Morphological Study of Middle Cardiac Vein in Human Hearts of North Western up and Its Application for Interventional Procedure
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Download PDF File
Folia Morphol. Vol. 78, No. 2, pp. 283–289 DOI: 10.5603/FM.a2018.0077 O R I G I N A L A R T I C L E Copyright © 2019 Via Medica ISSN 0015–5659 journals.viamedica.pl Observations of foetal heart veins draining directly into the left and right atria J.H. Kim1, O.H. Chai1, C.H. Song1, Z.W. Jin2, G. Murakami3, H. Abe4 1Department of Anatomy and Institute of Medical Sciences, Chonbuk National University Medical School, Jeonju, Korea 2Department of Anatomy, Wuxi Medical School, Jiangnan University, Wuxi, China 3Division of Internal Medicine, Jikou-kai Clinic of Home Visits, Sapporo, Japan 4Department of Anatomy, Akita University School of Medicine, Akita, Japan [Received: 19 June 2018; Accepted: 8 August 2018] Evaluation of semiserial sections of 14 normal hearts from human foetuses of gestational age 25–33 weeks showed that all of these hearts contained thin veins draining directly into the atria (maximum, 10 veins per heart). Of the 75 veins in these 14 hearts, 55 emptied into the right atrium and 20 into the left atrium. These veins were not accompanied by nerves, in contrast to tributaries of the great cardiac vein, and were negative for both smooth muscle actin (SMA) and CD34. However, the epithelium and venous wall of the anterior cardiac vein, the thickest of the direct draining veins, were strongly positive for SMA and CD34, respectively. In general, developing fibres in the vascular wall were positive for CD34, while the endothelium of the arteries and veins was strongly positive for the present DAKO antibody of SMA. -

Anomalous Middle Cardiac Vein Draining Into the Left Atrium
IMAGES IN THIS ISSUE Cardiovascular Disorders http://dx.doi.org/10.3346/jkms.2016.31.8.1179 • J Korean Med Sci 2016; 31: 1179-1180 Anomalous Middle Cardiac Vein Draining into the Left Atrium Jihyun Sohn,1 Young Soo Lee,2 Seung Pyo Hong,2 and Sung Hee Mun3 1Department of Cardiology, Kyungpook National University Hospital, Daegu, Korea; 2Department of Cardiology, Catholic University of Daegu, Daegu, Korea; 3Department of Radiology, Catholic University of Daegu, Daegu, Korea RV LV RA LA A B C LA CS RA PVLV LA MCV MCV LV D E Fig. 1. Cardiac computed tomography demonstrates the middle cardiac vein draining into the left atrium (yellow arrows). (A-C) Axial serial scan images of cardiac computed to- mography after contrast dye injection. (D) The 3-dimensional volume rendering image of cardiac computed tomography. (E) The curved planar reformation image of cardiac computed tomography. A 67-year-old woman was admitted for radiofrequency catheter oxygen supplement. Her electrocardiogram, chest X-ray, and ablation (RFCA) of paroxysmal atrial fibrillation. She had un- echocardiogram were within normal limits. She underwent derwent patch closure of atrial septal defect 7 years before. Her cardiac computed tomography for the left atrial reconstruction arterial blood oxygen saturation level was 94.6% without any before the RFCA. It revealed abnormal drainage of the middle © 2016 The Korean Academy of Medical Sciences. pISSN 1011-8934 This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. -

The Variability of the Small Cardiac Vein in the Adult Human Heart
Folia Morphol. Vol. 63, No. 2, pp. 159–162 Copyright © 2004 Via Medica O R I G I N A L A R T I C L E ISSN 0015–5659 www.fm.viamedica.pl The variability of the small cardiac vein in the adult human heart Monika Cendrowska-Pinkosz Department of Anatomy, University Medical School, Lublin, Poland [Received 5 February 2003; Revised 25 November 2003; Accepted 31 December 2003] Direct analyses were performed on 50 hearts submitted for post mortem exam- ination. The remaining hearts were examined by the corrosion method. The aim of the work was to assess the morphology of the small cardiac vein. The small cardiac vein, which runs along the back surface of the coronary sulcus, would usually drain into the coronary sinus at its right side (86% of cases). Cases of the small cardiac vein draining into the middle cardiac vein were also noticed (12%) or directly into the right atrium (1%). In 1% of the preparations it ran along the right margin in the direction of the apex of the heart. In 30% of the corrosion preparations the small cardiac vein was not accessible with the help of corrosion. In 24% of the dissection preparations it was not possible to reach the small cardiac vein with the help of dissection. A statisti- cally significant relationship was observed between the frequency of the pres- ence or absence of the small cardiac vein and the sex of the donor (p > 0.001). In the group examined the percentage of men who did not have the small cardiac vein was 6 times higher than among the woman. -

A Case of the Bilateral Superior Venae Cavae with Some Other Anomalous Veins
Okaiimas Fol. anat. jap., 48: 413-426, 1972 A Case of the Bilateral Superior Venae Cavae With Some Other Anomalous Veins By Yasumichi Fujimoto, Hitoshi Okuda and Mihoko Yamamoto Department of Anatomy, Osaka Dental University, Osaka (Director : Prof. Y. Ohta) With 8 Figures in 2 Plates and 2 Tables -Received for Publication, July 24, 1971- A case of the so-called bilateral superior venae cavae after the persistence of the left superior vena cava has appeared relatively frequent. The present authors would like to make a report on such a persistence of the left superior vena cava, which was found in a routine dissection cadaver of their school. This case is accompanied by other anomalies on the venous system ; a complete pair of the azygos veins, the double subclavian veins of the right side and the ring-formation in the left external iliac vein. Findings Cadaver : Mediiim nourished male (Japanese), about 157 cm in stature. No other anomaly in the heart as well as in the great arteries is recognized. The extracted heart is about 350 gm in weight and about 380 ml in volume. A. Bilateral superior venae cavae 1) Right superior vena cava (figs. 1, 2, 4) It measures about 23 mm in width at origin, about 25 mm at the pericardiac end, and about 31 mm at the opening to the right atrium ; about 55 mm in length up to the pericardium and about 80 mm to the opening. The vein is formed in the usual way by the union of the right This report was announced at the forty-sixth meeting of Kinki-district of the Japanese Association of Anatomists, February, 1971,Kyoto. -
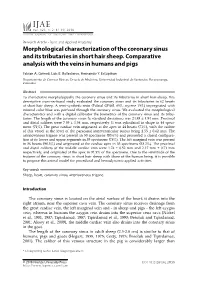
Morphological Characterization of the Coronary Sinus and Its Tributaries in Short Hair Sheep. Comparative Analysis with the Veins in Humans and Pigs
IJAE Vol. 123, n. 2: 81-90, 2018 ITALIAN JOURNAL OF ANATOMY AND EMBRYOLOGY Research Article - Basic and Applied Anatomy Morphological characterization of the coronary sinus and its tributaries in short hair sheep. Comparative analysis with the veins in humans and pigs Fabian A. Gómez, Luis E. Ballesteros, Hernando Y. Estupiñan Departamento de Ciencias Básicas, Escuela de Medicina, Universidad Industrial de Santander, Bucaramanga, Colombia Abstract To characterize morphologically the coronary sinus and its tributaries in short hair sheep, this descriptive cross-sectional study evaluated the coronary sinus and its tributaries in 62 hearts of short hair sheep. A semi-synthetic resin (Palatal GP40L 85%; styrene 15%) impregnated with mineral color blue was perfused through the coronary sinus. We evaluated the morphological characteristics and with a digital calibrator the biometrics of the coronary sinus and its tribu- taries. The length of the coronary sinus (± standard deviation) was 24.85 ± 4.94 mm. Proximal and distal calibers were 7.55 ± 1.54 mm, respectively. It was cylindrical in shape in 44 speci- mens (71%). The great cardiac vein originated at the apex in 44 hearts (71%), with the caliber of this vessel at the level of the paraconal interventricular sulcus being 2.55 ± 0.62 mm. The arteriovenous trigone was present in 50 specimens (80.6%) and presented a closed configura- tion at its lower and upper segments in 39 specimens (78%). The left marginal vein was present in 56 hearts (90.3%) and originated at the cardiac apex in 33 specimens (53.2%). The proximal and distal calibers of the middle cardiac vein were 1.74 ± 0.52 mm and 2.17 mm ± 0.71 mm respectively, and originated at the apex in 91.9% of the specimens. -

With a Closed Coronary Sinus by W
Thorax: first published as 10.1136/thx.15.2.172 on 1 June 1960. Downloaded from Thorax (1960), 15, 172. A CASE OF BILATERAL SUPERIOR VENAE CAVAE WITH A CLOSED CORONARY SINUS BY W. G. HARRIS From the Departmzent of Anatomy, University College, London (RECEIVED FOR PUBLICATION OCTOBER 7, 1959) During the routine dissection of a cadaver a inferior vena cava and pulmonary veins. No left superior vena cava was noticed passing into other congenital abnormality was found in the the coronary sinus. This condition is not heart. uncommon, but further dissection showed that the THE EMBRYOLOGY coronary sinus ended 1 cm. from the wall of the Hutton (1915) suggested two possible embryo- right atrium. Inspection of the right atrium logical causes for this abnormality: (1) Fusion showed no opening for the coronary sinus and the between the coronary segments of the left and wall between the opening for the inferior vena cava and the tricuspid orifice was smooth. A more complete dissection showed the following details of anatomy. Passing downwards from the proximal end of the left innominate vein was a left superior vena cava. It started about 2 cm. from the junction of copyright. the left internal jugular and subclavian veins, and, passing in front of the hilum of the left lung, across the back of the left atrium, it entered the left end of the coronary sinus. At this point the great cardiac vein entered the left superior vena http://thorax.bmj.com/ cava from below, and this was the point at which the left superior vena cava was assumed to become the coronary sinus. -

G06, G12, G13 (1000263, 1000268, 1000269) 2 Latin
…going one step further G06 1000263 G13 1000269 G12 1000268 G06, G12, G13 (1000263, 1000268, 1000269) 2 Latin G12, G13: A Apex cordis B Septum interventriculare, pars muscularis I Atrium dextrum Ia Auricula dextra II Atrium sinistrum IIb Auricula sinistra III Ventriculus dexter IV Ventriculus sinister 1 V. cava superior 1a V. brachiocephalica sinistra 2 V. cava inferior 3 Valva atrioventricularis dextra (Valva tricuspidalis) 3a Mm. papillares 3b Valva trunci pulmonalis 4 Truncus pulmonalis 4a A. pulmonalis sinistra 4b A. pulmonalis dextra 5 Vv. pulmonales 6 Valva atrioventricularis sinistra (Valva mitralis) 6c Mm. papillares 6d Valva aortae 7 Pars ascendens aortae ® 7a Arcus aortae 7b Truncus brachiocephalicus 7c A. carotis communis sinistra 7d A. subclavia sinistra 8 A. coronaria dextra 8a R. interventricularis posterior a. coronariae dextrae 8b R. posterolateralis dexter a. coronariae dextrae 9a R. interventricularis anterior a. coronariae sinistrae 9b R. circumflexus a. coronariae sinistrae 9c R. lateralis a. coronariae sinistrae 10 Sinus coronarius 10a V. cardiaca magna 10b V. cardiaca parva 10c V. cardiaca media (V. interventricularis posterior) 10d Vv. ventriculi sinisteri posteriores 11 Sulcus coronarius 12 Sulcus interventricularis anterior 13 Sulcus interventricularis posterior G13: 14 Trachea 15 Oesophagus 3 Heart, 2-times life size English G12, G13: A Apex of heart B Muscular part of interventricular septum I Right atrium Ia Right auricle II Left atrium IIb Left auricle III Right ventricle IV Left ventricle 1 Superior vena -

Superior Vena Cava Pulmonary Trunk Aorta Parietal Pleura (Cut) Left Lung
Superior Aorta vena cava Parietal pleura (cut) Pulmonary Left lung trunk Pericardium (cut) Apex of heart Diaphragm (a) © 2018 Pearson Education, Inc. 1 Midsternal line 2nd rib Sternum Diaphragm Point of maximal intensity (PMI) (b) © 2018 Pearson Education, Inc. 2 Mediastinum Heart Right lung (c) Posterior © 2018 Pearson Education, Inc. 3 Pulmonary Fibrous trunk pericardium Parietal layer of serous pericardium Pericardium Pericardial cavity Visceral layer of serous pericardium Epicardium Myocardium Heart wall Endocardium Heart chamber © 2018 Pearson Education, Inc. 4 Superior vena cava Aorta Left pulmonary artery Right pulmonary artery Left atrium Right atrium Left pulmonary veins Right pulmonary veins Pulmonary semilunar valve Left atrioventricular valve Fossa ovalis (bicuspid valve) Aortic semilunar valve Right atrioventricular valve (tricuspid valve) Left ventricle Right ventricle Chordae tendineae Interventricular septum Inferior vena cava Myocardium Visceral pericardium (epicardium) (b) Frontal section showing interior chambers and valves © 2018 Pearson Education, Inc. 5 Left ventricle Right ventricle Muscular interventricular septum © 2018 Pearson Education, Inc. 6 Capillary beds of lungs where gas exchange occurs Pulmonary Circuit Pulmonary arteries Pulmonary veins Venae Aorta and cavae branches Left atrium Left Right ventricle atrium Heart Right ventricle Systemic Circuit Capillary beds of all body tissues where gas exchange occurs KEY: Oxygen-rich, CO2-poor blood Oxygen-poor, CO2-rich blood © 2018 Pearson Education, Inc. 7 (a) Operation of the AV valves 1 Blood returning 4 Ventricles contract, to the atria puts forcing blood against pressure against AV valve cusps. AV valves; the AV valves are forced open. 5 AV valves close. 2 As the ventricles 6 Chordae tendineae fill, AV valve cusps tighten, preventing hang limply into valve cusps from ventricles. -
Lab 3 Heart Sounds, Valve Problems and Blood Flow
Lab 3 Heart Sounds, Valve Problems and Blood Flow MDufilho 1 Heart Sound Lub-dup, lub-dup, lub-dup • Lub – lower pitch • Dup – higher pitch • Normal heart sounds -Animated Normal S1 S2 MDufilho 2 Figure 18.20 Areas of the thoracic surface where the sounds of individual valves can best be detected. Aortic valve sounds heard in 2nd intercostal space at right sternal margin Pulmonary valve sounds heard in 2nd intercostal space at left sternal margin Mitral valve sounds heard over heart apex (in 5th intercostal space) in line with middle of clavicle Tricuspid valve sounds typically heard in right sternal margin of 5th MDufilho intercostal space 3 Figure 18.5e – Heart Valves Aorta Left pulmonary artery Superior vena cava Right pulmonary artery Left atrium Left pulmonary veins Pulmonary trunk Right atrium Mitral (bicuspid) valve Right pulmonary veins Fossa ovalis Aortic valve Pectinate muscles Pulmonary valve Tricuspid valve Right ventricle Left ventricle Chordae tendineae Papillary muscle Interventricular septum Trabeculae carneae Epicardium Inferior vena cava Myocardium Endocardium Frontal section MDufilho 4 (not in text) Valve Prolapse MDufilho 5 (not in text) Valve Prolapse MDufilho 6 (not in text) Valvular Stenosis MDufilho 7 (not in text) Valvular Stenosis Heart Sounds S3 S4 Murmurs MDufilho 8 Figure 18.5b Blood Supply to the Myocardium Left common carotid artery Brachiocephalic trunk Left subclavian artery Superior vena cava Aortic arch Ligamentum arteriosum Right pulmonary artery Left pulmonary artery Ascending aorta Left pulmonary -

CARDIOLOGY PHYSIOLOGY Part 1 Describe the Adult Coronary Circulation the Left Main and Right Coronary Arteries Originate At
CARDIOLOGY PHYSIOLOGY Part 1 Describe the adult coronary circulation The left main and right coronary arteries originate at the base of the aorta, from the coronary ostia, which is located behind the aortic leaflets. These two arteries lie on the surface of the heart whereas the smaller arteries penetrate the epicardium and supply blood to the myocardium. The left main coronary artery arises from the posterior aortic sinus above the left coronary cusp of the aortic valve and has two main branches, the circumflex and the left anterior descending artery. The circumflex artery lies in the left atrioventricular groove and supplies most of the left atrium and the posterior and lateral parts of the left ventricle. It, also with the left anterior descending artery, supplies the anterolateral papillary muscle. The circumflex artery has several branches including; atrial branches and obtuse marginal branches 1, 2 and 3. In 10% of people the circumflex supplies the posterior descending artery, this is termed ‘left dominant circulation’. Also, in 40% of the population, the circumflex supplies the sinoatrial node. The left anterior descending artery, which is also known as the anterior interventricular branch, follows the anterior interventricular sulcus down to the apex of the heart where it often anastomoses with the terminal branches of the posterior descending artery. It supplies the anterolateral portions of the heart, the anterior 2/3 of the interventricular septum. Important branches include the diagonal branches, which run laterally to supply the anterolateral wall of the LV, and the septal branches which supplies the anterior 2/3 of the interventricular septum. -

Thorax-Heart-Blood-Supply-Innervation.Pdf
Right coronary artery • Originates from the right aortic sinus of the ascending aorta. Branches: • Atrial branches sinu-atrial nodal branch, • Ventricular branches • Right marginal branch arises at the inferior margin of the heart and continues along this border toward the apex of the heart; • Posterior interventricular branch- lies in the posterior interventricular sulcus. The right coronary artery supplies • right atrium and right ventricle, • sinu-atrial and atrioventricular nodes, • the interatrial septum, • a part of the left atrium, • the posteroinferior one-third of the interventricular septum, • a part of the posterior part of the left ventricle. Left coronary artery • from the left aortic sinus of the ascending aorta. The artery divides into its two terminal branches: • Anterior interventricular branch (left anterior descending artery- LAD), descends obliquely toward the apex of the heart in the anterior interventricular sulcus, one or two large diagonal branches may arise and descend diagonally across the anterior surface of the left ventricle; • Circumflex branch, which courses in the coronary sulcus and onto the diaphragmatic surface of the heart and usually ends before reaching the posterior interventricular sulcus-a large branch, the left marginal artery, usually arises from it and continues across the rounded obtuse margin of the heart. Coronary distribution Coronary anastomosis Applied Anatomy • Myocardial infarction Occlusion of a major coronary artery leads to an inadequate oxygenation of an area of myocardium and cell death. The severity depends on: size and location of the artery Complete or partial blockage (angina) • Coronary angioplasty • Coronary artery bypass grafting Cardiac veins The coronary sinus receives four major tributaries: • Great cardiac vein begins at the apex of the heart. -

Overview of Cardiac Anatomy Relevant to Catheter Ablation
CAOC01 9/18/07 2:35 PM Page 1 I Fundamentals CAOC01 9/18/07 2:35 PM Page 3 Overview of cardiac anatomy relevant to 1 catheter ablation Siew Yen Ho Every new diagnostic technique and every new surgical for appropriate clinical correlations. He termed the orienta- or interventional procedure in the heart leads to a review tion of the heart, seen in its living condition, as “attitudinal.” of the organ’s anatomy relevant to that particular tech- Since electrophysiologists “view” the patient with the nique or procedure. Although the anatomy of the heart heart in situ, it is essential that the attitudinal approach [3] has remained unchanged, the perspectives from which should be adopted when describing the spatial relation- clinicians can approach the heart have evolved through ships of chambers and structures. The names of the cham- the ages. Catheter ablation for cardiac arrhythmias is the bers remain unaltered, although right heart chambers are relatively “new boy on the block” that has led to a new not strictly to the right nor left heart chambers strictly to perception of cardiac anatomy in the normally structured the left. as well as the congenitally malformed heart. In this chap- The heart lies in the mediastinum of the thoracic cavity, ter, I hope to provide an overview of the fundamentals in between the left and right lungs. When viewed from the anatomy of the normally structured heart, with emphasis front, the heart has a trapezoidal silhouette. Two-thirds of on features relevant to catheter ablation. Necessarily, much its bulk lies to the left of the midline of the chest, with its of the information is basic, although crucial to knowing apex directed to the left and inferiorly.