Importance of Histopathology in Diagnosis of Large Fibroepithelial Polyp in Oral Cavity: a Case Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Rare Presentation of Benign Brenner Tumor of Ovary: a Case Report
International Journal of Reproduction, Contraception, Obstetrics and Gynecology Periasamy S et al. Int J Reprod Contracept Obstet Gynecol. 2018 Jul;7(7):2971-2974 www.ijrcog.org pISSN 2320-1770 | eISSN 2320-1789 DOI: http://dx.doi.org/10.18203/2320-1770.ijrcog20182920 Case Report A rare presentation of benign Brenner tumor of ovary: a case report Sumathi Periasamy1, Subha Sivagami Sengodan2*, Devipriya1, Anbarasi Pandian2 1Department of Surgery, 2Department of Obstetrics and Gynaecology, Government Mohan Kumaramangalam Medical College, Salem, Tamil Nadu, India Received: 17 April 2018 Accepted: 23 May 2018 *Correspondence: Dr. Subha Sivagami Sengodan, E-mail: [email protected] Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Brenner tumors are rare ovarian tumors accounting for 2-3% of all ovarian neoplasms and about 2% of these tumors are borderline (proliferating) or malignant. These tumors are commonly seen in 4th-8th decades of life with a peak in late 40s and early 50s. Benign Brenner tumors are usually small, <2cm in diameter and often detected incidentally during surgery or on pathological examination. Authors report a case of a large, calcified benign Brenner tumor in a 55-year-old postmenopausal woman who presented with complaint of abdominal pain and mass in abdomen. Imaging revealed large complex solid cystic pelvic mass -peritoneal fibrosarcoma. She underwent laparotomy which revealed huge Brenner tumor weighing 9kg arising from left uterine cornual end extending up to epigastric region. -

Immunohistochemical and Electron Microscopic Findings in Benign Fibroepithelial Vaginal Polyps J Clin Pathol: First Published As 10.1136/Jcp.43.3.224 on 1 March 1990
224 J Clin Pathol 1990;43:224-229 Immunohistochemical and electron microscopic findings in benign fibroepithelial vaginal polyps J Clin Pathol: first published as 10.1136/jcp.43.3.224 on 1 March 1990. Downloaded from T P Rollason, P Byrne, A Williams Abstract LIGHT MICROSCOPY Eleven classic benign "fibroepithelial Sections were cut from routinely processed, polyps" of the vagina were examined paraffin wax embedded blocks at 4 gm and using a panel of immunocytochemical immunocytochemical techniques were agents. Two were also examined electron performed using a standard peroxidase- microscopically. In all cases the stellate antiperoxidase method.7 The antibodies used and multinucleate stromal cells were as follows: polyclonal rabbit characteristic of these lesions stained antimyoglobin (batch A324, Dako Ltd, High strongly for desmin, indicating muscle Wycombe, Buckinghamshire), monoclonal intermediate filament production. In anti-desmin (batch M724, Dako Ltd), mono- common with uterine fibroleiomyomata, clonal anti-epithelial membrane antigen (batch numerous mast cells were also often M613, Dako Ltd), monoclonal anti-vimentin seen. Myoglobin staining was negative. (batch M725, Dako Ltd), polyclonal rabbit Electron microscopical examination anti-cytokeratin (Bio-nuclear services, Read- confirmed that the stromal cells con- ing) and monoclonal anti cytokeratin NCL tained abundant thin filaments with focal 5D3 (batch M503, Bio-nuclear services). densities and also showed the ultrastruc- Mast cells were shown by a standard tural features usually associated with chloroacetate esterase method using pararo- myofibroblasts. saniline,8 which gave an intense red cyto- It is concluded that these tumours plasmic colouration, and by the routine would be better designated polypoid toluidine blue method. myofibroblastomas in view of the above An attempt was made to assess semiquan- findings. -

Fibro-Epithelial Polyp: Case Report with Literature Review
ISSN: 2456-8090 (online) CASE REPORT International Healthcare Research Journal 2017;1(7):14-17. DOI: 10.26440/IHRJ/01_07/116 QR CODE Fibro-Epithelial Polyp: Case Report with Literature Review RATNA SAMUDRAWAR 1, HEENA MAZHAR2, MUKESH KUMAR KASHYAP3, RUBI GUPTA4 A Oral fibroma is the most common benign soft tissue tumor caused due to continuous trauma from sharp cusp of teeth or faulty dental B restoration. It presents as sessile or occasionally pedunculated painless swelling which can be soft to firm in consistency. Its incidence occurs mostly during third to fifth decade and shows preference for female. Its occurrence corresponds with intraoral areas that are S prone to trauma such as the tongue, buccal mucosa and labial mucosa, lip, gingiva. Even with conservative surgical excision, the T lesion may recur until the source of continuous irritation persists. This article presents a case of large size oral fibroma on left alveolar R region associated with ulceration along with literature review. A C KEYWORDS: Benign Connective Tissue Tumor, Fibro-epithelial Polyp, Irritation Fibroma, Traumatic Fibroma, Focal Fibrous T Hyperplasia. K INTRODUCTION Fibroma of the oral mucosa is the most common complaint of growth in left lower back region of benign soft tissue tumor of the oral cavity derived the mouth since 4 months. History elicited that from fibrous connective tissues (CTs).1 Its the a solitary, painless growth had been observed pathogenesis lies in the fact that due to continues in his left mandibular molar region which was local trauma, a type of reactive hyperplasia of initially small in size and then it gradually fibrous tissue occurs.2 Thus, “Focal fibrous enlarged to present size of oval shape, well- hyperplasia” (FFH) term was suggested by Daley defined, pedunculated lesion. -

Soft Tissue Sarcoma Classifications
Soft Tissue Sarcoma Classifications Contents: 1. Introduction 2. Summary of SSCRG’s decisions 3. Issue by issue summary of discussions A: List of codes to be included as Soft Tissue Sarcomas B: Full list of codes discussed with decisions C: Sarcomas of neither bone nor soft tissue D: Classifications by other organisations 1. Introduction We live in an age when it is increasingly important to have ‘key facts’ and ‘headline messages’. The national registry for bone and soft tissue sarcoma want to be able to produce high level factsheets for the general public with statements such as ‘There are 2000 soft tissue sarcomas annually in England’ or ‘Survival for soft tissue sarcomas is (eg) 75%’ It is not possible to write factsheets and data briefings like this, without a shared understanding from the SSCRG about which sarcomas we wish to include in our headline statistics. The registry accepts that soft tissue sarcomas are a very complex and heterogeneous group of cancers which do not easily reduce to headline figures. We will still strive to collect all data from cancer registries about anything that is ‘like a sarcoma’. We will also produce focussed data briefings on sites such as dermatofibrosarcomas and Kaposi’s sarcomas – the aim is not to forget any sites we exclude! The majority of soft tissue sarcomas have proved fairly uncontroversial in discussions with individual members of the SSCRG, but there were 7 particular issues it was necessary to make a group decision on. This paper records the decisions made and the rationale behind these decisions. 2. Summary of SSCRG’s decisions: Include all tumours with morphology codes as listed in Appendix A for any cancer site except C40 and C41 (bone). -

Histogenesis of Ovarian Malignant Mixed Mesodermal Tumours J Clin Pathol: First Published As 10.1136/Jcp.43.4.287 on 1 April 1990
J Clin Pathol 1990;43:287-290 287 Histogenesis of ovarian malignant mixed mesodermal tumours J Clin Pathol: first published as 10.1136/jcp.43.4.287 on 1 April 1990. Downloaded from T J Clarke Abstract embedded tumour tissue were cut at 4 im and The histogenesis of ovarian malignant stained with haematoxylin and eosin, periodic mixed mesodermal tumours, which acid Schiff (PAS) before and after diastase includes the concept of metaplastic car- treatment, Caldwell and Rannie's reticulin cinoma, is controversial. Four such stain, and phosphotungstic acid haematoxylin tumours were examined for evidence of (PTAH). Sequential sections were stained by metaplastic transition from carcinoma to the indirect immunoperoxidase technique sarcoma using morphology and reticulin using monoclonal antibodies directed against stains. Consecutive sections were stained cytokeratin (PKK1 which reacts with low immunohistochemically using cyto- molecular weight cytokeratins of44, 46, 52 and keratin and vimentin to determine 54 kilodaltons), vimentin, a-l-antitrypsin and whether cells at the interface between myoglobin. Appropriate positive and negative carcinoma and sarcoma expressed both controls, with omission of specific antisera in cytokeratin and vimentin. There was no the latter, were performed. Haematoxylin and evidence ofmorphological, architectural, eosin stained sections were examined for or immunohistochemical transitions secondary fluorescence using a Leitz Dialux from carcinoma to sarcoma in the four 20ES microscope and mercury vapour light tumours studied. This suggests that source epifluorescence. ovarian malignant mixed mesodermal Four patients, aged 68, 71, 72 and 73 presen- tumours are not metaplastic carcinomas ted with abdominal distension and discomfort but are composed of histogenetically dif- and were found to have an ovarian malignant ferent elements. -

Brenner Tumor of Ovary: an Incidental Finding: a Case Report
International Journal of Reproduction, Contraception, Obstetrics and Gynecology Jodha BS et al. Int J Reprod Contracept Obstet Gynecol. 2017 Mar;6(3):1132-1135 www.ijrcog.org pISSN 2320-1770 | eISSN 2320-1789 DOI: http://dx.doi.org/10.18203/2320-1770.ijrcog20170600 Case Report Brenner tumor of ovary: an incidental finding: a case report Bhanwar Singh Jodha, Richa Garg* Department of Obstetrics and Gynecology, Umaid Hospital, Regional Institute of Maternal and Child Health, Dr. S. N. Medical College, Jodhpur, Rajasthan, India Received: 20 December 2016 Accepted: 31 January 2017 *Correspondence: Dr. Richa Garg, E-mail: [email protected] Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Brenner tumor of the ovary is very rare, mostly benign, small, and unilateral. Malignant brenner tumor is much rarer. Malignant brenner tumor of ovary closely resembles the transitional cell carcinoma of ovary. These tumors are believed to arise from urothelial metaplasia of ovarian surface epithelium. However the latter has a worse prognosis. Here we present a case of Brenner tumor of ovary in a postmenopausal woman treated surgically and its features are briefly discussed. Keywords: Brenner tumor, Ovarian neoplasm, Ultrasonography INTRODUCTION bladder epithelium.7 The Brenner tumors are usually small, solid, firm grayish knots up to 2 cm in size, Ovarian tumors are common forms of neoplasia in however, they may also be quite big, and in such cases women and it accounts for about 30.0% of female genital they usually have cystic components as a result of cystic cancers.1 Ovarian carcinoma is the fourth most common degeneration and necrosis. -

A Clinical and Histopathological Study of 122 Cases of Dermatofibroma (Benign Fibrous Histiocytoma)
Ann Dermatol Vol. 23, No. 2, 2011 DOI: 10.5021/ad.2011.23.2.185 ORIGINAL ARTICLE A Clinical and Histopathological Study of 122 Cases of Dermatofibroma (Benign Fibrous Histiocytoma) Tae Young Han, M.D., Hee Sun Chang, M.D., June Hyun Kyung Lee, M.D., Won-Mi Lee, M.D.1, Sook-Ja Son, M.D. Departments of Dermatology and 1Pathology, Eulji General Hospital, College of Medicine, Eulji University, Seoul, Korea Background: Many variants of dermatofibromas have been INTRODUCTION described, and being aware of the variants of derma- tofibromas is important to avoid misdiagnosis. Objective: Dermatofibroma (benign fibrous histiocytoma) is a We wanted to evaluate the clinical and pathologic common skin lesion and it accounts for approximately 3% characteristics of 122 cases of dermatofibromas. Methods: of the skin lesion specimens received by one derma- We retrospectively reviewed the medical records and 122 topathology laboratory1. There is a predilection for derma- biopsy specimens of 92 patients who were diagnosed with tofibroma to develop on the extremities, and particularly dermatofibroma in the Department of Dermatology at Eulji on the lower extremities of young adults. There is a female Hospital of Eulji University between January 2000 and preponderance amongst the patients with dermatofib- March 2010. Results: Nearly 80% of the cases occurred roma1. Dermatofibroma is round or ovoid, firm, dermal between the ages of 20 and 49 years, with an overall nodules and they are usually <1 cm in diameter2. The predominance of females. Over 70% of the lesions were diagnosis is usually straightforward if the classical clinical found on the extremities. -

Table of Contents
CONTENTS 1. Specimen evaluation 1 Specimen Type. 1 Clinical History. 1 Radiologic Correlation . 1 Special Studies . 1 Immunohistochemistry . 2 Electron Microscopy. 2 Genetics. 3 Recognizing Non-Soft Tissue Tumors. 3 Grading and Prognostication of Sarcomas. 3 Management of Specimen and Reporting. 4 2. Nonmalignant Fibroblastic and Myofibroblastic Tumors and Tumor-Like Lesions . 7 Nodular Fasciitis . 7 Proliferative Fasciitis and Myositis . 12 Ischemic Fasciitis . 18 Fibroma of Tendon Sheath. 21 Nuchal-Type Fibroma . 24 Gardner-Associated Fibroma. 27 Desmoplastic Fibroblastoma. 27 Elastofibroma. 34 Pleomorphic Fibroma of Skin. 39 Intranodal (Palisaded) Myofibroblastoma. 39 Other Fibroma Variants and Fibrous Proliferations . 44 Calcifying Fibrous (Pseudo)Tumor . 47 Juvenile Hyaline Fibromatosis. 52 Fibromatosis Colli. 54 Infantile Digital Fibroma/Fibromatosis. 58 Calcifying Aponeurotic Fibroma. 63 Fibrous Hamartoma of Infancy . 65 Myofibroma/Myofibromatosis . 69 Palmar/Plantar Fibromatosis. 80 Lipofibromatosis. 85 Diffuse Infantile Fibromatosis. 90 Desmoid-Type Fibromatosis . 92 Benign Fibrous Histiocytoma (Dermatofibroma). 98 xi Tumors of the Soft Tissues Non-neural Granular Cell Tumor. 104 Neurothekeoma . 104 Plexiform Fibrohistiocytic Tumor. 110 Superficial Acral Fibromyxoma . 113 Superficial Angiomyxoma (Cutaneous Myxoma). 118 Intramuscular Myxoma. 125 Juxta-articular Myxoma. 128 Aggressive Angiomyxoma . 128 Angiomyofibroblastoma. 135 Cellular Angiofibroma. 136 3. Fibroblastic/Myofibroblastic Neoplasms with Variable Biologic Potential. -
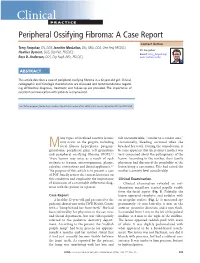
Peripheral Ossifying Fibroma: a Case Report
Clinical P RACTIC E Peripheral Ossifying Fibroma: A Case Report Contact Author Terry Farquhar, RN, DDS; Jennifer MacLellan, BSc, MSc, DDS, Cert Ped, FRCD(C); Dr. Farquhar Heather Dyment, DDS, Dip Ped, FRCD(C); Email: terry_farquhar@ Ross D. Anderson, DDS, Dip Paed, MSc, FRCD(C) urmc.rochester.edu ABSTRACT This article describes a case of peripheral ossifying fibroma in a 12-year-old girl. Clinical, radiographic and histologic characteristics are discussed and recommendations regard- ing differential diagnosis, treatment and follow-up are provided. The importance of excellent communication with patients is emphasized. For citation purposes, the electronic version is the definitive version of this article: www.cda-adc.ca/jcda/vol-74/issue-9/809.html any types of localized reactive lesions felt uncomfortable, “similar to a canker sore.” may occur on the gingiva, including Occasionally, bleeding occurred when she Mfocal fibrous hyperplasia, pyogenic brushed her teeth. During the consultation, it granuloma, peripheral giant cell granuloma became apparent that the patient’s mother was and peripheral ossifying fibroma (POF).1–3 very concerned about the pathogenesis of the These lesions may arise as a result of such lesion. According to the mother, their family irritants as trauma, microorganisms, plaque, physician had discussed the possibility of the calculus, restorations and dental appliances.2,3 lesion being a carcinoma. This had raised the The purpose of this article is to present a case mother’s anxiety level considerably. of POF, briefly review the current literature on this condition and emphasize the importance Clinical Examination of discussion of a reasonable differential diag- Clinical examination revealed an ery- nosis with the patient or a parent. -

68Yr Old Female with Post Menopausal Bleeding
Case Report Open Access J Surg Volume 7 Issue 2 - December 2017 DOI: 10.19080/OAJS.2017.07.555707 Copyright © All rights are reserved by Sushila Ladumor B 68yr Old Female with Post Menopausal Bleeding Sushila B. Ladumor1* Adham Darweesh2 1Consultant Radiologist, Clinical Imaging Department, Hamad Medical Corporation, Qatar 2Senior Consultant Radiologist, Clinical Imaging Department, Hamad Medical Corporation, Qatar Submission: November 11, 2017; Published: December 08, 2017 *Corresponding author: Sushila Ladumor B, Consultant Radiologist, Clinical Imaging Department, Hamad Medical Corporation, Assistant Professor in Clinical Radiology, Weil Cornel Medical College, Doha, Qatar, Email: Abstract (Uterine adenomyosis) With the help of recent advanced imaging plays amazing role in non-invasive diagnosis of uterine adenomyosis, usually common condition characterized by the presence of heterotopic non-malignant endometrial glands and stroma in the myometrium with hyperplasia of the adjacent smooth muscle [1]. Uterine adenomyosis is a condition in which the inner lining of the uterus (the endometrium) breaks through the muscle wall of the uterus (the myometrium). Patient can be asymptomatic or it may cause atypical pain and chronic vaginal bleeding which does not respond to usual hormonal therapy or uterine evacuation. The other common symptoms apart from pelvic pain and dysmenorrhea, menstrual cramps, lower pathology such as dysfunctional uterine bleeding, leiomyoma, and endometriosis [1]. abdominal heaviness and bloating before menstrual periods. However, these symptoms are nonspecific and can be associated with other Clinical History: bleeding. No previous Imaging or any prior consultation in system. Presenting case of uterine adenomysis and ovarian thecoma-fibroma in a 68year old lady presenting with post-menopausal Ovarian thecoma-fibroma Ovarian thecoma-fibroma groups (OTFG) are uncommon sex cord-stromal neoplasms (mesenchymal origin). -

Sclerotic Fibroma-Like Dermatofibroma: an Uncommon Distinctive Variant of Dermatofibroma
Histol Histopathol (2005) 20: 801-806 Histology and http://www.hh.um.es Histopathology Cellular and Molecular Biology Sclerotic fibroma-like dermatofibroma: an uncommon distinctive variant of dermatofibroma M.C. González-Vela1, J.F. Val-Bernal1, M. Martino1, M.A. González-López2, E. García-Alberdi1 and S. Hermana1 1Department of Anatomical Pathology and 2Service of Dermatology Marqués de Valdecilla University Hospital, Medical Faculty, University of Cantabria, Santander, Spain Summary. Dermatofibroma (DF) is a common benign Introduction cutaneous tumor with many variants based on alterations in the morphology and composition of its diverse Dermatofibroma (DF) is a common benign skin elements. One very infrequent type is sclerotic fibroma- tumor that usually occurs on the extremities, particularly like DF (SF-DF). We report 7 new cases of SF-DF. In the lower, of young or middle-aged adults (Niemi, addition, their main clinicopathological and 1970). Histologically, the tumor shows no sharp immunohistochemical features were compared with 14 circumscription and is composed of varying proportions unselected common DFs and with 3 sclerotic fibromas of fibrocytes, fibroblasts, myofibroblasts, histiocytes and (SFs). histiocytic-like cells intermixed with variable numbers Microscopically, the 7 cases of SF-DFs showed an of giant cells, foamy macrophages, siderophages, unencapsulated, well-circumscribed, hypocellular central lymphocytes and occasional plasma cells. The stroma is nodule with thick collagen bundles arranged in a composed of many small blood vessels and variable storiform pattern with prominent clefts. The overlying amounts of mature collagen (Calonje and Fletcher, epidermis was attenuated. The periphery of this nodule 1994). A wide diversity of histopathological variants of was more cellular with histopathologic features of DF has been described (Calonje and Fletcher, 1994; common DF. -

Pigmented Peduncule on the Leg
PHOTO CHALLENGE Pigmented Peduncule on the Leg Laura Catalina Arango Duque, MD; Africa Juárez Martín, MD; Beatriz Torio Sánchez, MD; María García Sánchez, MD; Cristina Bajo del Pozo, MD A 68-year-old man with a history of type 2 diabe- tes mellitus and hypercholesterolemia presented to the dermatology department with a cutaneous lesion on the posterior aspect of the right thigh of 2 years’ duration. The lesion had become larger during the 4 months prior to presentation and was mostly asymptomatic but became tender when subjected to trauma. Physical examination revealed a firm, 2-cm, slightly pigmented pedun- cule on the posterior right thigh. No lymphade- nopathies were noted. The lesion was completely excised for histologic examination. WHAT’S THE DIAGNOSIS? a. acquired fibrokeratoma b. cutaneous leiomyoma c. fibroma d. polypoid dermatofibroma e. sclerotic fibroma CUTIS DoPLEASE not TURN TO PAGEcopy E10 FOR THE DIAGNOSIS From the Complejo Asistencial Universitario de Palencia, Spain. Drs. Arango Duque, Júarez Martín, García Sánchez, and Bajo del Pozo are from the Dermatology Department. Dr. Torio Sánchez is from the Pathology Department. The authors report no conflict of interest. Correspondence: Laura Catalina Arango Duque, MD, Avenida de los Donantes de Sangre s/n, 34005, Palencia, Spain ([email protected]). WWW.MDEDGE.COM/CUTIS VOL. 101 NO. 4 I APRIL 2018 E9 Copyright Cutis 2018. No part of this publication may be reproduced, stored, or transmitted without the prior written permission of the Publisher. PHOTO CHALLENGE DISCUSSION THE DIAGNOSIS: Polypoid Dermatofibroma istologic examination revealed a poorly demarcated other DF subtypes. Requena et al5 reported 12 cases of lesion localized in the dermis that was composed giant DF, another clinical subtype, that were larger than Hof an admixture of fibroblastlike cells, histiocytes, 5 cm in diameter, most of which had a polypoid appearance.