Analysis of the Effects and Current Treatments of Laminin Deficiency
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
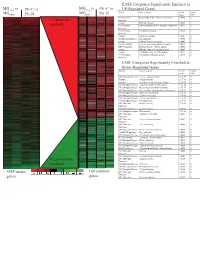
Supplement 1 Microarray Studies
EASE Categories Significantly Enriched in vs MG vs vs MGC4-2 Pt1-C vs C4-2 Pt1-C UP-Regulated Genes MG System Gene Category EASE Global MGRWV Pt1-N RWV Pt1-N Score FDR GO Molecular Extracellular matrix cellular construction 0.0008 0 110 genes up- Function Interpro EGF-like domain 0.0009 0 regulated GO Molecular Oxidoreductase activity\ acting on single dono 0.0015 0 Function GO Molecular Calcium ion binding 0.0018 0 Function Interpro Laminin-G domain 0.0025 0 GO Biological Process Cell Adhesion 0.0045 0 Interpro Collagen Triple helix repeat 0.0047 0 KEGG pathway Complement and coagulation cascades 0.0053 0 KEGG pathway Immune System – Homo sapiens 0.0053 0 Interpro Fibrillar collagen C-terminal domain 0.0062 0 Interpro Calcium-binding EGF-like domain 0.0077 0 GO Molecular Cell adhesion molecule activity 0.0105 0 Function EASE Categories Significantly Enriched in Down-Regulated Genes System Gene Category EASE Global Score FDR GO Biological Process Copper ion homeostasis 2.5E-09 0 Interpro Metallothionein 6.1E-08 0 Interpro Vertebrate metallothionein, Family 1 6.1E-08 0 GO Biological Process Transition metal ion homeostasis 8.5E-08 0 GO Biological Process Heavy metal sensitivity/resistance 1.9E-07 0 GO Biological Process Di-, tri-valent inorganic cation homeostasis 6.3E-07 0 GO Biological Process Metal ion homeostasis 6.3E-07 0 GO Biological Process Cation homeostasis 2.1E-06 0 GO Biological Process Cell ion homeostasis 2.1E-06 0 GO Biological Process Ion homeostasis 2.1E-06 0 GO Molecular Helicase activity 2.3E-06 0 Function GO Biological -

Binding of Recombinant Human Cytokeratin 19 to Laminin
CELL STRUCTURE AND FUNCTION 25: 171–175 (2000) © 2000 by Japan Society for Cell Biology Binding of Recombinant Human Cytokeratin 19 to Laminin: A Possible Role in Interaction between Intermediate Filament Derived from Epithelial Cells and Extracellular Matrixes Naomi Dobashi1, Jiro Fujita1,*, Masayuki Murota2, Yuji Ohtsuki3, Shuji Bandoh1, Yutaka Ueda1, Kazutaka Dohmoto1, Satoko Hojo1, Mikio Nishioka2, Toshihiko Ishida, and Jiro Takahara1 1First Department of Internal Medicine, Kagawa Medical University, Kagawa 2Third Department of Internal Medicine, Kagawa Medical University, Kagawa 3Department of Pathology, Kochi Medical School, Kochi, Japan ABSTRACT. Cytokeratin 8 (CK8) and cytokeratin 19 (CK19) is a specific cytoskeletal component of simple epi- thelia, including bronchial epithelial cells. We hypothesized that CK8 or CK19 released from epithelial cells may bind to and cause damage to extracellular matrixes through binding of anti-CK8 or anti-CK19 autoantibodies. In the present study, bindings of recombinant human CK8 and CK19 to laminin (both derived from mouse sarcoma cells and human), collagen, gelatin, and fibronectin were evaluated by a modified enzyme-linked immunosorbent assay (ELISA). In addition, binding of CK19 to laminin was also confirmed by inhibition assay. As a result, CK19 strongly bound to mouse laminin as well as human laminin. Pretreatment with laminin significantly reduced the binding of CK19 to laminin. However, binding of recombinant CK19 to laminin was not demonstrated by Western immunoblot, suggesting that SDS treatment of laminin diminished the binding. These results suggest that released CK19 from epithelial cells may have played a role in the damage of basement membrane by accumulation of an immune complex composed by CK19 and anti-CK19 autoantibody. -

Congenital Muscular Dystrophy Due to Laminin Α2 (Merosin) Deficiency (MDC1A) in an Ethnic Malay Girl 1MK Thong, 3Sofiah Ali,4 YE Park, 5DS Kim, 6KJ Goh, 2KT Wong
Neurology Asia 2017; 22(2) : 155 – 159 Congenital muscular dystrophy due to laminin α2 (merosin) deficiency (MDC1A) in an ethnic Malay girl 1MK Thong, 3Sofiah Ali, 4YE Park, 5DS Kim, 6KJ Goh, 2KT Wong 1Departments of Paediatrics, 2Pathology and 6Medicine, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia; 3Sime Darby Medical Centre, Subang Jaya, Selangor, Malaysia; 4Department of Neurology and Biomedical Research Institute, Pusan National University Hospital, Busan, Korea; 5Department of Neurology, Research Institute for Convergence of Biomedical Science and Technology, Pusan National University Yangsan Hospital, Yangsan, Korea Abstract We report the first known ethnic Malay patient with laminin alpha-2 (merosin) deficiency (MDC1A), a subtype of congenital muscular dystrophy (CMD)as a result of novel LAMA2 gene mutations. The 21-month-old female presented with hypotonia at birth and gross motor delay of her distal lower limbs. Physical examination showed generalised hypotonia, hyporeflexia and myopathic facies but good cognitive functions. Serum creatine kinase was elevated and white matter changes were detected in the brain MRI. Muscle biopsy showed dystrophic changes with complete laminin α2 deficiency by immunohistochemistry. Mutation analysis of LAMA2 showed compound heterozygote at exon 21, c.2888delG(p.Gly963Alafs*111) and exon 34, c.4886dupC(p.Pro1629Profs*40) leading to premature stop codon for each of the frameshift mutations. Patient review at seven years of age showed satisfactory cognitive functions despite having contractures and weakness. Genetic testing of LAMA2 related muscular dystrophy facilitated the earlier diagnosis of MDC1A and genetic counselling for this family. Keywords: laminin alpha-2 deficiency; merosin deficiency. LAMA2, Malaysia, congenital muscular dystrophy, MDC1A INTRODUCTION mutations in the laminin alpha-2 (LAMA2)gene. -

Blood Vitronectin Is a Major Activator of LIF and IL-6 in the Brain Through Integrin–FAK and Upar Signaling Matthew P
© 2018. Published by The Company of Biologists Ltd | Journal of Cell Science (2018) 131, jcs202580. doi:10.1242/jcs.202580 RESEARCH ARTICLE Blood vitronectin is a major activator of LIF and IL-6 in the brain through integrin–FAK and uPAR signaling Matthew P. Keasey1, Cuihong Jia1, Lylyan F. Pimentel1,2, Richard R. Sante1, Chiharu Lovins1 and Theo Hagg1,* ABSTRACT Microglia and astrocytes express the VTN receptors αvβ3 and α β We defined how blood-derived vitronectin (VTN) rapidly and potently v 5 integrin (Herrera-Molina et al., 2012; Kang et al., 2008; activates leukemia inhibitory factor (LIF) and pro-inflammatory Milner, 2009; Welser-Alves et al., 2011). Microglia and astrocytes, interleukin 6 (IL-6) in vitro and after vascular injury in the brain. as well as endothelial cells, are major producers of pro- α in vitro Treatment with VTN (but not fibrinogen, fibronectin, laminin-111 or inflammatory cytokines, such as IL-6 and TNF , and collagen-I) substantially increased LIF and IL-6 within 4 h in after traumatic or ischemic injury to the brain (Banner et al., 1997; C6-astroglioma cells, while VTN−/− mouse plasma was less effective Erta et al., 2012; Lau and Yu, 2001) or upon self-induction by IL-6 than that from wild-type mice. LIF and IL-6 were induced by (Van Wagoner and Benveniste, 1999). IL-6 is a major regulator of a intracerebral injection of recombinant human (rh)VTN in mice, but variety of inflammatory disorders and a target for therapies (Hunter induction seen upon intracerebral hemorrhage was less in VTN−/− and Jones, 2015). -

LAMA2-Related Muscular Dystrophy
LAMA2-related muscular dystrophy Description LAMA2-related muscular dystrophy is a disorder that causes weakness and wasting ( atrophy) of muscles used for movement (skeletal muscles). This condition varies in severity, from a severe, early-onset type to a milder, late-onset form. Early-onset LAMA2-related muscular dystrophy is apparent at birth or within the first few months of life. It is considered part of a class of muscle disorders called congenital muscular dystrophies and is sometimes called congenital muscular dystrophy type 1A. Affected infants may have severe muscle weakness, lack of muscle tone (hypotonia), little spontaneous movement, and joint deformities (contractures). Weakness of the muscles in the face and throat can result in feeding difficulties and an inability to grow and gain weight at the expected rate. Respiratory insufficiency, which occurs when muscles in the chest are weakened, causes a weak cry and breathing problems that can lead to frequent, potentially life-threatening lung infections. As affected children grow, they often develop an abnormal, gradually worsening side-to- side curvature of the spine (scoliosis) and inward curvature of the back (lordosis). Children with early-onset LAMA2-related muscular dystrophy often do not develop the ability to walk. Difficulty with speech may result from weakness of the facial muscles and an enlarged tongue. Seizures occur in about a third of individuals with early-onset LAMA2-related muscular dystrophy; rarely, heart complications occur in this form of the disorder. Symptoms of late-onset LAMA2-related muscular dystrophy become evident later in childhood or adulthood, and are similar to those of a group of muscle disorders classified as limb-girdle muscular dystrophies. -

A Dual Laminin/Collagen Receptor Acts in Peripheral Nerve Regeneration (Extracellular Matrix/Integrin) B
Proc. Nati. Acad. Sci. USA Vol. 87, pp. 1319-1322, February 1990 Neurobiology A dual laminin/collagen receptor acts in peripheral nerve regeneration (extracellular matrix/integrin) B. TOYOTA, S. CARBONETTO, AND S. DAVID Centre for Research in Neuroscience, McGill University, Montreal General Hospital Research Institute, 1650 Cedar Avenue, Montreal, PQ H3G 1A4, Canada Communicated by Richard L. Sidman, November 28, 1989 (receivedfor review July 5, 1989) ABSTRACT A regeneration chamber was created in vivo extracts not only ofPC12 cells but also ofembryonic rat neural by suturing a synthetic tube sealed at its distal end onto the tissues (26). We show here that (i) laminin coated onto the nerve proximal stump of a severed rat sciatic nerve. Nerves regen- tubes enhances sciatic nerve regeneration and (ii) mAb 3A3 erated into tubes coated with laminin at a rate of 0.33 mm/day inhibits regeneration. These data suggest that the laminin/ after a lag of about 2 days. At 25 days, regenerating nerves had collagen integrin recognized by this antibody functions in re- extended 23% farther into laminin-coated tubes as compared generation in vivo. with uncoated ones. Monoclonal antibody 3A3, which func- tionally interferes with a dual lanminin/collagen receptor, MATERIALS AND METHODS inhibited nerve regeneration into laminin-coated tubes by 32%. Cell Culture. Cultures of dissociated chicken dorsal root In contrast, monoclonal antibody JG22, which inhibits chicken ganglia were prepared as described (27). Briefly, ganglia were matrix receptors, had no significant effect on regeneration. removed from 9-day-old chicken embryos treated with trypsin Immunohistochemical studies of teased adult rat sciatic nerves (0.025%) for 20 min at 37°C. -

Decorin Gene Transfer Inhibited the Expression of Tgfβ1 and Ecm in Rat Mesangial Cells
360 EU RO PE AN JOUR NAL OF MED I CAL RE SEARCH August 16, 2007 Eur J Med Res (2007) 12: 360-368 © I. Holzapfel Publishers 2007 DECORIN GENE TRANSFER INHIBITED THE EXPRESSION OF TGFβ1 AND ECM IN RAT MESANGIAL CELLS F. Wu1, H. Yao2, A. Bader3, F. Dong2, F. Zhu1, N. Wu2, B. Wang1, H. Li1, N. H. Brockmeyer3, P. Altmeyer3 1Department of Endocrinology, the Affiliated Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Hangzhou, China; 2Institute of Infectious Diseases, the First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, China; 3Department of Dermatology and Allergy, Ruhr-University, Bochum, Germany Abstract chemistry further comfirmed that the Ad-decorin Objective: To explore the regulative role of decorin on transduced RMCs produced much less TGFβ1 com- the ECM gene-expression in diabetic nephropathy, re- pared with the Ad-lacz transduced RMCs. combinant adenovirus expressing rat decorin (Ad- Conclusion: The constructed recombinant decorin ade- decorin) was constructed to further investigat the ef- novirus can highly efficiantly express biologically ac- fects of decorin overproduction on the expression of tive decorin. Overexpression of decorin down-regu- TGFβ1 and ECM in rat mesangial cells (RMCs) in lates the expression of TGFβ1 and ECM components high glucose condition. from RMCs. These results suggest that overexpression Methods: The recombinant decorin adenovirus and of decorin may be one of the theraputic approaches lacz adenovirus(Ad-lacz), as a control, were construct- to diabetic nephropathy. ed. RT-PCR, restriction enzyme digestion, western blot and gene sequence were used for validating cor- INTRODUCTION rectness of Ad-decorin. -

Temporal and Spatial Patterns of Tenascin and Laminin Immunoreactivity Suggest Roles for Extracellular Matrix in Development of Gustatory Papillae and Taste Buds
THE .JOURNAL OF COMPARATIVE NEUROLOGY 364:535-555 ( 1996) Temporal and Spatial Patterns of Tenascin and Laminin Immunoreactivity Suggest Roles for Extracellular Matrix in Development of Gustatory Papillae and Taste Buds CHARLOTTE M. MISTRETTA AND LINDA F. HAUS Department of Biologc and Materials Sciences, School of Dentistry, University of Michigan, Ann Arbor, MI 48109-1078 ABSTRACT Gustatory papillae are complex organs that are composed of 1) an epithelium, 2) specialized sensory cells within the epithelium (the taste buds), 3) a broad connective core, and 4) sensory innervation. During papilla development, cells in the various tissue compartments must divide, aggregate, detach, migrate, and reaggregate in relation to each other, but factors that regulate such steps are poorly understood and have not been extensively studied. All of these processes potentially require participation of the extracellular matrix. Therefore, we have studied temporal and spatial patterns of immunoreactivity for two extracellular matrix molecules, tenascin and laminin, in the developing fungiform and circumvallate papillae of fetal, perinatal, and adult sheep tongue. To determine relations of tenascin and laminin to sensory innervation, we used an antibody to growth-associated protein (GAP-43)to label growing nerves. Immunocy- tochemical distributions of tenascin and laminin alter during development in a manner that reflects morphogenesis rather than histologic boundaries of the taste papillae. In early fungiform papillae, tenascin immunoreactivity is very weak within the mesenchyme of the papilla core. However, there is a subsequent shift to an intense, restricted localization in the apical papilla core only-directly under taste bud-bearing regions of the papilla epithelium. In early circumvallate papillae, tenascin immunoreactivity is patchy within the papilla core and within the flanking, nongustatory papillae. -

The Role of Laminins in Cartilaginous Tissues: from Development to Regeneration
EuropeanY Sun et al Cells. and Materials Vol. 34 2017 (pages 40-54) DOI: 10.22203/eCM.v034a03 Laminin and cartilage ISSN regeneration 1473-2262 THE ROLE OF LAMININS IN CARTILAGINOUS TISSUES: FROM DEVELOPMENT TO REGENERATION Y. Sun1,2, T.L. Wang1, W.S. Toh3 and M. Pei1,4,5,* 1 Stem Cell and Tissue Engineering Laboratory, Department of Orthopedics, West Virginia University, Morgantown, WV, USA 2 Department of Orthopedics, Orthopedics Institute, Subei People’s Hospital of Jiangsu Province, Yangzhou, Jiangsu, 225001, China 3 Faculty of Dentistry, National University of Singapore, Singapore, Republic of Singapore 4 Exercise Physiology, West Virginia University, Morgantown, WV, USA 5 Mary Babb Randolph Cancer Center, Robert C. Byrd Health Sciences Center, West Virginia University, Morgantown, WV, USA Abstract As a key molecule of extracellular matrix, laminin provides a delicate microenvironment for cell functions. Recent findings suggest that laminins expressed by cartilage-forming cells (chondrocytes, progenitor cells and stem cells) could promote chondrogenesis. However, few papers outline the effect of laminins on providing a favorable matrix microenvironment for cartilage regeneration. In this review, we delineated the expression of laminins in hyaline cartilage, fibrocartilage and cartilage-like tissue (nucleus pulposus) throughout several developmental stages. We also examined the effect of laminins on the biological activities of chondrocytes, including adhesion, migration and survival. Furthermore, we scrutinized the potential influence of various laminin isoforms on cartilage-forming cells’ proliferation and chondrogenic differentiation. With this information, we hope to facilitate an understanding of the spatial and temporal interactions between cartilage-forming cells and laminin microenvironment to eventually advance cell-based cartilage engineering and regeneration. -

The Distribution of Tenascin-X Is Distinct and Often Reciprocal To
The Distribution of Tenascin-X Is Distinct and Often Reciprocal to That of Tenascin-C Ken-ichi Matsumoto,*: Ynmiko Saga,§ Toshimichi Ikemura,~ Teruyo Sakakura,§ and Ruth Chiquet-Ehrismann* * Friedrich Miescher Institute, p.o. Box 2543, 4002 Basel, Switzerland; *Department of Evolutionary Genetics, National Institute of Genetics, Mishima, Shizuoka-ken 411, Japan; and 0RIKEN, Laboratory of Cell Biology, Tsukuba, Japan Abstract. We have isolated a cDNA encoding mouse tioned medium, as well as the purified protein bind to tenascin-X (TN-X), a new member of the family of heparin, but no binding to tenascin-C (TN-C), tenascin genes. The TN-X gene lies in the major fibronectin, laminin or collagens could be detected. histocompatibility complex (MHC) class HI region, as Thus the heparin-binding activity may be a common it is the case for its human counterpart. On Northern feature of the tenascins. The TN-X mRNA as well as blots we detected a TN-X mRNA of "013 kb in most the protein are predominantly expressed in heart and tissues analyzed, whereas in various mouse cell lines skeletal muscle, but the mRNA is found in most tis- mRNAs of "011 and 13 kb were detected, suggesting sues at a low level. Immunostaining showed the pro- the possibility of alternative splicing of TN-X tran- tein to be associated with the extracellular matrix of scripts. We raised antibodies against mouse TN-X the muscle tissues and with blood vessels in all of the fragments expressed in bacteria and used these anti- tissues analyzed. Although the TN-X gene lies in the bodies to identify the TN-X protein in heart cell ex- MHC class HI locus, it is not expressed in the lym- tracts and in the conditioned medium of a renal carci- phoid organs analyzed, except for the staining around noma cell line. -
![Lgals3bp Cell Adhesion [GO:0007155] Extracellular Matrix [GO:0031012](https://docslib.b-cdn.net/cover/7517/lgals3bp-cell-adhesion-go-0007155-extracellular-matrix-go-0031012-3317517.webp)
Lgals3bp Cell Adhesion [GO:0007155] Extracellular Matrix [GO:0031012
Supplementary material Ann Rheum Dis Gene ontology (molecular Gene.NameGene ontology (biological process) Gene ontology (cellular component) function) extracellular matrix [GO:0031012]; extracellular region [GO:0005576]; extracellular space [GO:0005615]; membrane [GO:0016020]; scavenger receptor activity Lgals3bp cell adhesion [GO:0007155] proteinaceous extracellular matrix [GO:0005578] [GO:0005044] extracellular matrix structural extracellular matrix organization [GO:0030198]; endoplasmic reticulum [GO:0005783]; extracellular constituent [GO:0005201]; hydrogen peroxide catabolic process [GO:0042744]; matrix [GO:0031012]; extracellular space heme binding [GO:0020037]; oxidation-reduction process [GO:0055114]; [GO:0005615]; proteinaceous extracellular matrix metal ion binding [GO:0046872]; Pxdn response to oxidative stress [GO:0006979] [GO:0005578] peroxidase activity carbohydrate biosynthetic process [GO:0016051]; N-acetylgalactosamine 4-O- dermatan sulfate proteoglycan metabolic process Golgi membrane [GO:0000139]; integral component sulfotransferase activity Chst14 [GO:0050655] of membrane [GO:0016021] [GO:0001537] cell-cell adhesion [GO:0098609]; cell migration [GO:0016477]; cell recognition [GO:0008037]; heterophilic cell-cell adhesion via plasma membrane cell adhesion molecules [GO:0007157]; homophilic cell adhesion via plasma membrane adhesion cell adhesion molecule binding molecules [GO:0007156]; positive regulation of [GO:0050839]; dynein light chain natural killer cell mediated cytotoxicity directed binding [GO:0045503]; protein -

Severe Congenital Muscular Dystrophy in a Mexican Family with a New Nonsense Mutation (R2578X) in the Laminin Α-2 Gene
B.J Hum Jochimsen Genet et(2003) al.: Stetteria 48:91–95 hydrogenophila © Jpn Soc Hum Genet and Springer-Verlag4600/91 2003 SHORT COMMUNICATION Ramon M. Coral-Vazquez · Haydee Rosas-Vargas Pedro Meza-Espinosa · Irma Mendoza Juan C. Huicochea · Guillermo Ramon · Fabio Salamanca Severe congenital muscular dystrophy in a Mexican family with a new nonsense mutation (R2578X) in the laminin α-2 gene Received: August 22, 2002 / Accepted: November 11, 2002 Abstract The congenital muscular dystrophies (CMDs) are Introduction a heterogeneous group of autosomal recessive disorders. Approximately one half of cases diagnosed with classic CMD show primary deficiency of the laminin α2 chain of Congenital muscular dystrophies (CMDs) are a heteroge- merosin. Complete absence of this protein is usually associ- neous group of neuromuscular disorders characterized by ated with a severe phenotype characterized by drastic muscular dystrophy and are further divided according to muscle weakness and characteristic changes in white matter different degrees of central nervous system involvement in cerebral magnetic resonance imaging (MRI). Here we (Banker 1994). In this group is included classic or pure report an 8-month-old Mexican female infant, from a con- CMD (OMIM 156225), Fukuyama CMD (OMIM 253800), sanguineous family, with classical CMD. Serum creatine α7 integrin congenital myopathy (OMIM 600536), rigid kinase was elevated, muscle biopsy showed dystrophic spin CMD (OMIM 602771), and muscle-eye-brain disease changes, and there were abnormalities in brain MRI. (OMIM 253280). The classic form of CMD without mental Immunofluorescence analysis demonstrated the complete deficiency presents muscle weakness with hypotonia and absence of laminin α2. In contrast, expression of α-, -, γ-, weakness at birth or within the first few months of life and δ-sarcoglycans and dystrophin, all components of the (Tome et al.