Queen Charlotte/Haida Gwaii General Hospital
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Telkwa High Road Circle Tour
Telkwa High Road Circle Tour To Prince Rupert (314 km) A Bulkley Valley Museum WITSET D Driftwood Canyon Provincial Park G Spend some time learning about the (MORICETOWN) 10 kilometres north of Smithers human and ancient natural history Known locally as “the Fossil Beds”, Driftwood Canyon is of the Bulkley Valley. Entrance is by the site of the world’s earliest known salmonid fossil— donation. eosalmo driftwoodensis. Since the Bulkley River is one of the B world’s great steelhead rivers, it cannot be a coincidence that Aldermere Trails salmonids got their start in this valley. The fossils at Driftwood An easy trail walk to the site of the Canyon are up to 50 million years old and include plants, insects, Bulkley Valley’s earliest non-First fish, birds and rodents. The land that makes up the park was Nations settlement. donated by long-time Bulkley Valley resident Gordon Harvey. The fossil beds are under the management of BC Parks and C Tyhee Lake Provincial Park visitors are welcome to use this lovely day-use park. There Enjoy the sandy beach, wildlife are picnic tables beside Driftwood Creek. The trail to 17.2 km viewing platform and many amenities the fossil beds is wheelchair accessible. Enjoy the 25.7 km of the park, including playground, firepits, park and the interpretive material, but please do not covered picnic facilities and more. collect fossils. YELLOWHEAD E Babine Mountains Provincial Park Telkwa Access the alpine or stay in the valley — trails N abound in this incredible park. H Paved highway High F Paved road Mountainview Horseback Trail Riding Gravel road Circle route Book a scenic horseback trail ride for an hour or a BULKLEY day. -

Indian and Non-Native Use of the Bulkley River an Historical Perspective
Scientific Excellence • Resource Protection & Conservation • Benefits for Canadians DFO - Library i MPO - Bibliothèque ^''entffique • Protection et conservation des ressources • Bénéfices aux Canadiens I IIII III II IIIII II IIIIIIIIII II IIIIIIII 12020070 INDIAN AND NON-NATIVE USE OF THE BULKLEY RIVER AN HISTORICAL PERSPECTIVE by Brendan O'Donnell Native Affairs Division Issue I Policy and Program Planning Ir, E98. F4 ^ ;.;^. 035 ^ no.1 ;^^; D ^^.. c.1 Fisher és Pêches and Oceans et Océans Cariad'â. I I Scientific Excellence • Resource Protection & Conservation • Benefits for Canadians I Excellence scientifique • Protection et conservation des ressources • Bénéfices aux Canadiens I I INDIAN AND NON-NATIVE I USE OF THE BULKLEY RIVER I AN HISTORICAL PERSPECTIVE 1 by Brendan O'Donnell ^ Native Affairs Division Issue I 1 Policy and Program Planning 1 I I I I I E98.F4 035 no. I D c.1 I Fisheries Pêches 1 1*, and Oceans et Océans Canada` INTRODUCTION The following is one of a series of reports onthe historical uses of waterways in New Brunswick and British Columbia. These reports are narrative outlines of how Indian and non-native populations have used these -rivers, with emphasis on navigability, tidal influence, riparian interests, settlement patterns, commercial use and fishing rights. These historical reports were requested by the Interdepartmental Reserve Boundary Review Committee, a body comprising representatives from Indian Affairs and Northern Development [DIAND], Justice, Energy, Mines and Resources [EMR], and chaired by Fisheries and Oceans. The committee is tasked with establishing a government position on reserve boundaries that can assist in determining the area of application of Indian Band fishing by-laws. -

Crown Lands: a History of Survey Systems
CROWN LANDS A History of Survey Systems W. A. Taylor, B.C.L.S. 1975 Registries and Titles Department Ministry of Sustainable Resource Management Victoria British Columbia 5th Reprint, 2004 4th Reprint, 1997 3rd Reprint, 1992 2nd Reprint and Edit, 1990 1st Reprint, 1981 ii To those in the Provincial Archives who have willingly supplied information, To those others who, knowingly and unknowingly, have contributed useful data, and help, and To the curious and interested who wonder why things were done as they were. W. A. Taylor, B.C.L.S. 1975 iii - CONTENTS - Page 1 Evolution of Survey Systems in British Columbia 4 First System 1851 - Hudson's Bay Company Sections. 4 Second System 1858 - Sections and Ranges Vancouver Island. 9 Third System 1858 - Sections, Ranges, Blocks. 13 Fourth System - Variable Sized District Lots. 15 Fifth System 1873 - Townships in New Westminster District. 20 Sixth System - Provincial Townships. 24 Seventh System - Island Townships. 25 Eighth System - District Lot System. 28 Ninth System - Dominion Lands. 31 General Remarks 33 Footnotes - APPENDICES - 35 Appendix A - Diary of an early surveyor, 1859. 38 Appendix B - Scale of fees, 1860. 39 Appendix C - General Survey Instructions. 40 Appendix D - E. & N. Railway Company Survey Rules, 1923. 43 Appendix E - Posting - Crown Land Surveys. 44 Appendix F - Posting - Dominion Land Surveys. 45 Appendix G - Posting - Land Registry Act Surveys. 46 Appendix H - Posting - Mineral Act Surveys. 47 Appendix I - Official Map Acts. 49 Appendix J - Lineal and Square Measure. iv - LIST OF PLATES - Page 2 Events Affecting Early Survey Systems 5 Plate 1. Victoria District Official Map. -
Telkwa Caribou Population Status and Background Information Summary
! ! ! Telkwa Caribou Population Status and Background Information Summary ! ! ! ! June%12,%2014% ! ! ! ! ! ! Prepared!by:! ! Deborah!Cichowski! Caribou!Ecological!Consulting! Box!3652! Smithers,!B.C.! !V0J!2N0! ! ! ! ! ! Prepared!for:! ! BC!Ministry!of!Forests,!Lands!and!Natural!Resource!Operations! Bag!5000! Smithers,!B.C.,!! V0J!2N0! ! ! ! ! ! Acknowledgements ! I!would!like!to!thank!Mark!Williams!and!George!Schultze,!formerly!of!the! BC!Ministry!of!Forests,!Lands!and!Natural!Resource!Operations!(BC! MFLNRO),!for!providing!information!and!for!sharing!their!knowledge!and! perspectives!about!the!Telkwa!caribou!population.!!I!would!also!like!to! thank!Conrad!Thiessen!(BC!MFLNRO)!for!graciously!addressing!all!my! requests!for!information,!and!Conrad!Thiessen!and!Len!Vanderstar!(BC! MFLNRO)!for!sharing!their!knowledge!of!the!Telkwa!caribou!and!recovery! area.!!Conrad!Thiessen!and!Mark!Williams!reviewed!earlier!versions!of! the!report.!!Funding!was!provided!by!BC!Ministry!of!Forests,!Lands!and! Natural!Resource!Operations.! ! ! ! ! ! Telkwa'Caribou'Population'Status'and'Background'Information'Summary' ii' Table of Contents ! Acknowledgements!....................................................................................!ii! Table!of!Contents!.......................................................................................!iii! List!of!Figures!..............................................................................................!v! List!of!Tables!..............................................................................................!vi! -

Births by Facility 2015/16
Number of Births by Facility British Columbia Maternal Discharges from April 1, 2015 to March 31, 2016 Ü Number of births: Fort Nelson* <10 10 - 49 50 - 249 250 - 499 500 - 999 Fort St. John 1,000 - 1,499 Wrinch Dawson Creek 1,500 - 2,499 Memorial* & District Mills Chetwynd * ≥ 2,500 Memorial Bulkley Valley MacKenzie & 1,500-2,499 Stuart Lake Northern Prince Rupert District * Births at home with a Haida Gwaii* University Hospital Registered Healthcare Provider of Northern BC Kitimat McBride* St. John G.R. Baker Memorial Haida Gwaii Shuswap Lake General 100 Mile District Queen Victoria Lower Mainland Inset: Cariboo Memorial Port Golden & District McNeill Lions Gate Royal Invermere St. Paul's Cormorant Inland & District Port Hardy * Island* Lillooet Ridge Meadows Powell River Vernon VGH* Campbell River Sechelt Kootenay Elk Valley Burnaby Lake Squamish Kelowna St. Joseph's General BC Women's General Surrey Penticton Memorial West Coast East Kootenay Abbotsford Royal General Regional Richmond Columbian Regional Fraser Creston Valley Tofino Canyon * Peace Langley Nicola General* Boundary* Kootenay Boundary Arch Memorial Nanaimo Lady Minto / Chilliwack Valley * Regional Gulf Islands General Cowichan Saanich District Victoria 0 62.5 125 250 375 500 Peninsula* General Kilometers * Hospital does not offer planned obstetrical services. Source: BC Perinatal Data Registry. Data generated on March 24, 2017 (from data as of March 8, 2017). Number of Births by Facility British Columbia, April 1, 2015 - March 31, 2016 Facility Community Births 100 Mile -

Skeena Salmon Habitat Conference .2
SSKEENAKEENA SSALMONALMON HHABITATABITAT CCONFERENCEONFERENCE SEPTEMBER 15-16 SMITHERS, B.C. SPEAKERSPEAKER ABSTRACTSABSTRACTS SPEAKERS: 1 BRIAN RIDDELL, CONFERENCE CHAIR BRIAN FUHR, BULKLEY VALLEY RESEARCH CENTRE 2 WELCOMING REMARKS: ROY MORRIS, WET’SUWET’EN HEREDITARY CHIEF CRESS FARROW, TOWN OF SMITHERS MAYOR SHELLEY BROWN, REPRESENTING SKEENA-BULKLEY VALLEY MP NATHAN CULLEN SHELLY WORTHINGTON, REPRESENTING STIKINE MLA DOUG DONALDSON 3 HONOURABLE JOHN FRASER, B.C. PACIFIC SALMON FORUM CHAIR ON IORDAN ACIFIC ALMON ORUM ESEARCH IRECTOR JON O’RIORDAN, PACIFIC SALMON FORUM RESEARCH DIRECTOR 4 GEOFF RECKNELL, INTEGRATED LAND MANAGEMENT BUREAU 5 MARK SAUNDERS, FISHERIES AND OCEANS CANADA 6 MEL KOTYK, FISHERIES AND OCEANS CANADA 7 GLEN WILLIAMS, GITANYOW FIRST NATION HEREDITARY CHIEF JANE LLOYD-SMITH, MINISTRY OF FORESTS BOBBY LOVE, MINISTRY OF FORESTS AND ILMB 8 WALTER JOSEPH, OFFICE OF THE WET’SUWET’EN IAN SHARPE, MINISTRY OF ENVIRONMENT SHAUNA BENNETT, BIO LOGIC CONSULTING 9 JODY HOLMES, RAIN FOREST SOLUTIONS 10 EVENING PROGRAM: ALI HOWARD & BRIAN HUNTINGTON, SPIRIT OF THE SKEENA SWIM 11 SANDRA SULYMA, MINISTRY OF ENVIRONMENT 12 DAVE DAUST 13 MICHAEL WEBSTER, GORDON AND BETTY MOORE FOUNDATION 14 JOHN REYNOLDS, SIMON FRASER UNIVERSITY 15 KERRI BROWNIE, MINISTRY OF FORESTS 16 JACK STANFORD, UNIVERSITY OF MONTANA 17 JEFFREY ANDERSON, GEOMORPHIC EARTH & ENVIRONMENTAL .1. CONFERENCE CHAIR: BRIAN RIDDELL Conference Objectives Brian Riddell is president and CEO of the Pacific Salmon Foundation. He has a PhD from McGill University and is former Division Head, Salmon and Freshwater Ecosystems, Science Branch, Department of Fisheries and Oceans, Pacific Biological Station based in Nanaimo, BC. Brian is one of Canada’s most respected and decorated salmon researchers and managers. -

Regional District of Bulkley-Nechako)
Agricultural Land Use Planning in Northern British Columbia Case Study of Smithers Telkwa Rural Area (Regional District of Bulkley-Nechako) FINAL REPORT Dr. David J. Connell Associate Professor University of Northern British Columbia May, 2015 Agricultural Land Use Planning in Northern British Columbia FINAL REPORT: SMITHERS TELKWA RURAL AREA CASE STUDY Executive Summary In this report we present the results of a case study of agricultural land use planning in the Smithers Telkwa Rural Area (STRA), the rural area that surrounds the Town of Smithers and the Village of Telkwa in British Columbia. The STRA is part of Electoral Area A in the Regional District of Bulkley-Nechako (RDBN). The study involved an assessment of the breadth and quality of the local legislative framework that governs agricultural land use planning, including policies, legislation, and governance. We assessed the strength of the local framework for agricultural land use planning using four principles as criteria: maximise stability, integrate public priorities across jurisdictions, minimise uncertainty, and accommodate flexibility. The study also involved an assessment of the political context within which agricultural land use planning takes place and decisions are made. This part of the assessment included documentation and analysis of three policy regimes: farmland preservation, global competitiveness, and food sovereignty. A policy regime refers to the combination of issues, ideas, interests, actors, and institutions that are involved in formulating policy and for governing once policies are devised. The aim of the case study is to contribute to three areas of knowledge. The case study lends insight to the state of agricultural land use planning in the RDBN. -

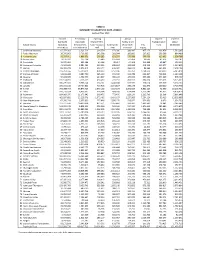
Table 28 2017/18 Total Actual Revenues (Operating, Special Purpose and Capital Funds)
TABLE 28 2017/18 TOTAL ACTUAL REVENUES (OPERATING, SPECIAL PURPOSE AND CAPITAL FUNDS) PROVINCIAL GRANTS PROVINCIAL GRANTS PROVINCIAL GRANTS PROVINCIAL GRANTS PROVINCIAL GRANTS PROVINCIAL GRANTS MUNICIPAL GRANTS MINISTRY OF EDUCATION % OF MINISTRY OF EDUCATION % OF MINISTRY OF EDUCATION % OF OTHER % OF OTHER % OF OTHER % OF SPENT ON SITES % OF (Operating) TOTAL (Special Purpose) TOTAL (Capital) TOTAL (Operating) TOTAL (Special Purpose) TOTAL (Capital) TOTAL (Capital) TOTAL 5 Southeast Kootenay 56,769,318 84.2% 3,878,512 5.8% - - - - 109,421 0.2% - - - - 6 Rocky Mountain 35,150,899 75.6% 3,685,965 7.9% 1,981 0.0% 35,240 0.1% 15,359 0.0% - - - - 8 Kootenay Lake 51,585,200 78.4% 5,918,360 9.0% - - 246,709 0.4% - - - - - - 10 Arrow Lakes 7,047,608 84.4% 558,881 6.7% - - 18,000 0.2% - - - - - - 19 Revelstoke 10,884,708 74.1% 866,931 5.9% - - 61,070 0.4% - - - - - - 20 Kootenay-Columbia 38,131,484 82.5% 3,644,899 7.9% - - 237,430 0.5% - - - - - - 22 Vernon 77,650,399 78.1% 8,314,425 8.4% - - 270,110 0.3% 11,000 0.0% - - - - 23 Central Okanagan 198,814,251 80.4% 16,662,719 6.7% 27,241 0.0% 695,250 0.3% - - - - - - 27 Cariboo-Chilcotin 50,698,481 81.7% 4,726,794 7.6% - - 20,000 0.0% 168,909 0.3% - - - - 28 Quesnel 33,525,372 85.7% 3,195,700 8.2% - - 34,900 0.1% 26,355 0.1% - - - - 33 Chilliwack 124,122,438 79.8% 9,709,195 6.2% 4,280,318 2.8% 179,513 0.1% 14,426 0.0% 89,986 0.1% 1,697,626 1.1% 34 Abbotsford 172,163,240 81.2% 13,571,340 6.4% 2,887,308 1.4% 273,182 0.1% 50,078 0.0% - - - - 35 Langley 178,863,512 74.3% 18,719,104 7.8% 7,580,000 3.2% -

Alberni Valley Track & Field Club Bulkley Valley Athletic Society
BC Athletics 2016 JD Crest Winners September 14, 2016 Alberni Valley Track & Field Club (sorted by Club) Broekhuizen, Jordyn BRONZE Hall, Isabella SILVER Hall, Victoria BRONZE Hunt, Emily SILVER Mckean, Jackson SILVER Mcleod, Ally BRONZE Orchard, Linden BRONZE Savard, Clare BRONZE Souther, Peter BRONZE Symington, David SILVER Symington, Gavin SILVER Wynans, Dominic SILVER Wynans, Samuel SILVER Bulkley Valley Athletic Society Press, Sean BRONZE Burnaby Striders Track & Field Club Cummings, Jaeland GOLD Iwan, Niklas SILVER Kanyamuna, Kelsey GOLD Lopez, Mateo SILVER Mirisklavos, Alexander SILVER Primeau, Luc GOLD Roche, Michelle BRONZE Vandermey, Joshua SILVER Campbell River Comets Berkey, Rowen BRONZE Berkey, Shea GOLD Brennan, Menoa SILVER Chatterton, Anna BRONZE Chatterton, Gavin SILVER Danielson, Kiana BRONZE Dirom, Luke GOLD Grafton, Jessica SILVER Idiens, Joel BRONZE Konkle-Skuse, Ryley GOLD Milne, Emily GOLD Milne, Lucas BRONZE Perras, Trent SILVER Revoy, Kate-Lynn BRONZE Simmons, Lacie GOLD Skuse, Tyza SILVER Underhill, Abigayle SILVER Chilliwack Track & Field Club Cote, Larissa GOLD Fuller, Kailea SILVER BC Athletics 2016 JD Crest Winners September 14, 2016 Goodnough, Nathan SILVER (sorted by Club) Klaus, Chanine GOLD Klaus, Juane SILVER Lenz, Brandt GOLD Lenz, Malia GOLD Markey, Clara GOLD Meachin, Simon BRONZE Roche, Sophie BRONZE Smith, Theo BRONZE Unruh, Macy SILVER Coastal Track Club Forsyth, Isabelle GOLD Ogbeiwi, Michael GOLD Comox Valley Cougars Bakshi, Ankit SILVER Bakshi, Avik BRONZE Burch, Patti BRONZE Horel (Biggs), Kailey -

Town of Smithers
TOWN OF SMITHERS Minutes of the Regular Meeting of Council held in Council Chambers, 3836 Fourth Avenue, Smithers, B.C., on Tuesday, January 13, 2004, at 7:30 p.m. Council Present: Staff Present: Jim Davidson, Mayor Wallace Mah, Corporate Administrator/CAO Norm Adomeit, Councillor Jason Llewellyn, Deputy Chief Administrative Cathryn Bucher, Councillor Officer Cress Farrow, Councillor James Warren, Corporate Administrative Assistant Bill Goodacre, Councillor Leslie Ford, Financial Administrator/Collector Andy Howard, Councillor Mark Allen, Director of Development Services Marilyn Stewart, Councillor. Darcey Kohuch, Director of Operational Services Keith Stecko, Airport Manager/Deputy Fire Chief Penny Goodacre, Recording Secretary. Staff Excused: Les Schumacher, Fire Chief. Media Present: C. Lester, BVLD, and M. Pearson, The Interior News. Public Present: J. Stewart, K. Gurry, D. MacKay, E. MacKay, B. Elsner, I. Meier, T. Barbuto and C. Northrup. CALL TO ORDER 1. Mayor Davidson called the meeting to order (7:30 p.m.). PUBLIC HEARING 2. None. APPROVAL OF MINUTES 3-1 Adomeit/Farrow 04.0001 THAT the minutes of the Regular Meeting of Council held December 9, 2003, REG DEC 9 be adopted. CARRIED UNANIMOUSLY. 3-2 Farrow/Bucher 04.0002 THAT the minutes of the Committee of the Whole meeting held December 16, C.O.W. 2003, be adopted and the cost of mailing the survey be financed from Council DEC 16 Contingency. CARRIED UNANIMOUSLY. 3-3 Howard/Adomeit 04.0003 THAT the minutes of the Committee of the Whole meeting held January 6, C.O.W. 2004, be adopted. JAN 6 CARRIED UNANIMOUSLY. BUSINESS ARISING FROM THE MINUTES 4-1 Report ADM 03-102 dated December 16, 2003, from W. -
2020-2021 Summary of Grants
TABLE A SUMMARY OF GRANTS TO DATE, 2020/21 Updated May 2020 2020/21 Preliminary Learning Annual Student Teachers' Estimated Classroom Improvement Facility Grant Transportation Labour School District Operating Enhancement Fund - Support Community- (Total Oper. Pay Fund Settlement Grant Block Fund Allocation Staff LINK Portion)* Equity 5 Southeast Kootenay 65,373,362 2,521,513 236,579 373,586 286,997 457,171 361,459 1,510,285 6 Rocky Mountain 39,375,063 2,711,005 142,508 391,904 195,806 207,823 369,399 884,489 8 Kootenay Lake 55,337,051 4,866,976 200,282 631,599 279,588 300,996 419,602 1,338,788 10 Arrow Lakes 8,135,932 197,784 29,448 105,604 62,454 40,560 42,675 160,142 19 Revelstoke 11,976,283 496,384 43,344 98,017 65,368 101,498 49,847 314,296 20 Kootenay-Columbia 41,322,622 2,884,464 149,552 688,964 193,868 248,239 242,977 1,042,845 22 Vernon 85,495,328 5,573,017 309,422 645,902 356,510 85,865 361,094 2,328,158 23 Central Okanagan 223,351,556 15,510,011 808,330 1,252,296 785,351 1,238,323 600,000 6,145,818 27 Cariboo-Chilcotin 53,913,488 3,487,700 195,123 676,140 311,749 665,837 739,024 1,243,194 28 Quesnel 34,263,909 1,732,479 124,007 489,126 179,096 379,632 274,209 878,407 33 Chilliwack 135,514,037 7,116,729 490,428 722,132 456,531 864,624 329,456 3,575,689 34 Abbotsford 186,276,925 9,998,124 674,161 1,240,748 691,973 118,014 313,969 5,074,150 35 Langley 195,606,160 19,757,851 707,918 2,071,827 680,178 551,875 260,000 5,739,774 36 Surrey 703,788,757 36,877,425 2,547,102 4,017,294 2,362,029 6,861,224 72,999 19,190,731 37 Delta 147,713,554 -

A Four-Year Picture
September 2005 Health Authority Redesign Accomplishments A Four-Year Picture Northern Health NORTHERN HEALTH Health Service Redesign British Columbia is planning a health care system where high quality health care is available to everyone – where services are timely, affordable and sustainable, for today and future generations. Since 2002, when government streamlined 52 health regions with competing or overlapping mandates into six health authorities, the province has been able to maximize the resources available for direct patient care. Five regional health authorities now have responsibility for planning and delivering local health services, such as public health, mental health, residential, home and hospital care. The Provincial Health Services Authority oversees provincial and highly-specialized health services, such as the BC Cancer Agency. A strong economy and sound fiscal management have enabled the province to increase health care spending by $3.8 billion between 2001 and 2007. Strategic investments, based on best practices and innovative approaches to local challenges, are improving health authorities’ ability to respond to patients’ needs. As British Columbia moves forward into the 21st century, lifestyle choices – in nutrition, physical activity, non-smoking and responsible use of alcohol – will be the foundation of keeping our population healthy and our health care system sustainable. Northern Health Northern Health provides a full range of health care services to approximately 297,0001 residents in northern British Columbia. It covers almost two-thirds of B.C., bordered by the Northwest and Yukon Territories, the B.C. interior, Alberta, Alaska and the Pacific Ocean. Northern Health employs 7,000 staff. Acute Care Services Health authorities and the Provincial Health Services Authority are designing a network of acute care that includes centres of excellence for specialized services and community hospitals or treatment centres for basic emergency services.