Adult Cardiology
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Information Memorandum Modernization of Philippine Orthopedic Center
Information Memorandum Modernization of Philippine Orthopedic Center November 2012 Disclaimer Information contained in this Information Memorandum (IM) document is for reference purposes only. The information and terms and conditions contained in the Instructions to Bidders, the BOT Agreement and its Annexes, including the Minimum Performance Standards and Specifications shall be made available as separate documents to the bidders and shall be considered binding upon the bidders. In case of any conflict between the information and terms in this IM and the BOT Agreement and its Annexes, including the Minimum Performance Standards and Specifications, and the Instructions to Bidders, the information and terms specified in the BOT Agreement and its Annexes, including the Minimum Performance Standards and Specifications and the Instructions to Bidders, shall prevail. This IM does not purport to be all-inclusive or to contain all of the information that a bidder may consider material or desirable in making its decision to participate in the bidding. No representation or warranty, express or implied, is made, or responsibility of any kind is or will be accepted by the Department of Health, or the GOP or any of its agencies, with respect to the accuracy and completeness of the information contained in this IM. The Department of Health may amend or replace any of the information contained in this memorandum at any time, without giving any prior notice or providing any reason. In furnishing this IM, the Department of Health, or the GOP or any of its agencies undertakes no obligation to provide recipients with access to any additional information, or to update, or to correct any inaccuracies which may become apparent in this IM or any other information made available in connection with the project. -

Volume 21 Number 1, January-June 2016
ISSN 0118-9034 Philippine Heart Center Journal Vol. 21 No. 1 January - June 2016 Editorial Lessons from Galapagos Gilbert C. Vilela, MD Consultant’s Corner Comparison of the New Mayo Clinic Risk Scores and Clinical SYNTAX Score in Predicting Adverse Cardiovascular Outcomes Following Percutaneous Coronary Intervention at the Philippine Heart Center Helenne Joie M. Brown, MD; James O. Ho Khe Sui, MD; Catherine C. Tan, MD; Vergel A. Quiogue, MD Original Articles Effectiveness of an Accelerated Phase II as Compared to the Comparison of the Clinical Outcome and Cost of Transcatheter Standard Cardiac Rehabilitation Program in Improving Exercise Device Occlusion and Surgical Closure of Isolated Ventricular Capacity and Quality of Life Septal Defect Benjamin Jose C. Quito, MD; Marcelo R. Esguerra, MD; Leandro Bernadette B. Valdez, MD; Juan C. Reganion, MD; Jean Antonio C. Bongosia, MD; Edgardo E. Ebba, MD G. Villareal, MD; Juliet J. Balderas, MD Association of Nutritional Status using Mini-Nutritional Assessment The Clinical and Procedural Outcome of Patients Undergoing Trans- ® Radial Approach vs. Trans-Femoral Approach in Percutaneous Short Form (MNA -SF) with Risk of Exacerbation Among Elderly Coronary Intervention COPD Patients Phillip C. Ines, MD; Norberto A. Tuaño, MD; James O. Ho Khe Sui, Peter Ian B. Tabar, MD; Aileen Guzman-Banzon, MD; Ma. Encarnita- MD; Noe A. Babilonia, MD Blanco-Limpin, MD A Cohort Study on the Use of Absorbable Sutures vs. Steel Wires in Association of Door-to-Balloon Time with Clinical Outcomes in Post- Sternal Closure in Pediatric Patients after Cardiovascular Surgery: Primary Percutaneous Coronary Intervention Patients a Philippine Heart Center experience Ed D. -

Metro Manila AFFILIATED HOSPITALS, CLINICS & Tel No: (02) 874 2506 / (02) 874 HOSPITAL of the INFANT JESUS SAN RAMON HOSPITAL INC
LAS PIÑAS Tel No.: (02) 682 2222 ADVENTIST MANILA MEDICAL Quezon Ave cor. Sct Magbanua, EAST MANILA HOSPITAL Blanket accreditation of all doctors CENTER Diliman, Quezon City MANAGERS CORP (OUR LADY OF 1975 Donada St., Pasay City Tel No: (02) 3723825 ALABANG MEDICAL CLINIC LOURDES HOSPITAL) SALVE REGINA HOSPITAL Tel. No: (02) 5259191 (Las Piñas Branch) Alabang –Zapote Sta. Mesa, Manila Marcos Hi-Way, Marikina City; Blanket accreditation with doctors DE LOS SANTOS MEDICAL CENTER Road Cor. Pelayo Village Talon, Las Tel No: (02) 716-8001 to 20 Trunkline: 477-4832/ 477-4847 201 E Rodriguez Sr. Ave, Quezon Piñas City SAN JUAN DE DIOS EDUCATIONAL City, 1112 Metro Manila AFFILIATED HOSPITALS, CLINICS & Tel No: (02) 874 2506 / (02) 874 HOSPITAL OF THE INFANT JESUS SAN RAMON HOSPITAL INC. FOUNDATION INC. HOSPITAL Tel. No: 893 5762 DENTISTS as of (April 29, 2019) 0164 / 0925 729 5550 Laong Laan Road, Sampaloc, 108 Gen.Ordonez, Marikina, 1811 Roxas Boulevard, Pasay City; Blanket accreditation with doctors Manila MMla; Trunkline: 831-9731, 831-6921 DILIMAN DOCTORS HOSPITAL Please call/text our 24/7 HOTLINE Tel. No: 7312771 Blanket accreditation of doctors 251 Commonwealth Ave, ALABANG MEDICAL CLINIC Blanket Accreditation with Doctors Tel No: (02) 941 8632 Matandang Balara, Quezon City, numbers for proper endorsement PASIG (Almanza Branch) 2F Susana Arcade 1119 Metro Manila GLOBE: 09778042137 #476 Real Street Almanza, Las Piñas MANILA DOCTORS HOSPITAL ST. VICTORIA HOSPITAL Tel. No (02) 883 6900 SUN: 09256521927 City United Nation Avenue, Malate, J.P.Rizal, Marikina, Metro Manila; MEDCOR PASIG HOSPITAL AND PLDT: 02 (2084611) Tel No: (02) 800 3840 / (02) 800 Manila; Trunkline: 942-2022 MEDICAL CENTER / MARIKINA DR. -

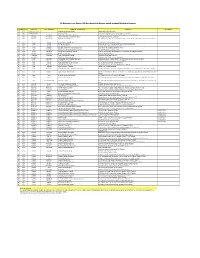
Continuing Professional Development (Cpd) Council for Physicians List of Accredited Providers As of February 2, 2018
CONTINUING PROFESSIONAL DEVELOPMENT (CPD) COUNCIL FOR PHYSICIANS LIST OF ACCREDITED PROVIDERS AS OF FEBRUARY 2, 2018 ACCREDITATION TELEPHONE NO. NAME OF PROVIDER ADDRESS E-MAIL ADDRESS DATE OF EXPIRATION NO. FAX NO. [email protected] / Philippine Medical Association PMA Bldg., North Avenue, Quezon 929-6366 1 2012-001 www.philippinemedicalassociation. 13-Feb-21 (PMA) City Fax: 929-6951 org College of Medicine, University of 547 Pedro Gil St., Ermita, Manila, 2 2012-002 [email protected] 0918-905-0862 18-Apr-20 the Philippines Philippines, 1000 Rm. 2007 Medical Arts Bldg., UST 749-9707 Fax No. 740- 3 2012-003 Dementia Society of the Philippines www.dementia.org.ph 14-Feb-15 Hospital, España, Manila 9725 [email protected] / Unit 25 Facilities Centre, #548 (632) 531-1278/ 534- 4 2012-004 Diabetes Philippines [email protected]/ 12-Jul-20 Shaw Blvd., Mandaluyong City 9559 www.diabetesphil.org Unit 205 The Garden Heights [email protected] / 584-2700 5 2012-005 Pain Society of the Philippines, Inc. Condominium 268 E. Rodriguez Sr. [email protected] / 13-Mar-20 Cel: 0917-6213705 Avenue, Quezon city www.painsociety.ph Unit 4 Metro Square Townehomes, 374-1855 Pediatric Infectious Disease [email protected]/ 6 2012-006 No. 35 Scout Tuazon cor. Scout de Fax No. 412-6998 13-Feb-21 Society of the Philippines (PIDSP) Guia, Quezon City www.pidsphil.org Cel: 0917-834-9837 Room 403 PPS Building, #52 Perinatal Association of the [email protected]/ 925-3538 7 2012-007 Kalayaan Avenue, Brgy. Malaya, 13-Feb-21 Philippines, Inc. -
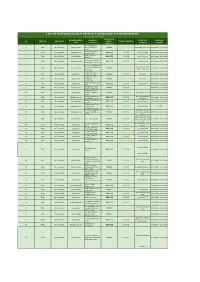
List of Licensed Covid-19 Testing Laboratory in the Philippines
LIST OF LICENSED COVID-19 TESTING LABORATORY IN THE PHILIPPINES ( as of November 26, 2020) OWNERSHIP MUNICIPALITY / NAME OF CONTACT LICENSE REGION PROVINCE (PUBLIC / TYPE OF TESTING # CITY FACILITY NUMBER VALIDITY PRIVATE) Amang Rodriguez 1 NCR Metro Manila Marikina City Memorial Medical PUBLIC Cartridge - Based PCR 8948-0595 / 8941-0342 07/18/2020 - 12/31/2020 Center Asian Hospital and 2 NCR Metro Manila Muntilupa City PRIVATE rRT PCR (02) 8771-9000 05/11/2020 - 12/31/2020 Medical Center Chinese General 3 NCR Metro Manila City of Manila PRIVATE rRT PCR (02) 8711-4141 04/15/2020 - 12/31/2020 Hospital Detoxicare Molecular 4 NCR Metro Manila Mandaluyong City PRIVATE rRT PCR (02) 8256-4681 04/11/2020 - 12/31/2020 Diagnostics Laboratory Dr. Jose N. Rodriguez Memorial Hospital and (02) 8294-2571; 8294- 5 NCR Metro Manila Caloocan City PUBLIC Cartridge - Based PCR 08/13/2020 - 12/31/2020 Sanitarium 2572 ; 8294-2573 (GeneXpert)) Lung Center of the 6 NCR Metro Manila Quezon City PUBLIC rRT PCR 8924-6101 03/27/2020 - 12/31/2020 Philippines (LCP) Lung Center of the 7 NCR Metro Manila Quezon City Philippines PUBLIC Cartridge - Based PCR 8924-6101 05/06/2020 - 12/31/2020 (GeneXpert) Makati Medical Center 8 NCR Metro Manila Makati City PRIVATE rRT PCR (02) 8888-8999 04/11/2020 - 12/31/2020 (HB) Marikina Molecular 9 NCR Metro Manila Marikina City PUBLIC rRT PCR 04/30/2020 - 12/31/2020 Diagnostic laboratory Philippine Genome 10 NCR Metro Manila Quezon City Center UP-Diliman PUBLIC rRT PCR 8981-8500 Loc 4713 04/23/2020 - 12/31/2020 (NHB) Philippine Red Cross - (02) 8790-2300 local 11 NCR Metro Manila Mandaluyong City PRIVATE rRT PCR 04/23/2020 - 12/31/2020 National Blood Center 931/932/935 Philippine Red Cross - 12 NCR Metro Manila City of Manila PRIVATE rRT PCR (02) 8527-0861 04/14/2020 - 12/31/2020 Port Area Philippine Red Cross 13 NCR Metro Manila Mandaluyong City Logistics and PRIVATE rRT PCR (02) 8790-2300 31/12/2020 Multipurpose Center Research Institute for (02) 8807-2631; (02) 14 NCR Metro Manila Muntinlupa City Tropical Medicine, Inc. -

The SOLID-TIMI 52 Randomized Clinical Trial
Supplementary Online Content O’Donoghue ML, Braunwald E, White HD, et al. Effect of darapladib on major coronary events after an acute coronary syndrome: the SOLID-TIMI 52 randomized clinical trial. JAMA. doi:10.1001/jama.2014.11061 eAppendix 1. SOLID-TIMI 52 trial - Trial Leadership & Investigators eAppendix 2. Inclusion and Exclusion Criteria eAppendix 3. Clinical Endpoint Definitions eFigure 1. Cumulative Incidence Curves for the Secondary Endpoint CV Death, MI or Stroke eFigure 2. Subgroups of Interest for the Secondary Composite Endpoint of CV Death, MI or Stroke eTable. Summary of MI According to the Universal Classification of MI by Randomized Treatment Arm eReferences This supplementary material has been provided by the authors to give readers additional information about their work. © 2014 American Medical Association. All rights reserved. Downloaded From: https://jamanetwork.com/ on 09/27/2021 O’Donoghue et al., SOLID-TIMI 52 trial - Supplementary Appendix eAppendix 1. SOLID-TIMI 52 trial - Trial Leadership & Investigators SOLID-TIMI 52 Executive Steering Committee members Chair: Eugene Braunwald (TIMI Study Group, Brigham and Women’s Hospital, Boston, MA, US) Global Principal Investigator: Christopher P. Cannon (TIMI Study Group, Brigham and Women’s Hospital, Boston, MA, US) Members: Christoph Bode (Medizinische Universitatsklinik Abt. Innere Medizin III, Freiberg, Germany) Judith Hochman (New York University School of Medicine, New York, NY, US) Aldo P. Maggioni (AMNCO Research Center, Firenze, Italy) Ph. Gabriel Steg (INSERMU698,Hôpital Bichat-CI. Bernard, Paris, France) Patrick Serruys (Erasmus University, Rotterdam, Netherlands) Douglas Weaver (Henry Ford Heart & Vascular Institute, Detroit, MI, US) Harvey D. White (Auckland City Hospital, Auckland University, Auckland, New Zealand) GlaxoSmithKline members: Mary Ann Lukas (GlaxoSmithKline, Philadelphia, PA, US) Richard Y. -

3 – Growth Centers
ANNEX 3 GROWTH CENTERS CBD-KNOWLEDGE COMMUNITY DISTRICT CUBAO GROWTH DISTRICT BATASAN-NGC GROWTH CENTER NOVLIHES-LAGRO GROWTH CENTER BALINTAWAK-MUNOZ GROWTH CENTER Annex 3: Growth Centers 1. CBD-KNOWLEDGE COMMUNITY DISTRICT 1.1. Area Coverage and Population The proposed CBD-Knowledge Community District has total area of 1,862 hectares and covers 22 barangays in Districts I, III and IV. It embraces the North, East, South and West triangles, UP Campus including the UP-Ayala Techno Hub, Ateneo de Manila University, Miriam College, Balara Filtration Plant, the vicinity of SM North EDSA and Veteran’s Memorial Medical Center and the residential communities in UP Village, Teacher’s Village, Pinyahan, Krus na Ligas, Malaya and Xavierville areas. 1.2. District Boundary The study area is bounded by the following: North: Area lot deep northside of Nueva Vizcaya St. and Road 3 up to lot deep westside of Mindanao Avenue then northward up to lot deep northside of Road 10 then eastward up to lot deep Westside of Visayas Avenue then northward up to lot deep northside of Central Avenue then eastward towards Commonwealth Avenue extending up to lot deep eastside of Katipunan Avenue. East: Area lot deep eastside of Katipunan Avenue going towards lot deep northside of Mactan St. then eastward towards lot deep eastside of Balintawak St. then southward to QC-Marikina politicalBoundary then westward through periphery of MWSS Balara Homesite up to MWSSAqueduct then southward up to lot deepEastside of Katipunan Avenue then Southward towards Mangyan St. and Eastward along southern periphery of LaVista Subdivision up to QC-Marikina politicalBoundary then southward up to Aurora Boulevard. -

Institute for Solidarity in Asia Philippine Heart Center Gold Trailblazer Award
SECOND QUARTER 2018 By: Charisse G. Enrique, MHA Marketing Specialist, Management Services Office With much honor and delight, the Philippine Heart Center (PHC) hereby announces its most recent recognition for meeting the international standards of excellence in quality care & service - the much coveted DIAMOND ACCREDITATION from the Accreditation Canada International. PHC is the first and only government hospital in Asia to receive the highest level of recognition from an international accrediting body who passionately adheres to healthcare safety and quality service. PHC Receives Diamond Accreditation from ACI— Ms. Marrieta A. Velasco- Acting Deputy Executive Director-Nursing Services, Dr. Joel M. Abanilla- PHC Executive Director, Leslee Thompson - ACI CEO, Ms. Ma. Theresa C. Barrameda-Quality Assurance, Coordinator, Katerina Tarasova - ACI Executive Director and Dr. Juliet J. Balderas-Chairman- Head, Office of Strat- Institute for Solidarity in Asia conferred Philippine Heart Center “Institutionalized” on the last stage of the Performance Governance System with Gold Trailblazer Award For illumination of darkened path in search of development For your tireless pursuit of excellence & integrity For your courageous efforts to lift the standards of governance in the public sector The Philippine Heart Center has surpassed the many challenges in the implementation of the Performance Governance System (PGS), such as completing the PGS Journey all the way to the level of Institutionalization, budgetary constraints, sustaining the enthusiasm of the OSM and the entire hospital staff and defining clear and real roles for all concerned in the external Multi-Sectoral Governance Council (MSGC). However tough the challenges may be, PHC remains focused and optimistic as it moves towards PGS Institutionalization. -

Philippine Heart Center Journal Vol 13, No.2, April-December 2007
ISSN 0118-9034 Philippine Heart Center Journal Vol 13, No.2, April-December 2007 Editorial Translating Research Into Practice (TRIP): from bench to where? Comparison of CPIS (clinical pulmonary infection score) and Clinical Leahdette Padua, MD, FPCP Criteria in the Diagnosis of Ventilator-associated Pneumonia in ICU Complex Patients Original Articles Jaime C. Tan, MD; Aileen Guzman-Banzon, MD; Fernando Ayuyao, MD; Teresita De Guia, MD Aortic Assessment of Left Ventricular Function by Doppler Velocity Tissue Imaging of the Mitral Annulus in Patients with A prospective cohort study on the effects of pulmonary rehabilitation Mitral Stenosis before and after Percutaneous Transvenous Mitral on Non-COPD lung disease Commissurotomy Glynna A. Ong-Cabrera MD, Percival A. Punzal MD, Teresita S. De Neil D. Erguiza,MD; Edwin S. Tucay, MD; Viannely Berwyn Guia MD, Ma. Encarnita Blanco-Limpin MD Flores,MD; Romeo J. Santos,MD; Raul D. Jara,MD. Pre-flight Testing of Children and Adolescent with Asthma A Comparative Study of Bioimpedance and the Thermodilution Alfredo L. Bongo Jr., M.D.,Percival Punzal, M.D., Abner Koh, M.D., Method in Cardiac Output Monitoring After Coronary Artery Bypass Nerissa A. De Leon, M.D., Milagros S. Bautista, M.D., Teresita S. Grafting De Guia, M.D. Joseph George G. Tamayo, MD; Santos-Jose Abad, MD Comparative Assessment of Asthma Control Test (ACT) and GINA Diagnosis of Arterial Disease of the Lower Extremities With Duplex Classification including FEV1 in predicting asthma severity Scanning: A Validation Study In Patients After Myocardial Infarction Maria Monica R. Mendoza, M.D. Bernice Ong-Dela Cruz, MD, Aileen In Patients with LV Dysfunction V. -

Philippines: Medical Facilities
List of medical facilities in the Philippines Prepared by British Embassy Manila www.gov.uk The following list of medical facilities has been prepared by the British Embassy Manila for the convenience of British Nationals who may require these services and assistance in the Philippines. It is provided on the understanding that we (the British Embassy/Consulate) do not assume or undertake any legal responsibility, to you, or those affected, if you choose to take it into account when instructing a medical facility or practitioner. Further and alternatively, we cannot accept any liability to any person or company for any financial loss or damage arising from the use of this information or from any failure to give information. Our aim is to provide our customers with as much relevant information to enable them to make better informed decisions but our lists are not recommendations and should not be treated as such Updated: 1 December 2020 List of medical facilities in Metro Manila Facilities listed below has told us the following things: they have English speaking staff you will need to pay for treatment EHIC Cards are not accepted; repayment plans aren’t available (European Economic Area (EEA) or Switzerland only) *This list is arrange in alphabetical order ADVENTIST MEDICAL CENTER MANILA (FORMERLY MANILA SANITARIUM) 1975 Donada Street corner San Juan Pasay City 1300 Telephone: +63 (2) 8525 9191 to 98 Emergency Room +63 (2) 8525 9191 local 151, 152 Website: https://www.amcmanila.org/default.aspx Type: Private hospital ASIAN HOSPITAL AND MEDICAL CENTER 2205 Civic Drive Filinvest Corporate City Alabang Mutinlupa City 1780 Telephone: +63 (2) 8771 9000 Emergency Room +63 (2) 8771 9000 local 8195,8196 Website: http://www.asianhospital.com/ Email: [email protected] Type: Private hospital CHINESE GENERAL HOSPITAL 286 Blumentritt Street Barangay 372 Zone 37 District 3 Sta. -
Provider List Astra Life for Overseas
RS Rekanan Luar Negeri AAI dan Astra Life khusus untuk product Medicare Premier NO CONTINENT COUNTRY CITY / PROVINCE NAME OF THE HOSPITAL ADDRESS TELEPHONE 1 ASIA Brunei Darussalam Jerudong Park Medical Centre Jerudong Park, BG3122, Brunei 2 ASIA Brunei Darussalam Gleneagles JPMC Jerudong Park Medical Centre , Brunei Darussalam BN2311 3 ASIA Cambodia Siam Reap Royal Angkor International Hospital National Route #6, Phum Kasekam, Khum Sra Ngea, Siem Reap, Cambodia 4 ASIA Cambodia Phnom Penh Sen Sok International University Hospital Street 1986, Phnom Penh, Cambodia 5 ASIA Cambodia Phnom Penh Royal Phnom Penh Hospital Toeuk Thla Village, Russian Federation Blvd.Sangkat Toeuk Thla,Khan Russey Keo, Phnom Pehn, Cambodia 6 ASIA China Beijing Beijing United Family Hospital 2 Jiangtai Rd, Chaoyang, Beijing, China 7 ASIA China Beijing Beijing Eden Hospital E-Building, No.51, Kunming Lake South Road Haidian District,Beijing 8 ASIA China Beijing Tiantan Puhua Hospital 12 Tiantan Nanli, Dongcheng, Beijing, China 9 ASIA China Shanghai Shanghai United Family Hospital and Clinics 1139 Xianxia Rd, Changning, Shanghai, China 10 ASIA China Shanghai Shanghai East International Medical Center 150 Jimo Rd, Pudong, Shanghai, China 11 ASIA China Guangzhou Guangzhou United Family Hospital 1F Annex, PICC Building, 301 Guangzhou Ave, Yuexiu District, Guangzhou 510600 12 ASIA Hong Kong Stubbs Rd HK Adventist Hospital 40 Stubbs Rd, Hong Kong 13 ASIA Hong Kong Tsuen Wan Tsuen Wan Adventist Hospital Hong Kong, Tsuen Raja Circuit 199 14 ASIA Hong Kong Matilda International Hospital 41 Mount Kellett Road, The Peak, Hong Kong 15 ASIA India New Delhi Indraprastha Apollo Hospitals (New Delhi) Indraprastha Apollo Hospitals, Sarita Vihar, Delhi-Mathura Road, New Delhi-110044 16 ASIA India Chennai Apollo Hospitals Chennai 21,Greams Road off.Greams lane, Chennai-600006 17 ASIA India Kolkata Apollo Gleneagles Hospital (Kolkata) No. -
Project for Strengthening the ASEAN Regional Capacity on Disaster Health Management
Ministry of Public Health (MOPH) National Institute for Emergency Medicine (NIEM) Kingdom of Thailand Official Project of Association of Southeast Asian Nations (ASEAN) ←文字上 / 上から 70mm Project for ←文字上 / 上から 75mm Strengthening the ASEAN Regional Capacity on Disaster Health Management Final Report ←文字上 / 下から 95mm ←文字上 / 下から 70mm July 2019 Japan International Cooperation Agency (JICA) Koei Research & Consulting Inc. EI JR 19-091 Project for Strengthening the ASEAN Regional Capacity on Disaster Health Management FINAL REPORT Table of Contents Glossary Chapter 1 Outline of the Project ................................................................................................................. 1-1 1.1 Background ........................................................................................................................................ 1-1 1.2 Overview of the Project ..................................................................................................................... 1-2 1.3 Overall Flow ...................................................................................................................................... 1-3 1.3.1 Preparatory Works (July 2016-February 2017) ......................................................................... 1-3 1.3.2 Output 1: Coordination platform on disaster health management is set up. .............................. 1-4 1.3.3 Output 2: Framework of regional collaboration practices is developed. ................................... 1-6 1.3.4 Output 3: Tools for effective