Microbial Communities in Placentas from Term Normal Pregnancy Exhibit Spatially Variable Profiles Lindsay A
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Medical Microbiology, Virology and Immunology (General Part)
YEREVAN STATE MEDICAL UNIVERSITY AFTER MKHITAR HERATSI Department of Medical Microbiology M.S.Hovhannisyan Medical Microbiology, Virology and Immunology (General Part) Yerevan 2019 AIMS AND PROBLEMS, SHORT HISTORICAL OUTLINE ON THE DEVELOPMENT OF MICROBIOLOGY Microbiology (GK-micros-small, bios-life, logos-science) - is the science studying minute organisms, invisible to the naked eye, named microbes. Microbiology studies the laws of the life and development of microorganisms and also the changes which they bring about in animal and plant organisms and in non-living matter. The microbes are found everywhere; they are on all the subjects around us. And these microbes are subdivided into: Pathogenic – causative agents of infectious diseases Conditionally pathogenic – this can become pathogenic according to the condition. Non-pathogenic – saprophytes, which are in nature and participate in the circulation of the substances (matters). According to the requirements of society MB divided into: general agricultural veterinary sanitary medical We should study medical microbiology. Modern medical microbiology has become an extensive science. It studied the microorganisms - bacteria, viruses, fungi, which are pathogenic for the human organism. Medical microbiology is subdivided into – bacteriology – the science of bacteria, the causative agents of a number of infectious diseases; virology – the science of viruses – no cellular living systems, capable of causing infectious diseases in man; immunology – the science which is concerned with the mechanisms of body protection against pathogenic microorganisms and foreign cells and substances; mycology – the study of fungi, pathogenic for man; protozoology – which deals with pathogenic, unicellular animal organisms. Each of these disciplines studies the following problems (items): 1. Morphology and physiology which includes microscopic and other kinds of research. -

Human Microbiota Association with Immunoglobulin a and Its Participation in Immune Response La Asociación De La Microbiota Huma
Colegio Mexicano de Inmunología Clínica A.C. Revista Inmunología Alergia México Human microbiota association with immunoglobulin A and its participation in immune response La asociación de la microbiota humana con la inmunoglo- bulina A y su participación en la respuesta inmunológica Erick Saúl Sánchez-Salguero,1 Leopoldo Santos-Argumedo1 Abstract Human microbiota is the aggregate of microorganisms that reside in our body. Its phylogenetic composition is related to the risk for suff ering from infl ammatory diseases and allergic conditions. Humans interact with a large number and variety of these microorganisms via the skin and mucous membranes. An immune protection mechanism is the production of secretory IgA (SIgA), which recognizes resident pathogenic microorganisms and prevents their interaction with host epithelial cells by means of immune exclusion. Formerly, it was thought that SIgA only function in mucous membranes was to recognize and exclude pathogens, but thanks to the use of massive sequencing techniques for human microbiota phylogenetic characterization, now we know that it can be associated with pathogenic and non-pathogenic microorganisms, an association that is important for functions the microbiota carries out in epithelia, such as regulating the capability of certain microbial species to settle on the skin and mucous membranes, and stimulation and regulation of the immune response and of the risk for the development of infl ammatory problems, allergic conditions, autoimmune diseases, and even cancer. Established microbiota determines the type of bacterial species (and probably viral and protozoan species) that reside on the skin and mucous membranes, promoting microbial diversity. Keywords: Secretory Immunoglobulin A; Microbiota; Immunity; Allergy; Skin and mucosal membranes Este artículo debe citarse como: Sánchez-Salguero ES, Santos-Argumedo L. -

Contributions of the Maternal Oral and Gut Microbiome to Placental
www.nature.com/scientificreports OPEN Contributions of the maternal oral and gut microbiome to placental microbial colonization Received: 8 February 2017 Accepted: 21 April 2017 in overweight and obese pregnant Published: xx xx xxxx women Luisa F. Gomez-Arango1,2, Helen. L. Barrett 1,2,3, H. David McIntyre1,4, Leonie K. Callaway1,2,3, Mark Morrison2, 5, 6 & Marloes Dekker Nitert 2,6 A distinct bacterial signature of the placenta was reported, providing evidence that the fetus does not develop in a sterile environment. The oral microbiome was suggested as a possible source of the bacterial DNA present in the placenta based on similarities to the oral non-pregnant microbiome. Here, the possible origin of the placental microbiome was assessed, examining the gut, oral and placental microbiomes from the same pregnant women. Microbiome profiles from 37 overweight and obese pregnant women were examined by 16SrRNA sequencing. Fecal and oral contributions to the establishment of the placental microbiome were evaluated. Core phylotypes between body sites and metagenome predictive functionality were determined. The placental microbiome showed a higher resemblance and phylogenetic proximity with the pregnant oral microbiome. However, similarity decreased at lower taxonomic levels and microbiomes clustered based on tissue origin. Core genera: Prevotella, Streptococcus and Veillonella were shared between all body compartments. Pathways encoding tryptophan, fatty-acid metabolism and benzoate degradation were highly enriched specifically in the placenta. Findings demonstrate that the placental microbiome exhibits a higher resemblance with the pregnant oral microbiome. Both oral and gut microbiomes contribute to the microbial seeding of the placenta, suggesting that placental colonization may have multiple niche sources. -

Placental Microbiome and Its Association with Preterm Labor: Systematic Literature Review
Review Article ISSN: 2574 -1241 DOI: 10.26717/BJSTR.2019.17.002962 Placental Microbiome and Its Association With Preterm Labor: Systematic Literature Review Bhuchitra Singh1 and Ping Xia2* 1Department of Gynecology & Obstetrics, Johns Hopkins School of Medicine, USA 2Department of Gynecology & Obstetrics, Johns Hopkins School of Medicine, USA *Corresponding author: Ping Xia, Department of Gynecology & Obstetrics, Johns Hopkins School of Medicine, USA ARTICLE INFO abstract Received: April 09, 2019 Preterm birth is a major cause of mortality and morbidity in infants, and it is also associated with lifelong health consequences. To understand the etiology of preterm Published: April 18, 2019 labor, recent studies have looked into how the placental microbiome differs between term and preterm births, and how the microbiome affects pregnancy outcomes. This Citation: Bhuchitra Singh, Ping Xia. review synthesized selected studies (n=5) from PubMed. Overall, these studies associated Placental Microbiome and Its As- preterm labor with placental bacteria. The research indicates that the placental sociation With Preterm Labor: Sys- microbiome is similar to the human oral microbiome. Studies also show that there are tematic Literature Review. Biomed bacteria present in both term and preterm fetal membranes. Although bacteria exists in J Sci & Tech Res 17(2)-2019. BJSTR. both types, the microbes of preterm membranes are greater in prevalence and species MS.ID.002962. diversity. In addition, compared to term births, preterm births contained more microbial DNA in placentas of subjects with chorioamnionitis and without chorioamnionitis. These Keywords: Microbiome; Placenta; Placental Microbiome; Preterm Birth; variety, and preterm labor regardless of bacterial infection status. The reviewed articles Pregnancy Outcomes alsofindings lead indicateto questions a positive of proper relationship sampling between methods bacterial and contamination, presence, microbial which will DNA be discussed using the results of Salter et al. -

Sparus Aurata) and Sea Bass (Dicentrarchus Labrax)
Gut bacterial communities in geographically distant populations of farmed sea bream (Sparus aurata) and sea bass (Dicentrarchus labrax) Eleni Nikouli1, Alexandra Meziti1, Efthimia Antonopoulou2, Eleni Mente1, Konstantinos Ar. Kormas1* 1 Department of Ichthyology and Aquatic Environment, School of Agricultural Sciences, University of Thessaly, 384 46 Volos, Greece 2 Laboratory of Animal Physiology, Department of Zoology, School of Biology, Aristotle University of Thessaloniki, 541 24 Thessaloniki, Greece * Corresponding author; Tel.: +30-242-109-3082, Fax: +30-242109-3157, E-mail: [email protected], [email protected] Supplementary material 1 Table S1. Body weight of the Sparus aurata and Dicentrarchus labrax individuals used in this study. Chania Chios Igoumenitsa Yaltra Atalanti Sample Body weight S. aurata D. labrax S. aurata D. labrax S. aurata D. labrax S. aurata D. labrax S. aurata D. labrax (g) 1 359 378 558 420 433 448 481 346 260 785 2 355 294 579 442 493 556 516 397 240 340 3 376 275 468 554 450 464 540 415 440 500 4 392 395 530 460 440 483 492 493 365 860 5 420 362 483 479 542 492 406 995 6 521 505 506 461 Mean 380.40 340.80 523.17 476.67 471.60 487.75 504.50 419.67 326.25 696.00 SEs 11.89 23.76 17.36 19.56 20.46 23.85 8.68 21.00 46.79 120.29 2 Table S2. Ingredients of the diets used at the time of sampling. Ingredient Sparus aurata Dicentrarchus labrax (6 mm; 350-450 g)** (6 mm; 450-800 g)** Crude proteins (%) 42 – 44 37 – 39 Crude lipids (%) 19 – 21 20 – 22 Nitrogen free extract (NFE) (%) 20 – 26 19 – 25 Crude cellulose (%) 1 – 3 2 – 4 Ash (%) 5.8 – 7.8 6.2 – 8.2 Total P (%) 0.7 – 0.9 0.8 – 1.0 Gross energy (MJ/Kg) 21.5 – 23.5 20.6 – 22.6 Classical digestible energy* (MJ/Kg) 19.5 18.9 Added vitamin D3 (I.U./Kg) 500 500 Added vitamin E (I.U./Kg) 180 100 Added vitamin C (I.U./Kg) 250 100 Feeding rate (%), i.e. -

Does a Prenatal Bacterial Microbiota Exist?
COMMENTARY Does a prenatal bacterial microbiota exist? M Hornef1 and J Penders2 THE CONCEPT OF A PRENATAL the establishment of the neonate’s own meconium samples of 21 healthy human MICROBIOME microbiota.4 Recently, maternal-fetal neonates born by either vaginal delivery The recent technical progress and enor- transmission of commensal bacteria or caesarean section and cultured mous efforts to unravel the manifold and the existence of a placental micro- bacteria of the genera Staphylococcus, interactions of the microbiota with the biome have been suggested.5–10 Coloni- Enterococcus, Streptococcus, Leuconos- host’s organism have provided striking zation of the healthy placental and/or toc, Bifidobacterium, Rothia, Bacteroides and unforeseen insights. This work fetal tissue with a diverse group of but also of the Proteobacteria Klebsiella, assigns the microbiota a central role metabolically active bacteria would; Enterobacter and Escherichia coli.6 in human health and has identified novel however, fundamentally challenge our Again, oral administration of the labeled strategies to prevent and fight diseases in current thinking of the development of E. faecium strain to pregnant mice led to the future. One particular aspect of this the fetus within a sterile, protected the detection in meconium samples.6 work has been the early colonization of environment. It would require new They concluded the presence of the newborn and a strong influence of concepts to explain how bacteria can ‘‘mother-to-child transmission’’ before maternal sources on the developing persist within host tissue but remain birth. Three other groups described the microbiota of the neonate.1,2 Birth, or anatomically restricted to prevent sys- PCR-based detection of bacteria in more accurately rupture of the amniotic temic spread within the fetal organism placental tissue. -

Community Structure of Soil Bacteria in a Tropical Rainforest Several Years After Fire
Microbes Environ. Vol. 23, No. 1, 49–56, 2008 http://wwwsoc.nii.ac.jp/jsme2/ doi:10.1264/jsme2.23.49 Community Structure of Soil Bacteria in a Tropical Rainforest Several Years After Fire SHIGETO OTSUKA1*, IMADE SUDIANA2, AIICHIRO KOMORI1, KAZUO ISOBE1, SHIN DEGUCHI1†, MASAYA NISHIYAMA1‡, HIDEYUKI SHIMIZU3, and KEISHI SENOO1 1Department of Applied Biological Chemistry, Graduate School of Agricultural and Life Sciences, The University of Tokyo, 1–1–1 Yayoi, Bunkyo-ku, Tokyo 113–8657, Japan; 2Research Centre for Biology, The Indonesian Institute of Sciences (LIPI), Cibinong Science Centre, Jalan Raya Jakarta-Bogor Km. 46, Cibinong 16911, Indonesia; and 3Asian Environment Research Group, National Institute for Environmental Studies, 16–2 Onogawa, Tsukuba, Ibaraki 305–8506, Japan (Received July 18, 2007—Accepted November 22, 2007) The bacterial community structure in soil of a tropical rainforest in East Kalimantan, Indonesia, where forest fires occurred in 1997–1998, was analysed by denaturing gradient gel electrophoresis (DGGE) with soil samples collected from the area in 2001 and 2002. The study sites were composed of a control forest area without fire damage, a lightly- burned forest area, and a heavily-burned forest area. DGGE band patterns showed that there were many common bac- terial taxa across the areas although the vegetation is not the same. In addition, it was indicated that a change of vegeta- tion in burned areas brought the change in bacterial community structure during 2001–2002. It was also indicated that, depending on a perspective, community structure of soil bacteria in post-fire non-climax forest several years after fire can be more heterogeneous compared with that in unburned climax forest. -
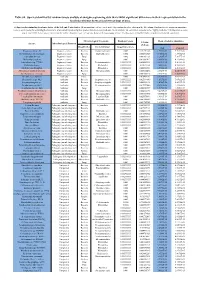
Table S8. Species Identified by Random Forests Analysis of Shotgun Sequencing Data That Exhibit Significant Differences In
Table S8. Species identified by random forests analysis of shotgun sequencing data that exhibit significant differences in their representation in the fecal microbiomes between each two groups of mice. (a) Species discriminating fecal microbiota of the Soil and Control mice. Mean importance of species identified by random forest are shown in the 5th column. Random forests assigns an importance score to each species by estimating the increase in error caused by removing that species from the set of predictors. In our analysis, we considered a species to be “highly predictive” if its importance score was at least 0.001. T-test was performed for the relative abundances of each species between the two groups of mice. P-values were at least 0.05 to be considered statistically significant. Microbiological Taxonomy Random Forests Mean of relative abundance P-Value Species Microbiological Function (T-Test) Classification Bacterial Order Importance Score Soil Control Rhodococcus sp. 2G Engineered strain Bacteria Corynebacteriales 0.002 5.73791E-05 1.9325E-05 9.3737E-06 Herminiimonas arsenitoxidans Engineered strain Bacteria Burkholderiales 0.002 0.005112829 7.1580E-05 1.3995E-05 Aspergillus ibericus Engineered strain Fungi 0.002 0.001061181 9.2368E-05 7.3057E-05 Dichomitus squalens Engineered strain Fungi 0.002 0.018887472 8.0887E-05 4.1254E-05 Acinetobacter sp. TTH0-4 Engineered strain Bacteria Pseudomonadales 0.001333333 0.025523638 2.2311E-05 8.2612E-06 Rhizobium tropici Engineered strain Bacteria Rhizobiales 0.001333333 0.02079554 7.0081E-05 4.2000E-05 Methylocystis bryophila Engineered strain Bacteria Rhizobiales 0.001333333 0.006513543 3.5401E-05 2.2044E-05 Alteromonas naphthalenivorans Engineered strain Bacteria Alteromonadales 0.001 0.000660472 2.0747E-05 4.6463E-05 Saccharomyces cerevisiae Engineered strain Fungi 0.001 0.002980726 3.9901E-05 7.3043E-05 Bacillus phage Belinda Antibiotic Phage 0.002 0.016409765 6.8789E-07 6.0681E-08 Streptomyces sp. -

When a Neonate Is Born, So Is a Microbiota
life Review When a Neonate Is Born, So Is a Microbiota Alessandra Coscia 1, Flaminia Bardanzellu 2,* , Elisa Caboni 2, Vassilios Fanos 2 and Diego Giampietro Peroni 3 1 Neonatology Unit, Department of Public Health and Pediatrics, Università degli Studi di Torino, 10124 Turin, Italy; [email protected] 2 Neonatal Intensive Care Unit, Department of Surgical Sciences, AOU and University of Cagliari, SS 554 km 4,500, 09042 Monserrato, Italy; [email protected] (E.C.); [email protected] (V.F.) 3 Clinical and Experimental Medicine Department, Section of Pediatrics, University of Pisa, Via Roma, 55, 56126 Pisa PI, Italy; [email protected] * Correspondence: bardanzellu.fl[email protected] Abstract: In recent years, the role of human microbiota as a short- and long-term health promoter and modulator has been affirmed and progressively strengthened. In the course of one’s life, each subject is colonized by a great number of bacteria, which constitute its specific and individual microbiota. Human bacterial colonization starts during fetal life, in opposition to the previous paradigm of the “sterile womb”. Placenta, amniotic fluid, cord blood and fetal tissues each have their own specific microbiota, influenced by maternal health and habits and having a decisive influence on pregnancy outcome and offspring outcome. The maternal microbiota, especially that colonizing the genital system, starts to influence the outcome of pregnancy already before conception, modulating fertility and the success rate of fertilization, even in the case of assisted reproduction techniques. During the perinatal period, neonatal microbiota seems influenced by delivery mode, drug administration and many other conditions. Special attention must be reserved for early neonatal nutrition, because breastfeeding allows the transmission of a specific and unique lactobiome able to modulate and positively affect the neonatal gut microbiota. -

Identification of Pseudomonas Species and Other Non-Glucose Fermenters
UK Standards for Microbiology Investigations Identification of Pseudomonas species and other Non- Glucose Fermenters Issued by the Standards Unit, Microbiology Services, PHE Bacteriology – Identification | ID 17 | Issue no: 3 | Issue date: 13.04.15 | Page: 1 of 41 © Crown copyright 2015 Identification of Pseudomonas species and other Non-Glucose Fermenters Acknowledgments UK Standards for Microbiology Investigations (SMIs) are developed under the auspices of Public Health England (PHE) working in partnership with the National Health Service (NHS), Public Health Wales and with the professional organisations whose logos are displayed below and listed on the website https://www.gov.uk/uk- standards-for-microbiology-investigations-smi-quality-and-consistency-in-clinical- laboratories. SMIs are developed, reviewed and revised by various working groups which are overseen by a steering committee (see https://www.gov.uk/government/groups/standards-for-microbiology-investigations- steering-committee). The contributions of many individuals in clinical, specialist and reference laboratories who have provided information and comments during the development of this document are acknowledged. We are grateful to the Medical Editors for editing the medical content. For further information please contact us at: Standards Unit Microbiology Services Public Health England 61 Colindale Avenue London NW9 5EQ E-mail: [email protected] Website: https://www.gov.uk/uk-standards-for-microbiology-investigations-smi-quality- and-consistency-in-clinical-laboratories -

Effects of Probiotics Supplementation on Placental Microbiome in Healthy Women Undergoing Spontaneous Delivery
Effects of probiotics supplementation on placental microbiome in healthy women undergoing spontaneous delivery Ping Yang The First Aliated Hospital of Jinan University Zhe Li The Third Aliated Hospital of Sun Yat-Sen University TYE KIAN DENG The First Aliated Hospital of Jinan University Tong Lu Shenzhen Long Hua District Central Hospital Yuyi Chen The First Aliated Hospital of Jinan University Zonglin He The First Aliated Hospital of Jinan University Juan Zhou The First Aliated Hospital of Jinan University Xiaomin Xiao ( [email protected] ) The First Aliated Hospital of Jinan University Research Article Keywords: probiotic, full term pregnancy, 16S rRNA sequencing, interaction network, placental microbiota Posted Date: April 21st, 2021 DOI: https://doi.org/10.21203/rs.3.rs-418396/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Effects of probiotics supplementation on placental microbiome in healthy women undergoing spontaneous delivery Ping Yang1, Zhe Li2, TYE KIAN DENG1, Tong Lu3, Yuyi Chen1, Zonglin He4, Juan Zhou1, Xiaomin Xiao1# 1Department of Obstetrics and Gynecology, The First Affiliated Hospital of Jinan University, Guangzhou, China. 2Department of Obstetrics and Gynecology, The Third Affiliated Hospital of Sun Yat-Sen University, Guangzhou, China. 3Department of Otolaryngology, Shenzhen Long Hua District Central Hospital, Shenzhen, China, 4International School, Jinan University. #Correspondence author Xiaomin Xiao [email protected] Abstract Purpose to investigate the effect of orally supplemented probiotic on term placental microbiota and provide possible evidences for clinical management of pregnant women. Methods A population-based cohort of specimens were collected from 37 healthy nulliparous pregnant women who underwent systemic examination. -

The Role of the Microbiome in the Developmental Origins of Health and Disease Leah T
The Role of the Microbiome inLeah T. Stiemsma,the PhD,Developmental Karin B. Michels, ScD, PhD Origins of Health and Disease abstract Although the prominent role of the microbiome in human health has been established, the early-life microbiome is now being recognized as a major influence on long-term human health and development. Variations in the composition and functional potential of the early-life microbiome are the result of lifestyle factors, such as mode of birth, breastfeeding, diet, and antibiotic usage. In addition, variations in the composition of the early-life NIH microbiome have been associated with specific disease outcomes, such as asthma, obesity, and neurodevelopmental disorders. This points toward Department of Epidemiology, Fielding School of Public this bacterial consortium as a mediator between early lifestyle factors and Health, University of California, Los Angeles, Los Angeles, California health and disease. In addition, variations in the microbial intrauterine environment may predispose neonates to specific health outcomes later in Dr Stiemsma conceptualized and outlined the review, conducted the literature search, drafted life. A role of the microbiome in the Developmental Origins of Health and the initial manuscript, and reviewed and revised Disease is supported in this collective research. Highlighting the early-life the manuscript; Dr Michels supervised the project critical window of susceptibility associated with microbiome development, and critically reviewed and edited the manuscript; and all authors approved the final manuscript as we discuss infant microbial colonization, beginning with the maternal- submitted and agreed to be accountable for all to-fetal exchange of microbes in utero and up through the influence of aspects of the work.