Chapter 6: Coding and Billing Basics
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Sensitive Teeth.Qxp
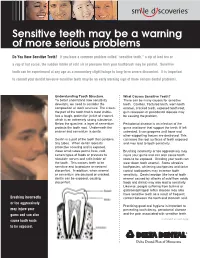
Sensitive teeth may be a warning of more serious problems Do You Have Sensitive Teeth? If you have a common problem called “sensitive teeth,” a sip of iced tea or a cup of hot cocoa, the sudden intake of cold air or pressure from your toothbrush may be painful. Sensitive teeth can be experienced at any age as a momentary slight twinge to long-term severe discomfort. It is important to consult your dentist because sensitive teeth may be an early warning sign of more serious dental problems. Understanding Tooth Structure. What Causes Sensitive Teeth? To better understand how sensitivity There can be many causes for sensitive develops, we need to consider the teeth. Cavities, fractured teeth, worn tooth composition of tooth structure. The crown- enamel, cracked teeth, exposed tooth root, the part of the tooth that is most visible- gum recession or periodontal disease may has a tough, protective jacket of enamel, be causing the problem. which is an extremely strong substance. Below the gum line, a layer of cementum Periodontal disease is an infection of the protects the tooth root. Underneath the gums and bone that support the teeth. If left enamel and cementum is dentin. untreated, it can progress until bone and other supporting tissues are destroyed. This Dentin is a part of the tooth that contains can leave the root surfaces of teeth exposed tiny tubes. When dentin loses its and may lead to tooth sensitivity. protective covering and is exposed, these small tubes permit heat, cold, Brushing incorrectly or too aggressively may certain types of foods or pressure to injure your gums and can also cause tooth stimulate nerves and cells inside of roots to be exposed. -

Hereditary Gingival Fibromatosis CASE REPORT
Richa et al.: Management of Hereditary Gingival Fibromatosis CASE REPORT Hereditary Gingival Fibromatosis and its management: A Rare Case of Homozygous Twins Richa1, Neeraj Kumar2, Krishan Gauba3, Debojyoti Chatterjee4 1-Tutor, Unit of Pedodontics and preventive dentistry, ESIC Dental College and Hospital, Rohini, Delhi. 2-Senior Resident, Unit of Pedodontics and preventive dentistry, Oral Health Sciences Centre, Post Correspondence to: Graduate Institute of Medical Education and Research , Chandigarh, India. 3-Professor and Head, Dr. Richa, Tutor, Unit of Pedodontics and Department of Oral Health Sciences Centre, Post Graduate Institute of Medical Education and preventive dentistry, ESIC Dental College and Research, Chandigarh, India. 4-Senior Resident, Department of Histopathology, Oral Health Sciences Hospital, Rohini, Delhi Centre, Post Graduate Institute of Medical Education and Research, Chandigarh, India. Contact Us: www.ijohmr.com ABSTRACT Hereditary gingival fibromatosis (HGF) is a rare condition which manifests itself by gingival overgrowth covering teeth to variable degree i.e. either isolated or as part of a syndrome. This paper presented two cases of generalized and severe HGF in siblings without any systemic illness. HGF was confirmed based on family history, clinical and histological examination. Management of both the cases was done conservatively. Quadrant wise gingivectomy using ledge and wedge method was adopted and followed for 12 months. The surgical procedure yielded functionally and esthetically satisfying results with no recurrence. KEYWORDS: Gingival enlargement, Hereditary, homozygous, Gingivectomy AA swollen gums. The patient gave a history of swelling of upper gums that started 2 years back which gradually aaaasasasss INTRODUCTION increased in size. The child’s mother denied prenatal Hereditary Gingival Enlargement, being a rare entity, is exposure to tobacco, alcohol, and drug. -
Don't We All Want Healthy Teeth and Gums? Yet Sometimes, Even with Brushing, Flossing, and Eating Healthy Foods — It Still Isn't Enough
Don't we all want healthy teeth and gums? Yet sometimes, even with brushing, flossing, and eating healthy foods — it still isn't enough. Or maybe you just want a whiter, brighter smile without the toxic ingredients in conventional products. It's herbs to the rescue! These 10 healing herbs prevent decay, and even restore. Add them to toothpaste, make them into tea, or make them into tinctures to combine into an herbal mouthwash. Herb #1 — Myrrh This is my go-to for teeth and gums. When toothache strikes, a little myrrh tincture placed on the tooth relieves pain in less than a minute. It also heals and tightens gums, cures bleeding gums, and fights bacteria that would otherwise cause gum disease and tooth decay. I use it daily as a preventative. Herb #2 — Neem Traditionally, sticks of neem were used as a natural toothbrush due to its strong antibacterial properties. Even today, it's regaining popularity. Modern research attests its ability to reduce plaque, prevent cavities and gum disease, and freshen breath. You can easily add powdered neem to your usual toothpaste. And remember, the bark is more potent than the leaf. Herb #3 — Echinacea. No, echinacea isn't just a cold-fighting herb! It also reduces inflamma- tion, boosts the immune system, and helps fight infection in the mouth. Herb #4 — Goldenseal. This herb is especially helpful for healing gums. It's antibiotic, anti- viral, and anti-inflammatory. Herb #5 — Oregon Grape Root. Antimicrobial and an astringent, Oregon grape root also soothes and tightens swollen gums. Herb #6 — Propolis. -

What Every Transplant Patient Needs to Know About Dental Care
What Every Transplant Patient Needs to Know About Dental Care International Transplant Nurses Society Should patients have that still need to be done. Taking gums each day because they don’t feel a dental exam before care of your teeth and gums (oral well. So some patients already have hygiene) is important for everyone. dental problems before they receive having a transplant? For people who are waiting for an a transplant. After transplant, you Transplant candidates should have a organ transplant and for those who may have been more concerned about dental check-up as part of the pre- have received organ transplants, problems like rejection, infection, transplant evaluation. It is helpful to maintaining healthy teeth and gums is or side effects of your medications. have an examination by your dentist an essential area of care. This booklet Because you are now taking medicines when you are being evaluated for will discuss many issues about dental to suppress your immune system, you transplant to check the health of your care and the best ways to take care of could have an increased risk of dental teeth and gums. This is important your teeth and gums. health problems. All of these factors because some medications that you can add to dental problems following take after transplant may cause you Why could I have transplant. to develop infections more easily. problems with my teeth Maintaining your dental health as best What are the most as you can while waiting for an organ and gums? will help you do better after your There are several reasons why you common dental transplant. -

Sensitive Teeth Sensitive Teeth Can Be Treated
FOR THE DENTAL PATIENT ... TREATMENT Sensitive teeth Sensitive teeth can be treated. Depending on the cause, your dentist may suggest that you try Causes and treatment desensitizing toothpaste, which contains com- pounds that help block sensation traveling from the tooth surface to the nerve. Desensitizing f a taste of ice cream or a sip of coffee is toothpaste usually requires several applications sometimes painful or if brushing or flossing before the sensitivity is reduced. When choosing makes you wince occasionally, you may toothpaste or any other dental care products, look have a common problem called “sensitive for those that display the American Dental Asso- teeth.” Some of the causes include tooth ciation’s Seal of Acceptance—your assurance that Idecay, a cracked tooth, worn tooth enamel, worn products have met ADA criteria for safety and fillings and tooth roots that are exposed as a effectiveness. result of aggressive tooth brushing, gum recession If the desensitizing toothpaste does not ease and periodontal (gum) disease. your discomfort, your dentist may suggest in- office treatments. A fluoride gel or special desen- SYMPTOMS OF SENSITIVE TEETH sitizing agents may be applied to the sensitive A layer of enamel, the strongest substance in the areas of the affected teeth. When these measures body, protects the crowns of healthy teeth. A layer do not correct the problem, your dentist may rec- called cementum protects the tooth root under the ommend other treatments, such as a filling, a gum line. Underneath the enamel and the crown, an inlay or bonding to correct a flaw or cementum is dentin, a part of the tooth that is decay that results in sensitivity. -

Tobacco and Your Oral Health
Oral Wellness Series Tobacco and Your Oral Health We all know smoking is bad for us, but did you know that chewing tobacco is just as harmful to your oral health as cigarettes? Tobacco causes bad breath, which nobody likes, but it has far more serious risks to your oral health, including: • Mouth sores • Slow healing after oral surgery • Difficulties correcting cosmetic dental problems • Stained teeth and tongue • Dulled sense of taste and smell The Biggest Risk? Did you know tobacco Cancer. The Centers for Disease Control have linked smoking and use is a huge risk factor tobacco use to oral cancer. Oral cancer is the eighth most common cancer in the U.S., and it’s very difficult to detect. As a result, two- for gum disease? thirds of all cases are diagnosed in late stages, making treatment and survival difficult.1 Tobacco and Gum Disease Tobacco use is also a huge risk factor for gum disease, a leading cause of tooth loss. More than 41% of daily smokers over the age of 65 are toothless because of gum disease, compared to only 20% of non-smokers.2 Maintain good oral health by avoiding tobacco. It keeps your whole body healthier. The Effects of Smoking on Your Gums Smoking reduces blood flow to your gums, cutting Is Smokeless Tobacco Safer? off vital nutrients and preventing bones from healing. Smokeless tobacco—chew, dip and snuff—is not This lets bacteria from tartar infect surrounding tissue, regulated by the FDA so it’s hard to know what’s in it. 3 forming deep pockets between teeth and gums. -

Sensitive Teeth May Be A
Sensitive Teeth May Be a Warning of More Serious bcbsfepdental.com Problems Sensitive teeth can be experienced at any age, with different levels of pain. When a sip of iced tea, a cup of hot cocoa, or the sudden intake of cold air or pressure from your toothbrush causes pain you may have a common problem called “sensitive teeth.” Sensitive teeth can be experienced at any age as a momentary slight twinge to long-term severe discomfort. It is important to consult with your dentist because sensitive teeth may be an early warning sign of more serious dental problems. Tooth Structure To better understand how sensitivity develops, we need to consider the composition of tooth structure. The crown — the part of the tooth that is most visible — has a tough, protective jacket of enamel, which is an extremely strong substance. Below the gum line, a layer of cementum Do I Need to See My Dentist? protects the tooth root. Underneath the enamel and If you have sensitive teeth, consult your cementum is dentin which contains tiny tubes. When dentin dentist to get a diagnostic evaluation. loses its protective covering (enamel or cementum) from This will determine the extent of the cracks or decay the small dentinal tubules become exposed problem and the treatment. Your permitting heat, cold, certain types of foods or pressure to dentist will evaluate your oral behavior stimulate nerves and cells inside of the tooth. This causes and recommend products that will best teeth to be sensitive producing occasional discomfort. serve you. Causes Dentists can provide mouthguards to minimize the impact of tooth grinding Sensitive teeth can be caused by cavities, fractures (cracked that is the result of clenching or tooth), worn tooth enamel, exposed tooth root, gum bruxing. -
Public Use Data File Documentation
Public Use Data File Documentation Part III - Medical Coding Manual and Short Index National Health Interview Survey, 1995 From the CENTERSFOR DISEASECONTROL AND PREVENTION/NationalCenter for Health Statistics U.S. DEPARTMENTOF HEALTHAND HUMAN SERVICES Centers for Disease Control and Prevention National Center for Health Statistics CDCCENTERS FOR DlSEASE CONTROL AND PREVENTlON Public Use Data File Documentation Part Ill - Medical Coding Manual and Short Index National Health Interview Survey, 1995 U.S. DEPARTMENT OF HEALTHAND HUMAN SERVICES Centers for Disease Control and Prevention National Center for Health Statistics Hyattsville, Maryland October 1997 TABLE OF CONTENTS Page SECTION I. INTRODUCTION AND ORIENTATION GUIDES A. Brief Description of the Health Interview Survey ............. .............. 1 B. Importance of the Medical Coding ...................... .............. 1 C. Codes Used (described briefly) ......................... .............. 2 D. Appendix III ...................................... .............. 2 E, The Short Index .................................... .............. 2 F. Abbreviations and References ......................... .............. 3 G. Training Preliminary to Coding ......................... .............. 4 SECTION II. CLASSES OF CHRONIC AND ACUTE CONDITIONS A. General Rules ................................................... 6 B. When to Assign “1” (Chronic) ........................................ 6 C. Selected Conditions Coded ” 1” Regardless of Onset ......................... 7 D. When to Assign -

Diagnosing Periodontitis
www.periodontal-health.com 1 Section 4 – Diagnosing periodontitis Contents • 4.1 Clinical examination 3 • 4.2 Basic periodontal examination 4 • 4.3 Periodontal chart 6 • 4.4 X-ray finding 8 • 4.5 Microbiological test 9 • 4.6 Classification of periodontal disease 10 www.periodontal-health.com 2 Section 4 – Diagnosing periodontitis Legal notice The website www.periodontal-health.com is an information platform ab- out the causes, consequences, diagnosis, treatment, and prevention of pe- riodontitis. The contents were created in media dissertations for a doctora- te at the University of Bern. Media dissertations under the supervision of PD Dr. Christoph A. Ramseier MAS Periodontology SSO, EFP Periodontology Clinic, Dental Clinics of the University of Bern Content created by Dr. Zoe Wojahn, MDM PD Dr. Christoph A. Ramseier, MAS Declaration of no-conflict-of-interest The production of this website and its hosting was and is being funded by the lead author. The translation of this website into the English language was funded by the European Federation of Periodontology (EFP). The pro- duction of the images was supported by the School of Dental Medicine of the University of Bern. Illustrations Bernadette Rawyler Scientific Illustrator Department of Multimedia, Dental Clinics of the University of Bern Correspondence address PD Dr. med. dent. Christoph A. Ramseier, MAS Dental Clinics of the University of Bern Periodontology Clinic Freiburgstrasse 7 CH-3010 Bern Tel. +41 31 632 25 89 E-Mail: [email protected] Creative Commons Lisence: Attribution-NonCommercial-ShareAlike 4.0 International (CC BY-NC-SA 4.0) https://creativecommons.org/licenses/by-nc-sa/4.0/deed.en www.periodontal-health.com 3 Section 4 – Diagnosing periodontitis 4.1 Clinical examination The clinical examination in the dental practice is the only way to properly assess the condition of the gums. -

Idiopathic Gingival Fibromatosis Associated with Generalized Aggressive Periodontitis: a Case Report
Clinical P RACTIC E Idiopathic Gingival Fibromatosis Associated with Generalized Aggressive Periodontitis: A Case Report Contact Author Rashi Chaturvedi, MDS, DNB Dr. Chaturvedi Email: rashichaturvedi@ yahoo.co.in ABSTRACT Idiopathic gingival fibromatosis, a benign, slow-growing proliferation of the gingival tissues, is genetically heterogeneous. This condition is usually part of a syndrome or, rarely, an isolated disorder. Aggressive periodontitis, another genetically transmitted disorder of the periodontium, typically results in severe, rapid destruction of the tooth- supporting apparatus. The increased susceptibility of the host population with aggressive periodontitis may be caused by the combined effects of multiple genes and their inter- action with various environmental factors. Functional abnormalities of neutrophils have also been implicated in the etiopathogenesis of aggressive periodontitis. We present a rare case of a nonsyndromic idiopathic gingival fibromatosis associated with general- ized aggressive periodontitis. We established the patient’s diagnosis through clinical and radiologic assessment, histopathologic findings and immunologic analysis of neutrophil function with a nitro-blue-tetrazolium reduction test. We describe an interdisciplinary approach to the treatment of the patient. For citation purposes, the electronic version is the definitive version of this article: www.cda-adc.ca/jcda/vol-75/issue-4/291.html diopathic gingival fibromatosis is a rare syndromic, have been genetically linked to hereditary condition -

Icd-9-Cm (2010)
ICD-9-CM (2010) PROCEDURE CODE LONG DESCRIPTION SHORT DESCRIPTION 0001 Therapeutic ultrasound of vessels of head and neck Ther ult head & neck ves 0002 Therapeutic ultrasound of heart Ther ultrasound of heart 0003 Therapeutic ultrasound of peripheral vascular vessels Ther ult peripheral ves 0009 Other therapeutic ultrasound Other therapeutic ultsnd 0010 Implantation of chemotherapeutic agent Implant chemothera agent 0011 Infusion of drotrecogin alfa (activated) Infus drotrecogin alfa 0012 Administration of inhaled nitric oxide Adm inhal nitric oxide 0013 Injection or infusion of nesiritide Inject/infus nesiritide 0014 Injection or infusion of oxazolidinone class of antibiotics Injection oxazolidinone 0015 High-dose infusion interleukin-2 [IL-2] High-dose infusion IL-2 0016 Pressurized treatment of venous bypass graft [conduit] with pharmaceutical substance Pressurized treat graft 0017 Infusion of vasopressor agent Infusion of vasopressor 0018 Infusion of immunosuppressive antibody therapy Infus immunosup antibody 0019 Disruption of blood brain barrier via infusion [BBBD] BBBD via infusion 0021 Intravascular imaging of extracranial cerebral vessels IVUS extracran cereb ves 0022 Intravascular imaging of intrathoracic vessels IVUS intrathoracic ves 0023 Intravascular imaging of peripheral vessels IVUS peripheral vessels 0024 Intravascular imaging of coronary vessels IVUS coronary vessels 0025 Intravascular imaging of renal vessels IVUS renal vessels 0028 Intravascular imaging, other specified vessel(s) Intravascul imaging NEC 0029 Intravascular -

Clinical Practice Guideline for Periodontics
Clinical Practice Guideline For Periodontics © MOH- Oral Health CSN –Periodontics-2010 Page 1 of 16 INTRODUCTION: Periodontal Diseases. This term, in its widest sense, includes all pathological conditions of the periodontium. It is however, commonly used with reference to those inflammatory disease which are plaque induced and which affect the marginal periodontium: Periodontitis and Gingivitis Gingivitis: Gingivitis is the mildest form of periodontal disease. It involves inflammation confined to the gingival tissues. • There is no loss of connective tissue attachment • A gingival pocket may be present Periodontitis: Is the apical extension of gingival inflammation to involve the supporting tissues. Destruction of the fibre attachment results in periodontal pockets. • it leads to loss of connective tissue attachment • which in turn results in loss of supporting alveolar bone © MOH- Oral Health CSN –Periodontics-2010 Page 2 of 16 OBJECTIVES OF TREATMENT • Relief of symptoms • Restoration of periodontal health • Restoration and maintenance of function and aesthetic PERIODONTAL ASSESSMENT Assessment of medical history Assessment of dental history Assessment of periodontal risk factors Assessment of extra-oral and intraoral structures and tissues 1. Age Assessment of teeth 2. Gender 3. Medications 1. Mobility 4. Presence of plaque and calculus (quantity and 2. Caries distribution) 3. Furcation involvement 5. Smoking 4. Position in dental arch and within alveolus 6. Race/Ethnicity 5. Occlusal relationships 7. Systemic disease (eg, diabetes) 6. Evidence of trauma from occlusion 8. Oral hygiene 9. Socio-economic status and level of education Assessment of periodontal soft tissues 1. Colour 2. Contour 3. Consistency (fibrotic or oedematous) 4. Presence of purulence (suppuration) 5.