Agraphia and Acalculia After a Left Prefrontal (F1, F2) Infarction
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Man'yogana.Pdf (574.0Kb)
Bulletin of the School of Oriental and African Studies http://journals.cambridge.org/BSO Additional services for Bulletin of the School of Oriental and African Studies: Email alerts: Click here Subscriptions: Click here Commercial reprints: Click here Terms of use : Click here The origin of man'yogana John R. BENTLEY Bulletin of the School of Oriental and African Studies / Volume 64 / Issue 01 / February 2001, pp 59 73 DOI: 10.1017/S0041977X01000040, Published online: 18 April 2001 Link to this article: http://journals.cambridge.org/abstract_S0041977X01000040 How to cite this article: John R. BENTLEY (2001). The origin of man'yogana. Bulletin of the School of Oriental and African Studies, 64, pp 5973 doi:10.1017/S0041977X01000040 Request Permissions : Click here Downloaded from http://journals.cambridge.org/BSO, IP address: 131.156.159.213 on 05 Mar 2013 The origin of man'yo:gana1 . Northern Illinois University 1. Introduction2 The origin of man'yo:gana, the phonetic writing system used by the Japanese who originally had no script, is shrouded in mystery and myth. There is even a tradition that prior to the importation of Chinese script, the Japanese had a native script of their own, known as jindai moji ( , age of the gods script). Christopher Seeley (1991: 3) suggests that by the late thirteenth century, Shoku nihongi, a compilation of various earlier commentaries on Nihon shoki (Japan's first official historical record, 720 ..), circulated the idea that Yamato3 had written script from the age of the gods, a mythical period when the deity Susanoo was believed by the Japanese court to have composed Japan's first poem, and the Sun goddess declared her son would rule the land below. -

SUPPORTING the CHINESE, JAPANESE, and KOREAN LANGUAGES in the OPENVMS OPERATING SYSTEM by Michael M. T. Yau ABSTRACT the Asian L
SUPPORTING THE CHINESE, JAPANESE, AND KOREAN LANGUAGES IN THE OPENVMS OPERATING SYSTEM By Michael M. T. Yau ABSTRACT The Asian language versions of the OpenVMS operating system allow Asian-speaking users to interact with the OpenVMS system in their native languages and provide a platform for developing Asian applications. Since the OpenVMS variants must be able to handle multibyte character sets, the requirements for the internal representation, input, and output differ considerably from those for the standard English version. A review of the Japanese, Chinese, and Korean writing systems and character set standards provides the context for a discussion of the features of the Asian OpenVMS variants. The localization approach adopted in developing these Asian variants was shaped by business and engineering constraints; issues related to this approach are presented. INTRODUCTION The OpenVMS operating system was designed in an era when English was the only language supported in computer systems. The Digital Command Language (DCL) commands and utilities, system help and message texts, run-time libraries and system services, and names of system objects such as file names and user names all assume English text encoded in the 7-bit American Standard Code for Information Interchange (ASCII) character set. As Digital's business began to expand into markets where common end users are non-English speaking, the requirement for the OpenVMS system to support languages other than English became inevitable. In contrast to the migration to support single-byte, 8-bit European characters, OpenVMS localization efforts to support the Asian languages, namely Japanese, Chinese, and Korean, must deal with a more complex issue, i.e., the handling of multibyte character sets. -
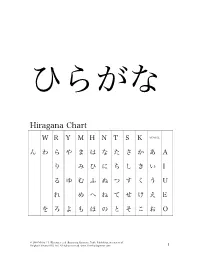
Hiragana Chart
ひらがな Hiragana Chart W R Y M H N T S K VOWEL ん わ ら や ま は な た さ か あ A り み ひ に ち し き い I る ゆ む ふ ぬ つ す く う U れ め へ ね て せ け え E を ろ よ も ほ の と そ こ お O © 2010 Michael L. Kluemper et al. Beginning Japanese, Tuttle Publishing, an imprint of Periplus Editions (HK) Ltd. All rights reserved. www.TimeForJapanese.com. 1 Beginning Japanese 名前: ________________________ 1-1 Hiragana Activity Book 日付: ___月 ___日 一、 Practice: あいうえお かきくけこ がぎぐげご O E U I A お え う い あ あ お え う い あ お う あ え い あ お え う い お う い あ お え あ KO KE KU KI KA こ け く き か か こ け く き か こ け く く き か か こ き き か こ こ け か け く く き き こ け か © 2010 Michael L. Kluemper et al. Beginning Japanese, Tuttle Publishing, an imprint of Periplus Editions (HK) Ltd. All rights reserved. www.TimeForJapanese.com. 2 GO GE GU GI GA ご げ ぐ ぎ が が ご げ ぐ ぎ が ご ご げ ぐ ぐ ぎ ぎ が が ご げ ぎ が ご ご げ が げ ぐ ぐ ぎ ぎ ご げ が 二、 Fill in each blank with the correct HIRAGANA. SE N SE I KI A RA NA MA E 1. -

Systems Neuroscience of Mathematical Cognition and Learning
CHAPTER 15 Systems Neuroscience of Mathematical Cognition and Learning: Basic Organization and Neural Sources of Heterogeneity in Typical and Atypical Development Teresa Iuculano, Aarthi Padmanabhan, Vinod Menon Stanford University, Stanford, CA, United States OUTLINE Introduction 288 Ventral and Dorsal Visual Streams: Neural Building Blocks of Mathematical Cognition 292 Basic Organization 292 Heterogeneity in Typical and Atypical Development 295 Parietal-Frontal Systems: Short-Term and Working Memory 296 Basic Organization 296 Heterogeneity in Typical and Atypical Development 299 Lateral Frontotemporal Cortices: Language-Mediated Systems 302 Basic Organization 302 Heterogeneity in Typical and Atypical Development 302 Heterogeneity of Function in Numerical Cognition 287 https://doi.org/10.1016/B978-0-12-811529-9.00015-7 © 2018 Elsevier Inc. All rights reserved. 288 15. SYSTEMS NEUROSCIENCE OF MATHEMATICAL COGNITION AND LEARNING The Medial Temporal Lobe: Declarative Memory 306 Basic Organization 306 Heterogeneity in Typical and Atypical Development 306 The Circuit View: Attention and Control Processes and Dynamic Circuits Orchestrating Mathematical Learning 310 Basic Organization 310 Heterogeneity in Typical and Atypical Development 312 Plasticity in Multiple Brain Systems: Relation to Learning 314 Basic Organization 314 Heterogeneity in Typical and Atypical Development 315 Conclusions and Future Directions 320 References 324 INTRODUCTION Mathematical skill acquisition is hierarchical in nature, and each iteration of increased proficiency builds on knowledge of a lower-level primitive. For example, learning to solve arithmetical operations such as “3 + 4” requires first an understanding of what numbers mean and rep- resent (e.g., the symbol “3” refers to the quantity of three items, which derives from the ability to attend to discrete items in the environment). -

Na Kana Magiti Kei Na Lotu
1 NA KANA MAGITI KEI NA LOTU (Vola Tabu : Maciu 22:1-10; Luke 14:12-24) Vola ko Rev. Dr. Ilaitia S. Tuwere. Sa inaki ni vunau oqo me taroga ka sauma talega na taro : A cava na Lotu? Ni da tekivu edaidai ena noda solevu vakalotu, sa na yaga meda taroga ka tovolea talega me sauma na taro oqori. Ia, ena levu na kena isau eda na solia, me vaka na: gumatuataki ni masu kei na vulici ni Vola Tabu, bula vakayalo, muria na ivakarau se lawa ni lotu ka vuqa tale. Na veika oqori era ka dina ka tu kina eso na isau ni taro : A Cava na Lotu. Na i Vola Tabu e sega ni tuvalaka vakavosa vei keda na ibalebale ni lotu. E vakavuqa me boroya vei keda na iyaloyalo me vakadewataka kina na veika eso e vinakata me tukuna. E sega talega ni solia e duabulu ga na iyaloyalo me baleta na lotu. E vuqa sara e solia vei keda. Oqori me vaka na Qele ni Sipi kei na i Vakatawa Vinaka; na Vuni Vaini kei na Tabana; na i Vakavuvuli kei iratou na nona Gonevuli se Tisaipeli, na Masima se Rarama kei Vuravura, na Ulu kei na Vo ni Yago taucoko, ka vuqa tale. Ena mataka edaidai, meda raica vata yani na iyaloyalo ni kana magiti. E rua na kena ivakamacala eda rogoca, mai na Kosipeli i Maciu kei na nei Luke. Na kana magiti se na solevu edua na ivakarau vakaitaukei. Eda soqoni vata kina vakaveiwekani ena noda veikidavaki kei na marau, kena veitalanoa, kena sere kei na meke, kena salusalu kei na kumuni iyau. -

Writing As Aesthetic in Modern and Contemporary Japanese-Language Literature
At the Intersection of Script and Literature: Writing as Aesthetic in Modern and Contemporary Japanese-language Literature Christopher J Lowy A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy University of Washington 2021 Reading Committee: Edward Mack, Chair Davinder Bhowmik Zev Handel Jeffrey Todd Knight Program Authorized to Offer Degree: Asian Languages and Literature ©Copyright 2021 Christopher J Lowy University of Washington Abstract At the Intersection of Script and Literature: Writing as Aesthetic in Modern and Contemporary Japanese-language Literature Christopher J Lowy Chair of the Supervisory Committee: Edward Mack Department of Asian Languages and Literature This dissertation examines the dynamic relationship between written language and literary fiction in modern and contemporary Japanese-language literature. I analyze how script and narration come together to function as a site of expression, and how they connect to questions of visuality, textuality, and materiality. Informed by work from the field of textual humanities, my project brings together new philological approaches to visual aspects of text in literature written in the Japanese script. Because research in English on the visual textuality of Japanese-language literature is scant, my work serves as a fundamental first-step in creating a new area of critical interest by establishing key terms and a general theoretical framework from which to approach the topic. Chapter One establishes the scope of my project and the vocabulary necessary for an analysis of script relative to narrative content; Chapter Two looks at one author’s relationship with written language; and Chapters Three and Four apply the concepts explored in Chapter One to a variety of modern and contemporary literary texts where script plays a central role. -

D Igital Text
Digital text The joys of character sets Contents Storing text ¡ General problems ¡ Legacy character encodings ¡ Unicode ¡ Markup languages Using text ¡ Processing and display ¡ Programming languages A little bit about writing systems Overview Latin Cyrillic Devanagari − − − − − − Tibetan \ / / Gujarati | \ / − Armenian / Bengali SOGDIAN − Mongolian \ / / Gurumukhi SCRIPT Greek − Georgian / Oriya Chinese | / / | / Telugu / PHOENICIAN BRAHMI − − Kannada SINITIC − Japanese SCRIPT \ SCRIPT Malayalam SCRIPT \ / | \ \ Tamil \ Hebrew | Arabic \ Korean | \ \ − − Sinhala | \ \ | \ \ _ _ Burmese | \ \ Khmer | \ \ Ethiopic Thaana \ _ _ Thai Lao The easy ones Latin is the alphabet and writing system used in the West and some other places Greek and Cyrillic (Russian) are very similar, they just use different characters Armenian and Georgian are also relatively similar More difficult Hebrew is written from right−to−left, but numbers go left−to−right... Arabic has the same rules, but also requires variant selection depending on context and ligature forming The far east Chinese uses two ’alphabets’: hanzi ideographs and zhuyin syllables Japanese mixes four alphabets: kanji ideographs, katakana and hiragana syllables and romaji (latin) letters and numbers Korean uses hangul ideographs, combined from jamo components Vietnamese uses latin letters... The Indic languages Based on syllabic alphabets Require complex ligature forming Letters are not written in logical order, but require a strange ’circular’ ordering In addition, a single line consists of separate -

Cognitive Performance Deficits and Dysgraphia in Alzheimer's Disease
Send Orders for Reprints to [email protected] 6 Open Medicine Journal, 2015, 2, 6-16 Open Access Cognitive Performance Deficits and Dysgraphia in Alzheimer’s Disease Patients Emanuela Onofri1, Marco Mercuri1, MariaLucia Salesi1, Max Rapp Ricciardi2 and Trevor Archer*,2 1Department of Anatomy, Histology, Legal Medicine and Orthopaedics, Sapienza University of Rome, Italy 2Department of Psychology, University of Gothenburg, Gothenburg, Sweden Abstract: Introduction: Agraphia or dysgraphia, observed often in early AD, encompasses a progressive disorganization and degeneration of the various components of handwriting. Methods: Deficits in writing ability, dysgraphia, and the relationship with other measures of cognitive decline were studied in a group of 30 patients, originating from the Lazio region, Rome, Italy, presenting a moderate to relatively severe stage of Alzheimer’s disease (AD). Extent of dysgraphia and cognitive performance was compared with a matched group of healthy controls selected from the same region. Results: Several markedly strong relationships between dysgraphia and several measures of cognitive performance in AD patients were observed concomitant with consistent deficits by this patient sample in comparison with the matched group of healthy control subjects were obtained. Additionally, several measures of loss of functional integrity, MMSE, ADL and IADL, were found to be associated with both dysgraphia and impairments in cognitive performance. Conclusion: The present results are discussed from the notion of -

Characteristics of Developmental Dyslexia in Japanese Kana: From
al Ab gic no lo rm o a h l i c t y i e s s Ogawa et al., J Psychol Abnorm Child 2014, 3:3 P i Journal of Psychological Abnormalities n f o C l DOI: 10.4172/2329-9525.1000126 h a i n l d ISSN:r 2329-9525 r u e o n J in Children Research Article Open Access Characteristics of Developmental Dyslexia in Japanese Kana: from the Viewpoint of the Japanese Feature Shino Ogawa1*, Miwa Fukushima-Murata2, Namiko Kubo-Kawai3, Tomoko Asai4, Hiroko Taniai5 and Nobuo Masataka6 1Graduate School of Medicine, Kyoto University, Kyoto, Japan 2Research Center for Advanced Science and Technology, the University of Tokyo, Tokyo, Japan 3Faculty of Psychology, Aichi Shukutoku University, Aichi, Japan 4Nagoya City Child Welfare Center, Aichi, Japan 5Department of Pediatrics, Nagoya Central Care Center for Disabled Children, Aichi, Japan 6Section of Cognition and Learning, Primate Research Institute, Kyoto University, Aichi, Japan Abstract This study identified the individual differences in the effects of Japanese Dyslexia. The participants consisted of 12 Japanese children who had difficulties in reading and writing Japanese and were suspected of having developmental disorders. A test battery was created on the basis of the characteristics of the Japanese language to examine Kana’s orthography-to-phonology mapping and target four cognitive skills: analysis of phonological structure, letter-to-sound conversion, visual information processing, and eye–hand coordination. An examination of the individual ability levels for these four elements revealed that reading and writing difficulties are not caused by a single disability, but by a combination of factors. -

Alexia Without Agraphia
Neuroradiology(1992) 34:210-214 Neuro radiology Springer-Verlag 1992 Alexia without agraphia D. J. Quint I and J. L. Gilmore 2 1Division of Neuroradiology,Department of Radiology,University of MichiganHospitals, Ann Arbor, Michigan,USA 2Department of Neurology,University of Rochester, Rochester, New York, USA Received: September 16, 1991 Summary. Two new cases of alexia without agraphia are mentation and right visual complaints. She had suffered presented. Pertinent clinical findings, anatomy, pathophy- from extensive atherosclerotic peripheralvascular disease siology and differential diagnoses are reviewed. The im- involving both the systemic and cerebral vasculature, portance of carefully examining the inferior portion of the necessitating carotid endarterectomy. The patient denied left side of the splenium of the corpus callosum on CT any "strokes", but did suffer from complications of scle- and/or MR scans in patients who present with this clinical roderma including gastritis, esophagitis and Raynaud's syndrome is stressed. phenomenon and had also had a cervical sympathectomy. The patient did report a vague episode of "loss of con- Key words: Alexia - Agraphia - Disconnection syndrome sciousness" 4-5 months before admission. - Magnetic resonance imaging - Computed tomography General physical examination showed some edema of the legs. Neurologic examination revealed the patient to be oriented to person and place, but not to time. She could Alexia without agraphia or pure word blindness is con- sidered one of the classic disconnection syndromes. Pa- identify letters, but could not read. She could write her name and spell simple words forwards and backwards. Cra- tients retain the ability to write, but are unable to read nial nerve (II-XII) examination demonstrated a right ho- (even words that they have just written) and often have monymous hemianopia. -

Children with Dyscalculia Show Hippocampal Hyperactivity During Symbolic Number Perception
fnhum-15-687476 July 14, 2021 Time: 18:40 # 1 ORIGINAL RESEARCH published: 20 July 2021 doi: 10.3389/fnhum.2021.687476 Children With Dyscalculia Show Hippocampal Hyperactivity During Symbolic Number Perception Sertaç Üstün1,2,3, Nazife Ayyıldız2,3,4, Emre H. Kale4, Öykü Mançe Çalı ¸sır4,5, Pınar Uran6, Özgür Öner7, Sinan Olkun8 and Metehan Çiçek1,2,3,4* 1 Department of Physiology, Ankara University School of Medicine, Ankara, Turkey, 2 Neuroscience and Neurotechnology Center of Excellence, Ankara, Turkey, 3 Department of Interdisciplinary Neuroscience, Health Science Institute, Ankara University, Ankara, Turkey, 4 Brain Research Center, Ankara University, Ankara, Turkey, 5 Program of Counseling and Guidance, Department of Educational Sciences, Ankara University Faculty of Educational Sciences, Ankara, Turkey, 6 Department of Child and Adolescent Psychiatry, Ankara University School of Medicine, Ankara, Turkey, 7 Department of Child and Adolescent Psychiatry, Bahçe ¸sehirUniversity School of Medicine, Istanbul,˙ Turkey, 8 Department of Mathematics Education, Final International University, Kyrenia, Cyprus Dyscalculia is a learning disability affecting the acquisition of arithmetical skills in children Edited by: Jonas Kaplan, with normal intelligence and age-appropriate education. Two hypotheses attempt to University of Southern California, explain the main cause of dyscalculia. The first hypothesis suggests that a problem United States with the core mechanisms of perceiving (non-symbolic) quantities is the cause of Reviewed by: dyscalculia (core deficit hypothesis), while the alternative hypothesis suggests that Hüseyin Akan, Ondokuz Mayıs University, Turkey dyscalculics have problems only with the processing of numerical symbols (access Roberto A. Abreu-Mendoza, deficit hypothesis). In the present study, the symbolic and non-symbolic numerosity Rutgers University–Newark, United States processing of typically developing children and children with dyscalculia were examined *Correspondence: with functional magnetic resonance imaging (fMRI). -

Frank's Do-It-Yourself Kana Cards V
Frank's do-it-yourself kana cards v. 1.0, 2000-08-07 Frank Stajano University of Cambridge and AT&T Laboratories Cambridge http://www.cl.cam.ac.uk/~fms27/ and http://www.uk.research.att.com/~fms/ This set of flash cards is meant to help you familiar cards and insist on the difficult part of き and さ with a separate stroke, become fluent in the use of the Japanese ones. unlike what happens in the fonts used in hiragana and katakana syllabaries. I made this document. I have followed the stroke it because I needed one myself and could The complete set consists of 10 double- counts of Henshall-Takagaki, even when not find it in the local bookshops (kanji sided sheets (20 printable pages) of 50 they seem weird for the shape of the char- cards were available, and I bought those; cards each, but you may choose to print acter as drawn on the card. but kana cards weren't); if it helps you too, smaller subsets as detailed below. Actu- so much the better. ally there are some blanks, so the total The easiest way to turn this document into number of cards is only 428 instead of 500. a set of cards is simply to print it (double The romanisation system chosen for these It would have been possible to fit them on sided of course!) and then cut each page cards is the Hepburn, which is the most 9 sheets instead of 10, but only by com- into cards with a ruler and a sharp blade.