MR Imaging Findings in Spinal Ligamentous Injury Philip F
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Synovial Joints Permit Movements of the Skeleton
8 Joints Lecture Presentation by Lori Garrett © 2018 Pearson Education, Inc. Section 1: Joint Structure and Movement Learning Outcomes 8.1 Contrast the major categories of joints, and explain the relationship between structure and function for each category. 8.2 Describe the basic structure of a synovial joint, and describe common accessory structures and their functions. 8.3 Describe how the anatomical and functional properties of synovial joints permit movements of the skeleton. © 2018 Pearson Education, Inc. Section 1: Joint Structure and Movement Learning Outcomes (continued) 8.4 Describe flexion/extension, abduction/ adduction, and circumduction movements of the skeleton. 8.5 Describe rotational and special movements of the skeleton. © 2018 Pearson Education, Inc. Module 8.1: Joints are classified according to structure and movement Joints, or articulations . Locations where two or more bones meet . Only points at which movements of bones can occur • Joints allow mobility while preserving bone strength • Amount of movement allowed is determined by anatomical structure . Categorized • Functionally by amount of motion allowed, or range of motion (ROM) • Structurally by anatomical organization © 2018 Pearson Education, Inc. Module 8.1: Joint classification Functional classification of joints . Synarthrosis (syn-, together + arthrosis, joint) • No movement allowed • Extremely strong . Amphiarthrosis (amphi-, on both sides) • Little movement allowed (more than synarthrosis) • Much stronger than diarthrosis • Articulating bones connected by collagen fibers or cartilage . Diarthrosis (dia-, through) • Freely movable © 2018 Pearson Education, Inc. Module 8.1: Joint classification Structural classification of joints . Fibrous • Suture (sutura, a sewing together) – Synarthrotic joint connected by dense fibrous connective tissue – Located between bones of the skull • Gomphosis (gomphos, bolt) – Synarthrotic joint binding teeth to bony sockets in maxillae and mandible © 2018 Pearson Education, Inc. -

Copyrighted Material
C01 10/31/2017 11:23:53 Page 1 1 1 The Normal Anatomy of the Neck David Bainbridge Introduction component’ of the neck is a common site of pathology, and the diverse forms of neck The neck is a common derived characteristic disease reflect the sometimes complex and of land vertebrates, not shared by their aquatic conflicting regional variations and functional ancestors. In fish, the thoracic fin girdle, the constraints so evident in this region [2]. precursor of the scapula, coracoid and clavi- Unlike the abdomen and thorax, there is no cle, is frequently fused to the caudal aspect of coelomic cavity in the neck, yet its ventral part the skull. In contrast, as vertebrates emerged is taken up by a relatively small ‘visceral on to the dry land, the forelimb separated from compartment’, containing the larynx, trachea, the head and the intervening vertebrae speci- oesophagus and many important vessels, alised to form a relatively mobile region – the nerves and endocrine glands. However, I neck – to allow the head to be freely steered in will not review these structures, as they do many directions. not represent an extension of the equine ‘back’ With the exception of the tail, the neck in the same way that the more dorsal locomo- remains the most mobile region of the spinal tor region does. column in modern-day horses. It permits a wide range of sagittal plane flexion and exten- sion to allow alternating periods of grazing Cervical Vertebrae 3–7 and predator surveillance, as well as frontal plane flexion to allow the horizon to be scan- Almost all mammals, including the horse, ned, and rotational movement to allow possess seven cervical vertebrae, C1 to C7 nuisance insects to be flicked off. -

Diagnosis of Atlantoaxial Instability Requires Clinical Suspicion To
al of S rn pi ou n Henderson Sr and Henderson Jr, J Spine 2017, 6:2 J e Journal of Spine DOI: 10.4172/2165-7939.1000364 ISSN: 2165-7939 Mini Review OMICS International Diagnosis of Atlantoaxial Instability Requires Clinical Suspicion to Drive the Radiological Investigation Fraser C Henderson Sr.1,2* and Fraser C Henderson Jr.3 1Doctors Community Hospital, Lanham, MD, USA 2The Metropolitan Neurosurgery Group, LLC, Chevy Chase, MD, USA 3Medical University of South Carolina, Charleston, SC, USA Introduction bending to the contralateral side, are often injured in motor vehicle collisions, and could be implicated in whiplash-associated disorders Atlantoaxial instability (AAI) occurs as a result of trauma, [15]. Failure of the alar ligament allows a 30% increased rotation to congenital conditions such as os odontoideum, neoplasm, infection the opposite side [16]. The atlantoaxial joint is ill-equipped to handle and degenerative connective tissue disorders such as rheumatoid the required multi-axial movements in the presence of ligamentous arthritis, genetic conditions such as HOX-D3 and Down syndrome, laxity or disruption [17]. Weakness of the muscles and ligaments, and heritable connective tissue disorders, emblematic of which are hormonal changes, infection, immunological problems, and congenital the Ehlers Danlos syndromes (EDS). Prototypical of disorders in dysmorphism may contribute to the overall mechanical dysfunction at which AAI is diagnosed, is rheumatoid arthritis (RA). Prior to the the C1-C2 motion segment. development of effective disease-modifying pharmacotherapies, 88% of RA patients exhibited radiographic evidence of C1-C2 involvement, Hypermobility of the AAJ is common in children, and up to 45° of in whom 49% were symptomatic and 20% myelopathic; ultimately, rotation may be observed in each direction. -
Digital Motion X-Ray Cervical Spine
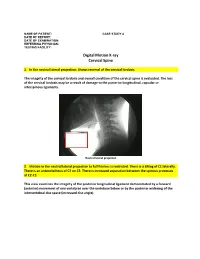
NAME OF PATIENT: CASE STUDY 4 DATE OF REPORT: DATE OF EXAMINATION: REFERRING PHYSICIAN: TESTING FACILITY: Digital Motion X-ray Cervical Spine 1. In the neutral lateral projection: Shows reversal of the cervical lordosis. The integrity of the cervical lordosis and overall condition of the cervical spine is evaluated. The loss of the cervical lordosis may be a result of damage to the posterior longitudinal, capsular or interspinous ligaments. Neutral lateral projection 2. Motion in the neutral lateral projection to full flexion: Is restricted. There is a tilting of C1 laterally. There is an anterolisthesis of C2 on C3. There is increased separation between the spinous processes at C2-C3. This view examines the integrity of the posterior longitudinal ligament demonstrated by a forward (anterior) movement of one vertebrae over the vertebrae below or by the posterior widening of the intervertebral disc space (increased disc angle). Widening of posterior disc space Anterolisthesis The integrity of the interspinous ligament is evaluated in the lateral flexion view. Damage to this ligament results in increased separation of the spinous processes in flexion. Damaged Interspinous Ligament Full flexion projection 3. Motion in the neutral lateral projection to full extension: Is restricted. There is a retrolisthesis of C4 on C5. This view examines the integrity of the anterior longitudinal ligament demonstrated by a backward (posterior) movement of one vertebrae over the vertebrae below or by the anterior widening of the intervertebral disc space (increased disc angle). Retrolisthesis Widening of the anterior disc Full Extension 4. Motion in the oblique flexion projection: Is restricted. There is gapping of the facet joints at C6-C7 bilaterally and C7-T1 bilaterally. -

Epithelia Joitns
NAME LOCATION STRUCTURE FUNCTION MOVEMENT Temporomandibular joint Condylar head of ramus of Synovial Diarthrosis Modified hinge joint mandible and glenoid fossa of Rotation and gliding temporal bone Biaxial Zygapophyseal joint Between articular processes of Synovial Diarthrosis Gliding 2 adjacent vertebrae Non axial Atlanto-Occipital joints Atlas and occipital condyle of Synovial Diarthrosis Ellipsoid occipital bone Biaxial Atlantoaxial joints Atlas and axis Synovial Diarthrosis Pivot Uniaxial Joints of vertebral arches Ligaments Fibrous Amphiarthrosis Syndesmoses Intervertebral symphyseal Intervertebral disk between 2 Cartilaginous Amphiarthrosis joints vertebrae Symphysis Costovertebral Head of ribs and body of Synovial Diarthrosis Gliding thoracic vertebra Non axial Costotrasnverse joints Tubercle of rib and transverse Synovial Diarthrosis Gliding process of thoracic vertebra Non axial Lumbosacral Joint Left and right zygopophyseal Laterally Synovial joint Intervertebral symphyseal joint Symphysis SternoclavicularJoint Clavicular notch articulates Synovial Diarthrosis Gliding with medial ends of clavicle Non Axial Manubriosternal Joint Hyaline cartilage junction Cartilaginous Synarthrosis Sternal Angle between manubrium and body Symphysis Xiphisternal Joint Cartilage between xiphoid Synchondrosis Synarthrosis process and body Synostoses Sternocostal Joint (1st) Costocartilage 1 with sternum Cartilaginous Synchondrosis Synarthrosis NAME Location Section Anterior longitudinal runs down anterior surface of vertebral body Vertebral column ligament Posterior longitudinal in canal, runs down posterior surface of vertebral body ligament Interspinous ligament Connects spinous processes Ligamentum flavum Connects laminae ! Intra-articular Disc Between articulating surface of sternum and clavicle Sternoclavicular Joint Costoclavicular ligament 1st rib to clavicle !. -

Duplication of the Alar Ligaments: a Case Report
Open Access Case Report DOI: 10.7759/cureus.2893 Duplication of the Alar Ligaments: A Case Report Asad Rizvi 1 , Joe Iwanaga 2 , Rod J. Oskouian 3 , Marios Loukas 4 , R. Shane Tubbs 5 1. St. Georges University School of Medicine, St. Georges, GRD 2. Seattle Science Foundation, Seattle, USA 3. Neurosurgery, Swedish Neuroscience Institute, Seattle, USA 4. Anatomical Sciences, St. George's University, St. George's, GRD 5. Neurosurgery, Seattle Science Foundation, Seattle, USA Corresponding author: Joe Iwanaga, [email protected] Abstract The alar ligament is one of the two strongest ligaments stabilizing the craniocervical junction. The literature describes many variations of the attachment, insertion, shape, and orientation of the alar ligament and an understanding of these variations is vital as they can lead to altered biomechanics or misinterpretation on imaging. Herein, we report, to our knowledge, the first case of duplication of the alar ligaments and discuss the anatomical variations present in the literature. Categories: Neurology, Pathology Keywords: alar ligament, duplication, craniocervical junction, variant, transverse occipital ligament, anatomy Introduction The craniocervical junction is composed of the atlantooccipital and the atlantoaxial joints. Several ligaments stabilize these joints, namely the transverse, alar, transverse occipital, accessory, lateral atlantooccipital, and apical ligaments [1]. The transverse and alar ligaments are the two strongest ligaments stabilizing the craniocervical junction with approximately 400 N and 200 N necessary until failure, respectively [1-2]. The alar ligaments are fibrous cords that attach to the dens bilaterally and insert on the base of the skull. They function to limit axial rotation and lateral bending on the contralateral side, and flexion secondarily [1- 2]. -

Posterior Longitudinal Ligament Status in Cervical Spine Bilateral Facet Dislocations
Thomas Jefferson University Jefferson Digital Commons Department of Orthopaedic Surgery Faculty Papers Department of Orthopaedic Surgery November 2005 Posterior longitudinal ligament status in cervical spine bilateral facet dislocations John A. Carrino Harvard Medical School & Brigham and Women's Hospital Geoffrey L. Manton Thomas Jefferson University Hospital William B. Morrison Thomas Jefferson University Hospital Alex R. Vaccaro Thomas Jefferson University Hospital and The Rothman Institute Mark E. Schweitzer New York University & Hospital for Joint Diseases Follow this and additional works at: https://jdc.jefferson.edu/orthofp Part of the Orthopedics Commons LetSee next us page know for additional how authors access to this document benefits ouy Recommended Citation Carrino, John A.; Manton, Geoffrey L.; Morrison, William B.; Vaccaro, Alex R.; Schweitzer, Mark E.; and Flanders, Adam E., "Posterior longitudinal ligament status in cervical spine bilateral facet dislocations" (2005). Department of Orthopaedic Surgery Faculty Papers. Paper 3. https://jdc.jefferson.edu/orthofp/3 This Article is brought to you for free and open access by the Jefferson Digital Commons. The Jefferson Digital Commons is a service of Thomas Jefferson University's Center for Teaching and Learning (CTL). The Commons is a showcase for Jefferson books and journals, peer-reviewed scholarly publications, unique historical collections from the University archives, and teaching tools. The Jefferson Digital Commons allows researchers and interested readers anywhere in the world to learn about and keep up to date with Jefferson scholarship. This article has been accepted for inclusion in Department of Orthopaedic Surgery Faculty Papers by an authorized administrator of the Jefferson Digital Commons. For more information, please contact: [email protected]. -

Chapter 02: Netter's Clinical Anatomy, 2Nd Edition
Hansen: Netter's Clinical Anatomy, 2nd Edition - with Online Access 2 BACK 1. INTRODUCTION 4. MUSCLES OF THE BACK REVIEW QUESTIONS 2. SURFACE ANATOMY 5. SPINAL CORD 3. VERTEBRAL COLUMN 6. EMBRYOLOGY FINAL 1. INTRODUCTION ELSEVIERl VertebraeNOT prominens: the spinous process of the C7- vertebra, usually the most prominent The back forms the axis (central line) of the human process in the midline at the posterior base of body and consists of the vertebral column, spinal cord, the neck supporting muscles, and associated tissues (skin, OFcon- l Scapula: part of the pectoral girdle that sup- nective tissues, vasculature, and nerves). A hallmark of ports the upper limb; note its spine, inferior human anatomy is the concept of “segmentation,” and angle, and medial border the back is a prime example. Segmentation and bilat l Iliac crests: felt best when you place your eral symmetry of the back will be obvious as you hands “on your hips”; an imaginary horizontal study the vertebral column, the distribution of the line connecting the crests passes through the spinal nerves, the muscles of th back, and its vascular spinous process of the L4 vertebra and the supply. intervertebral disc of L4-L5, a useful landmark Functionally, the back is involved in three primary for a lumbar puncture or epidural block tasks: l Posterior superior iliac spines: an imaginary CONTENThorizontal line connecting these two points l Support: the vertebral column forms the axis of passes through the spinous process of S2 (second the body and is critical for our upright posture sacral segment) (standing or si ting), as a support for our head, as an PROPERTYattachment point and brace for move- 3. -

Download PDF File
Folia Morphol. Vol. 70, No. 2, pp. 61–67 Copyright © 2011 Via Medica R E V I E W A R T I C L E ISSN 0015–5659 www.fm.viamedica.pl Human ligaments classification: a new proposal G.K. Paraskevas Department of Anatomy, Medical School, Aristotle University of Thessaloniki, Greece [Received 24 January 2011; Accepted 22 March 2011] A high concern exists among physicians about surgically important ligaments such as cruciate and collateral ligaments of the knee, patellar ligament, tibiofibular syndesmosis, collateral ligaments of the ankle, and coracoclavicular ligament. However, the classification of the ligaments is insufficient in the literature, due to their origin from connective tissue. A new classification is proposed, based on various parameters such as the macroscopic and microscopic features, the function and the nature of their attachment areas. (Folia Morphol 2011; 70, 2: 61–67) Key words: ligaments, classification, Nomina Anatomica INTRODUCTION connective tissue surrounding neurovascular bundles There was always some confusion concerning the or ducts as “true ligaments” [4]. classification of ligaments of the human body, presu- The “false ligaments”, could be subdivided in the mably due to their origin from the connective tissue following categories: that is considered a low quality tissue compared to oth- a) Splachnic ligaments, which are further subdivid- ers. Moreover, orthopaedists are focused only on surgi- ed into “peritoneal” (e.g. phrenocolic ligament), cally important ligaments. For these reasons there is an “pericardiac” (e.g. sternopericardial ligaments), absence of a well-designated classification system that “pleural” (e.g. suprapleural membrane), and subdivides the ligaments into subgroups according to “pure splachnic ligaments” (e.g. -

Variability of Morphology and Signal Intensity of Alar Ligaments in Healthy Volunteers Using MR ORIGINAL RESEARCH Imaging
Variability of Morphology and Signal Intensity of Alar Ligaments in Healthy Volunteers Using MR ORIGINAL RESEARCH Imaging N. Lummel BACKGROUND AND PURPOSE: Evaluation of alar traumatic injuries by using MR imaging is frequently C. Zeif performed. This study investigates the variability of morphology and signal intensity of alar ligaments in healthy volunteers so that pathology can be more accurately defined. A. Kloetzer J. Linn MATERIALS AND METHODS: Fifty healthy volunteers were examined on a 1.5T MR imaging scanner Ϫ H. Bru¨ ckmann with 2-mm PD weighted sequences in 3 planes. Delineation of the alar ligaments in 3 planes and signal-intensity characteristics on sagittal planes were analyzed by using a 4-point grading scale. H. Bitterling Variability of courses and morphologic characteristics were described. RESULTS: Delineation of alar ligaments was best viewed in the coronal plane, followed by the sagittal and axial planes. In the sagittal view, 6.5% of alar ligaments appeared homogeneously dark. Hyper- intense signal intensity in up to one-third of the cross-sectional area was present in 33% of cases; in up to two-thirds of the cross-sectional area, in 45% of cases; and in more than two-thirds of the cross-sectional area, in 15% of cases. Of alar ligaments, 58.5% ascended laterally, 40.5% ran horizontally, and 1% descended laterally. The cross-sectional area was round in 41.5%, oval in 51.5%, and winglike in 6.5%. CONCLUSIONS: On 1.5T MR imaging, the alar ligaments can be delineated best in the coronal and sagittal planes. Our data indicate a remarkable variability of morphology and course as well as signal intensity. -

Successful Treatment of Supraspinous and Interspinous Ligament Injury with Ultrasound-Guided Platelet-Rich Plasma Injection
HSSXXX10.1177/1556331621992312HSS Journal®: The Musculoskeletal Journal of Hospital for Special SurgeryCreighton et al 992312case-report2021 Case Report HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery Successful Treatment of Supraspinous 1 –4 © The Author(s) 2021 Article reuse guidelines: and Interspinous Ligament Injury sagepub.com/journals-permissions DOI:https://doi.org/10.1177/1556331621992312 10.1177/1556331621992312 With Ultrasound-Guided Platelet-Rich journals.sagepub.com/home/hss Plasma Injection: Case Series Andrew Creighton, DO1, Roger A. Sanguino, MS1, Jennifer Cheng, PhD1, and James F. Wyss, MD, PT1 Keywords supraspinous ligament, interspinous ligament, platelet-rich plasma, ultrasound, nonoperative treatments, lumbar spine Received October 18, 2020. Accepted October 21, 2020. Introduction running volume. The LBP intensity ranged from 3 to 9/10 and was worse with prolonged standing, sitting, or running. Low back pain (LBP) is a very common complaint and is He reported no improvement with 3 prior courses of PT, now the number one cause of disability across the globe NSAIDs, and use of a seat cushion. Physical examination [5,13]. Both the supraspinous ligament (SSL) and interspi- revealed mild right thoracolumbar curvature. Tenderness nous ligament (ISL) form part of the posterior ligamentous was appreciated over the L5 spinous process and interspi- complex, which is believed to play an integral role in the nous region above and below L5. Strength, sensation, and stability of the thoracolumbar spine [8]. The SSL begins at reflexes were normal. the C7 spinous process and extends to L3 and L4 in 22% Radiographs were unremarkable. Magnetic resonance and 74% of adults, respectively [11]. -

Diagnostic Utility of Increased STIR Signal in the Posterior Atlanto-Occipital and Atlantoaxial Membrane Complex on MRI in Acute C1–C2 Fracture
Published July 6, 2017 as 10.3174/ajnr.A5284 ORIGINAL RESEARCH SPINE Diagnostic Utility of Increased STIR Signal in the Posterior Atlanto-Occipital and Atlantoaxial Membrane Complex on MRI in Acute C1–C2 Fracture X Y.-M. Chang, X G. Kim, X N. Peri, X E. Papavassiliou, X R. Rojas, and X R.A. Bhadelia ABSTRACT BACKGROUND AND PURPOSE: Acute C1–C2 fractures are difficult to detect on MR imaging due to a paucity of associated bone marrow edema. The purpose of this study was to determine the diagnostic utility of increased STIR signal in the posterior atlanto-occipital and atlantoaxial membrane complex (PAOAAM) in the detection of acute C1–C2 fractures on MR imaging. MATERIALS AND METHODS: Eighty-seven patients with C1–C2 fractures, 87 with no fractures, and 87 with other cervical fractures with acute injury who had both CT and MR imaging within 24 hours were included. All MR images were reviewed by 2 neuroradiologists for the presence of increased STIR signal in the PAOAAM and interspinous ligaments at other cervical levels. Sensitivity and specificity of increased signal within the PAOAAM for the presence of a C1–C2 fracture were assessed. RESULTS: Increased PAOAAM STIR signal was seen in 81/87 patients with C1–C2 fractures, 6/87 patients with no fractures, and 51/87 patients with other cervical fractures with 93.1% sensitivity versus those with no fractures, other cervical fractures, and all controls. Specificity was 93.1% versus those with no fractures, 41.4% versus those with other cervical fractures, and 67.2% versus all controls for the detection of acute C1–C2 fractures.