Anatomy Lab 8- Upper Lower Limb Joints.Pub
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Total Volar Extrusion of the Lunate and Scaphoid Proximal Pole with Concurrent Scapholunate Dissociation
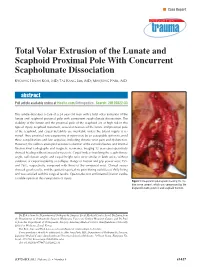
n Case Report Total Volar Extrusion of the Lunate and Scaphoid Proximal Pole With Concurrent Scapholunate Dissociation KYOUNG HWAN KOH, MD; TAE KANG LIM, MD; MIN JONG PARK, MD abstract Full article available online at Healio.com/Orthopedics. Search: 20120822-33 This article describes a case of a 24-year-old man with a total volar extrusion of the lunate and scaphoid proximal pole with concurrent scapholunate dissociation. The viability of the lunate and the proximal pole of the scaphoid are at high risk in this type of injury. Scaphoid nonunion, avascular necrosis of the lunate and proximal pole of the scaphoid, and carpal instability are inevitable unless the blood supply is re- stored. Thus, proximal row carpectomy at injury may be an acceptable option to avoid these complications and late sequelae, including chronic wrist pain and dysfunction. However, the authors attempted accurate reduction of the extruded bones and internal fixation.Final radiographs and magnetic resonance imaging 12 years postoperatively showed healing without avascular necrosis. Carpal indices involving the scapholunate angle, radiolunate angle, and carpal height ratio were similar in both wrists without evidence of carpal instability or collapse. Range of motion and grip power were 75% and 76%, respectively, compared with those of the uninjured wrist. Clinical scores showed good results, and the patient reported no pain during activities of daily living and was satisfied with his surgical results. Open reduction and internal fixation can be a viable option in this rare pattern of injury. Figure: Intraoperative photograph showing the me- dian nerve (arrow), which was compressed by the displaced lunate (asterisk) and scaphoid fracture. -

The Zona Orbicularis of the Hip Joint: Anatomical Study and Review of the Literature
Original Article www.anatomy.org.tr Received: November 30, 2017; Accepted: December 7, 2017 doi:10.2399/ana.17.047 The zona orbicularis of the hip joint: anatomical study and review of the literature Alexandra Fayne1, Peter Collin2, Melissa Duran1, Helena Kennedy2, Kiran Matthews3, R. Shane Tubbs4,5, Anthony V. D’Antoni6 1SUNY Downstate College of Medicine, New York, USA 2New York University School of Medicine, New York, USA 3City University New York, New York, USA 4Seattle Science Foundation, Seattle, WA, USA 5Department of Anatomical Sciences, St. George’s University, Grenada, West Indies 6Division of Anatomy, Department of Radiology, Weill Cornell Medical College, New York, USA Abstract Objectives: Although it is used as a landmark during various orthopedic procedures of the hip, few studies have focused on the anatomy of the zona orbicularis. Therefore, the purpose of the present research was to study its morphology to improve our understanding of its structure and potential variation. Methods: Ten adult cadavers (four males and six females) underwent dissection of the left and right hip joints to observe the morphology and location of the zona orbicularis. A digital caliper was used to measure the length and width of the zona orbic- ularis. Results: We found a zona orbicularis on all sides and that when present anteriorly, many of the inferior fibers of the zona orbic- ularis were confluent with the fibers of the iliofemoral ligament. The mean length for right sides was 35.95 mm and the mean length for left sides was 43.93 mm. The mean width for right sides was 3.74 mm and the mean width for left sides was 4.4 mm. -

Injuries to the Lower Extremity
InjuriesInjuries toto thethe LowerLower ExtremityExtremity MostMost commoncommon duedue toto applicationapplication ofof largelarge loads.loads. ImportantImportant becausebecause ofof thethe rolerole onon thethe lowerlower extremityextremity inin locomotionlocomotion HipHip AnatomyAnatomy Ball & Socket (3D) Ligament support Iliofemoral pubofemoral ischiofemoral ligamentum teres Joint capsule: labrum HipHip MusclesMuscles Flexion Extension Abduction Adduction Int. Rotation Ext. Rotation Adductors X X Tensor XXX fascia Gluteus XX Max Gluteus XX Medius Gluteus XX Minimus Gracilis X Ilopsoas X Pectinuous X X X Piriformis + + X Hamstrings X Sartorius X Rectus X Femoris HipHip fracturesfractures High energy forces falls car accidents pelvic (side impacts) high mortality rates Femoral neck fractures > 250,000 women 3 times likely to get fracture HipHip fracturesfractures Young people: high energy impacts Mechanism direct impact lateral rotation of leg Stress fractures femur Dynamic models of falls impact forces 3-10 kN HipHip LuxationLuxation (dislocation)(dislocation) Not common: hip stability High forces Most cases posterior dislocation Car accidents: dashboard Anterior inferior dislocation 10-20% of hip dislocation Force abduction Abduction, flexion and ext. rotation (obturator) Hip retroversion (toe-in) Congenital dislocation (infants) ThighThigh injuriesinjuries Three muscular compartments Ant. Medial anterior medial posterior Quadriceps contusion blunt trauma extensive hematoma swelling increase -

Compiled for Lower Limb
Updated: December, 9th, 2020 MSI ANATOMY LAB: STRUCTURE LIST Lower Extremity Lower Extremity Osteology Hip bone Tibia • Greater sciatic notch • Medial condyle • Lesser sciatic notch • Lateral condyle • Obturator foramen • Tibial plateau • Acetabulum o Medial tibial plateau o Lunate surface o Lateral tibial plateau o Acetabular notch o Intercondylar eminence • Ischiopubic ramus o Anterior intercondylar area o Posterior intercondylar area Pubic bone (pubis) • Pectineal line • Tibial tuberosity • Pubic tubercle • Medial malleolus • Body • Superior pubic ramus Patella • Inferior pubic ramus Fibula Ischium • Head • Body • Neck • Ramus • Lateral malleolus • Ischial tuberosity • Ischial spine Foot • Calcaneus Ilium o Calcaneal tuberosity • Iliac fossa o Sustentaculum tali (talar shelf) • Anterior superior iliac spine • Anterior inferior iliac spine • Talus o Head • Posterior superior iliac spine o Neck • Posterior inferior iliac spine • Arcuate line • Navicular • Iliac crest • Cuboid • Body • Cuneiforms: medial, intermediate, and lateral Femur • Metatarsals 1-5 • Greater trochanter • Phalanges 1-5 • Lesser trochanter o Proximal • Head o Middle • Neck o Distal • Linea aspera • L • Lateral condyle • L • Intercondylar fossa (notch) • L • Medial condyle • L • Lateral epicondyle • L • Medial epicondyle • L • Adductor tubercle • L • L • L • L • 1 Updated: December, 9th, 2020 Lab 3: Anterior and Medial Thigh Anterior Thigh Medial thigh General Structures Muscles • Fascia lata • Adductor longus m. • Anterior compartment • Adductor brevis m. • Medial compartment • Adductor magnus m. • Great saphenous vein o Adductor hiatus • Femoral sheath o Compartments and contents • Pectineus m. o Femoral canal and ring • Gracilis m. Muscles & Associated Tendons Nerves • Tensor fasciae lata • Obturator nerve • Iliotibial tract (band) • Femoral triangle: Boundaries Vessels o Inguinal ligament • Obturator artery o Sartorius m. • Femoral artery o Adductor longus m. -

Effects of Q-Angle on Lower Extremity Biomechanics And
EFFECTS OF Q-ANGLE ON LOWER EXTREMITY BIOMECHANICS AND INJURIES IN FEMALE COLLEGIATE TRACK AND FIELD ATHLETES By MYRANDA HOPE HAM Candidate for Master of Science in Engineering, Biomedical Engineering, Mercer University, May 2020 A Thesis Submitted to the Graduate Faculty of Mercer University School of Engineering in Partial Fulfillment of the Requirements for the Degree MASTER OF SCIENCE IN ENGINEERING MACON, GA 2020 EFFECTS OF Q-ANGLE ON LOWER EXTREMITY BIOMECHANICS AND INJURIES IN FEMALE COLLEGIATE TRACK AND FIELD ATHLETES By MYRANDA HOPE HAM Approved: ______________________________________ Date __________________ Dr. Ha Vo, Advisor ______________________________________ Date __________________ Dr. Edward O’Brien, Committee Member ______________________________________ Date __________________ Dr. Richard Kunz, Committee Member ______________________________________ Date __________________ Dr. Laura Lackey, Dean ACKNOWLEDGEMENTS I would like to first thank Dr. Vo for all his help throughout this project. I would not have been able to complete this study without his guidance. Thank you to Dr. Kunz and Dr. O’Brien for serving as member of my committee. Thank you to Amos Mansfield for approving this study to be conducted with Mercer University student-athletes. Thank you to all the Mercer Women’s Track and Field coaches, including Josh Hayman, Leesa Morales, and Jerod Wims, for being flexible and allowing the athletes to participate in this study around their practice schedule. Thank you to every member of the Mercer Women’s Track and -

Complex Knee Injuries
Journal of Orthopaedic Education219 Original Article Volume 3 Number 2, July- December 2017 DOI:http://dx.doi.org/10.21088/joe.2454.7956.3217.16 Complex Knee Injuries R.B. Uppin1, S.K.Saidapur2, ChintanN. Patel3 Author Affiliation: 1Professor, Dept. of Orthopaedics, KLE Academy of Higher Education, J.N. Medical College &Dr.PrabhakarKoreHospitalandMedicalResearchCenter,Belgaum–590010,Karnataka,India. 2Assistant Professor 3Postgraduate Student, Dept. of Orthopaedics, J.N. Medical College, Belagavi, Karnataka 590010, India. CorrespondingAuthor: R.B. Uppin, Professor, Dept. of Orthopaedics, KLE Academy of Higher Education, J.N. MedicalCollege&Dr.PrabhakarKoreHospitalandMedicalResearchCenter,Belgaum–590010,Karnataka,India. E-mail: [email protected] Received: 05October2017, Accepted on: 12October2017 Abstract AsquotedbyReneDescartes[1]“Thehumanbodyisamachinewhosemovementsaredirectedbysoul”; andkneebeingacomplexjointwithmyriadligamentsandstabilityandmayleadtovaryingdegreeof impairments.Managementoffourcomplexkneejointinjuriesfollowingtraumaarediscussedinthisarticle. Keywords:Injuries;Myriadligaments. Introduction Greatstabilitymainlydependsontheintegrityofthe ligamentousstructures. Thekneejointisthelargestandmostcomplicated synovialjointinthebody.Kneejointisamodified- hingediarthrodialsynovialjoint[2]witharticulation betweenthefemurandtibiawhichisweightbearing andthearticulationbetweenthepatellaandfemur whichallowsthepullofquadricepsfemorismuscle tobedirectedanteriorlyoverthekneetothetibia withouttendonwear.Thefibro-cartilagenous -

Board Review for Anatomy
Board Review for Anatomy John A. McNulty, Ph.D. Spring, 2005 . LOYOLA UNIVERSITY CHICAGO Stritch School of Medicine Key Skeletal landmarks • Head - mastoid process, angle of mandible, occipital protuberance • Neck – thyroid cartilage, cricoid cartilage • Thorax - jugular notch, sternal angle, xiphoid process, coracoid process, costal arch • Back - vertebra prominence, scapular spine (acromion), iliac crest • UE – epicondyles, styloid processes, carpal bones. • Pelvis – ant. sup. iliac spine, pubic tubercle • LE – head of fibula, malleoli, tarsal bones Key vertebral levels • C2 - angle of mandible • C4 - thyroid notch • C6 - cricoid cartilage - esophagus, trachea begin • C7 - vertebra prominence • T2 - jugular notch; scapular spine • T4/5 - sternal angle - rib 2 articulates, trachea divides • T9 - xiphisternum • L1/L2 - pancreas; spinal cord ends. • L4 - iliac crest; umbilicus; aorta divides • S1 - sacral promontory Upper limb nerve lesions Recall that any muscle that crosses a joint, acts on that joint. Also recall that muscles innervated by individual nerves within compartments tend to have similar actions. • Long thoracic n. - “winged” scapula. • Upper trunk (C5,C6) - Erb Duchenne - shoulder rotators, musculocutaneous • Lower trunk (C8, T1) - Klumpke’s - ulnar nerve (interossei muscle) • Radial nerve – (Saturday night palsy) - wrist drop • Median nerve (recurrent median) – thenar compartment - thumb • Ulnar nerve - interossei muscles. Lower limb nerve lesions Review actions of the various compartments. • Lumbosacral lesions - usually -

Lunate Flattening in Rheumatoid Wrists
Central Annals of Orthopedics & Rheumatology Research Article *Corresponding author Ryogo Nakamura, Nagoya Hand Center, Chunichi Hospital, 3-12-3 Marunouchi, Naka-ku, Nagoya 460- Lunate Flattening in 0002, Japan, Email: Submitted: 04 February 2014 Accepted: 28 May 2014 Rheumatoid Wrists Published: 30 May 2014 Ryogo Nakamura1, Satoshi Niwa1, Sayako Takahashi1, Etushiro Copyright © 2014 Nakamura et al. Naka1 and Masahiro Tatebe2* 1Nagoya Hand Center Chunichi Hospital, Nagoya, Japan OPEN ACCESS 2Hand and Microsurgery Center Anjo Kosei Hospital, Japan Abstract Lunate flattening was studied in 36 patients (62 wrists) with rheumatoid arthritis (RA) who were age- and gender-matched to people with normal wrists. The carpal height ratio (CHR) and lunate compression ratio (LCR; lunate height/ lunate diameter×100, Ståhl index) were measured from wrist radiographs of both groups and the lunate flattening ratio (LFR) was calculated by dividing the LCR by the CHR. The LFR reflects lunate flattening compared to carpal collapse. Twenty-four wrists underwent MRI study. T1-weighted images were evaluated for bone necrosis of the lunate. Results: the normal LFR value obtained from normal wrists ranged from 79.9 to 113.5 (mean±2SD). Lunates with RA could be classified into three groups by LFR values- lunates with a LFR above 113.5 (10 wrists, 16%), lunates with a LFR within the normal range (34 wrists, 55%), and lunates with a LFR lower than 79.9 (18 wrists, 29%). Twelve (50%) of the 24 wrists that underwent MRI study showed a low signal of the lunate in T1-weighted images showing osteonecrosis. Although a satisfactory cor- relation was not confirmed between a LFR value and a low signal on T1-weighted im- ages, lunate avascular necrosis was suspected to play a role in flattening of the lunate. -

A Thesis Entitled the Effects of Radial Core Decompression on Lunate
A Thesis entitled The Effects of Radial Core Decompression on Lunate and Scaphoid Kinematics by Andrew E. Smith Submitted to the Graduate Faculty as partial fulfillment of the requirements for the Master of Science in Mechanical Engineering Dr. Mohamed Samir Hefzy, Committee Chair Dr. Vijay Goel, Committee Member Dr. Michael Dennis, Committee Member Dr. Abdul-Azim Mustapha, Committee Member Dr. Patricia R. Komuniecki, Dean College of Graduate Studies The University of Toledo May 2012 Copyright 2012, Andrew E. Smith This document is copyrighted material. Under copyright law, no parts of this document may be reproduced without the expressed permission of the author. An Abstract of The Effects of Radial Core Decompression on Lunate and Scaphoid Kinematics by Andrew E. Smith Submitted to the Graduate Faculty as partial fulfillment of the requirements for the Master of Science in Mechanical Engineering The University of Toledo May 2012 Kienbocks disease causes degeneration of the lunate bone in the wrist leading to pain and reduced function of the joint. Clinical studies have found a new technique, radial core decompression (RCD) to be clinically effective in improving early stage Kienbock's disease. However, there have been no biomechanical studies characterizing the changes in wrist kinematics following the RCD procedure. The purpose of this study is to determine the changes in lunate and scaphoid motions following the RCD procedure. This study employs an electromagnetic 3-dimensional tracking system, Polhemus 3-SPACE to measure the motions of the lunate, scaphoid, and third metacarpal in four cadaveric specimens. Specimens were partially dissected and sutures were attached to five major tendons used for wrist motion. -

The Appendicular Skeleton the Appendicular Skeleton
The Appendicular Skeleton Figure 8–1 The Appendicular Skeleton • Allows us to move and manipulate objects • Includes all bones besides axial skeleton: – the limbs – the supportive girdles 1 The Pectoral Girdle Figure 8–2a The Pectoral Girdle • Also called the shoulder girdle • Connects the arms to the body • Positions the shoulders • Provides a base for arm movement 2 The Clavicles Figure 8–2b, c The Clavicles • Also called collarbones • Long, S-shaped bones • Originate at the manubrium (sternal end) • Articulate with the scapulae (acromial end) The Scapulae Also called shoulder blades Broad, flat triangles Articulate with arm and collarbone 3 The Scapula • Anterior surface: the subscapular fossa Body has 3 sides: – superior border – medial border (vertebral border) – lateral border (axillary border) Figure 8–3a Structures of the Scapula Figure 8–3b 4 Processes of the Glenoid Cavity • Coracoid process: – anterior, smaller •Acromion: – posterior, larger – articulates with clavicle – at the acromioclavicular joint Structures of the Scapula • Posterior surface Figure 8–3c 5 Posterior Features of the Scapula • Scapular spine: – ridge across posterior surface of body • Separates 2 regions: – supraspinous fossa – infraspinous fossa The Humerus Figure 8–4 6 Humerus • Separated by the intertubercular groove: – greater tubercle: • lateral • forms tip of shoulder – lesser tubercle: • anterior, medial •Head: – rounded, articulating surface – contained within joint capsule • Anatomical neck: – margin of joint capsule • Surgical neck: – the narrow -

Lower Extremity-Hip, Thigh, and Pelvis
Lower Extremity-Hip, Thigh, and Pelvis Basic Areas/Regions Gluteal-of or relating to or near the gluteal muscles Femoral-of or relating to the femur or thigh Pelvis-of or relating to the pelvis The pelvic girdle (pelvis) is made up of the ischium, the ilium and the pubis. On each side, the bones are fused together at the acetabulum. The two sides connect anteriorly at the pubic symphysis and posteriorly at the sacrum at the sacroiliac joints. Bones of the Pelvic Girdle Bone Landmarks Atlas Ilium 1. Iliac crest 2. Iliac tuberosity 3. Iliac fossa 4. Gluteal surface 5. Gluteal lines 6. Auricular surface 7. Arcuate line 8. Greater sciatic notch 9. Acetabulum 10. Acetabular rim 11. Acetabular notch 12. Anterior superior iliac spine (ASIS) 13. Anterior inferior iliac spine (AIIS) 14. Posterior superior iliac spine (PSIS) 15. Posterior inferior iliac spine (PIIS) Ischium 1. Ischial tuberosity 2. Ischial spine 3. Ischial ramus 4. Body of ischium 5. Lesser sciatic notch 6. Obturator foramen Pubis 1. Pubic tubercle 2. Superior pubic ramus 3. Inferior pubic ramus 4. Pubic symphysis 5. Symphyseal surface 6. Pectineal line 7. Body of pubis Femur 1. Head 2. Neck 3. Fovea capitus 4. Greater trochanter 5. Lesser trochanter 6. Intertrochanteric crest 7. Intertrochanteric line 8. Trochanteric fossa 1 9. Shaft of femur 10. Gluteal tuberosity 11. Pectineal line 12. Linea aspera 13. Adductor tubercle 14. Medial condyle 15. Lateral condyle 16. Medial epicondyle 17. Lateral epicondyle 18. Intercondylar notch 19. Intercondylar line 20. Patellar surface 21. Popliteal surface 22. Medial supracondylar line 23. -

Ulnar Variance and the Shape of the Lunate Bone a Radiological Investigation
ULNAR VARIANCE AND THE SHAPE OF THE LUNATE BONE A RADIOLOGICAL INVESTIGATION A. H. SCHUURMAN1, M. MAAS2, P. F. DIJKSTRA2, J. M. G. KAUER3 The authors designed a study to test the hypothesis Ulnar variance is the roentgenographic difference that the length of the ulna might affect the shape of of the length of the ulna relative to the radius. the lunate bone because of long-term molding during Positive ulna variance or ulna plus refers to an ulna life. This might then be useful to predict the presence longer than the radius, while the opposite is true in or absence of a dynamic or static ulna plus by the the ulna minus or negative ulnar variance. shape of the lunate bone. Obermann (6) correlated lunate shape and ulnar In a prospective study, posterior-anterior wrist xrays length in 68 patients. Although he found a 13% were taken in a standard fashion in 68 patients with a mean age of 34.5 years. Dominance, grip strength, incidence of type 1, 62% type 2 and 25% type 3, he ulnar variance and the shape of the lunate were found no correlation between type 1 and ulna recorded. length (even distribution in all). Type 2 was found Lunate shape, type 1, which is the least molded, was less often in the ulna minus group and type 3 was seen most frequently on both the left and right side most often found in the ulna plus group. Unfortu- and did not correlate with the dominant side. The nately no statistical analysis was performed.