the carpal bones in flying squirrels (Pteromyinae): a review Richard W. Thorington, Jr.1 and Brian J. Stafford2 1 ^Department of Vertebrate Zoology, National Museum of Natural History, Smithsonian Institution, Washington, DC 20560-0108 USA 2Department of Anatomy, Howard University College of Medicine, 520 W Street, N.W., Washington, DC 20059 USA Abstract. The homologies of the carpal bones of flying squirrels, presented by Oshida et al. (2000a, b), are reviewed, together with the evidence supporting traditional homology assessments. Evidence for the homology of the styliform cartilage of flying squirrels with the hypothenar cartilage of other squirrels is also reviewed. Development, articulations, topography, and muscle insertions favor both the traditional hypothesis of homology assess- ments of the carpal bones and also the hypothesis that the styliform cartilage is homologous with the hypothenar cartilage. Key words: carpal homologies, flying squirrels, Pteromyinae, styliform cartilage. In two papers, Oshida et al. (2000a, b) described the styliform cartilage of flying squirrels and suggested that it is homologous with the pisiform bone of other mammals. This is a revolutionary interpretation of the homology of the carpus. It contrasts with the hypothe- sis of Thorington et al. (1998) that the styliform cartilage of flying squirrels is homologous with the hypothenar cartilage of other squirrels. In addition, the homology assessments of Oshida et al. (2000a, b) for all the proximal carpal bones differ fundamentally from the more traditional hypothesis followed by many authors, e.g. Hill (1937), Bryant (1945), Holmgren (1952), Grasse and Dekeyser (1955), Thorington (1984), Thorington et al. -

Isolated Displaced Capitate Fracture: a Case Report
Trauma Mon. 2018 May; 23(3):e59236. doi: 10.5812/traumamon.59236. Published online 2017 August 9. Case Report Isolated Displaced Capitate Fracture: A Case Report Mohammad Zarei,1 Arvin Najafi,1,* Pejman Mansouri,1 and Mahmoud Farzan1 1Joint Reconstruction Research Center, Tehran University of Medical Sciences, Tehran, Iran *Corresponding author: Arvin Najafi, Joint Reconstruction Research Center, Imam Khomeini hospital, Bagherkhan st, Tehran, Iran. Tel: +98-9128576268, Fax: +98-2161192767, E-mail: [email protected] Received 2016 October 15; Revised 2017 February 15; Accepted 2017 April 24. Abstract Introduction: Isolated fractures of the capitate account for only 0.3% of carpal bones fractures. Case Presentation: We report a motorbike rider, aged 27 years, who was involved in a motorcycle accident. He complained of right wrist pain, and wrist motion was considerably impaired. In the right wrist radiograph and CT scan, we diagnosed an isolated displaced capitate fracture. Open reduction was done under regional anaesthesia. After confirming the guide-wire’s position and reduction of the fracture by imaging, we applied a headless compression screw (HCS, Synthes, Paoli, USA). After 24 months, the patient regained pain-free activity level with 90% of grip strength (in comparison with the contralateral wrist), with extension, flexion, radial deviation, ulnar deviation, supination, and pronation of 75°, 75°, 15°, 30°, 80°, and 80°, respectively. Conclusions: This study suggested that an early diagnosis and open reduction of the displaced fragment in the treatment of such difficult fractures can lead to a successful outcome. Keywords: Capitate Bone, Fracture, Wrist Injuries 1. Introduction found isolated displaced capitate fracture (Figures 1-3).