Malignant Hilar Obstruction Due to Neuroendocrine Tumor of Common Hepatic Duct – a Case Report and Short Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cholangiocarcinoma 2020: the Next Horizon in Mechanisms and Management
CONSENSUS STATEMENT Cholangiocarcinoma 2020: the next horizon in mechanisms and management Jesus M. Banales 1,2,3 ✉ , Jose J. G. Marin 2,4, Angela Lamarca 5,6, Pedro M. Rodrigues 1, Shahid A. Khan7, Lewis R. Roberts 8, Vincenzo Cardinale9, Guido Carpino 10, Jesper B. Andersen 11, Chiara Braconi 12, Diego F. Calvisi13, Maria J. Perugorria1,2, Luca Fabris 14,15, Luke Boulter 16, Rocio I. R. Macias 2,4, Eugenio Gaudio17, Domenico Alvaro18, Sergio A. Gradilone19, Mario Strazzabosco 14,15, Marco Marzioni20, Cédric Coulouarn21, Laura Fouassier 22, Chiara Raggi23, Pietro Invernizzi 24, Joachim C. Mertens25, Anja Moncsek25, Sumera Rizvi8, Julie Heimbach26, Bas Groot Koerkamp 27, Jordi Bruix2,28, Alejandro Forner 2,28, John Bridgewater 29, Juan W. Valle 5,6 and Gregory J. Gores 8 Abstract | Cholangiocarcinoma (CCA) includes a cluster of highly heterogeneous biliary malignant tumours that can arise at any point of the biliary tree. Their incidence is increasing globally, currently accounting for ~15% of all primary liver cancers and ~3% of gastrointestinal malignancies. The silent presentation of these tumours combined with their highly aggressive nature and refractoriness to chemotherapy contribute to their alarming mortality, representing ~2% of all cancer-related deaths worldwide yearly. The current diagnosis of CCA by non-invasive approaches is not accurate enough, and histological confirmation is necessary. Furthermore, the high heterogeneity of CCAs at the genomic, epigenetic and molecular levels severely compromises the efficacy of the available therapies. In the past decade, increasing efforts have been made to understand the complexity of these tumours and to develop new diagnostic tools and therapies that might help to improve patient outcomes. -

Primary Hepatic Neuroendocrine Carcinoma: Report of Two Cases and Literature Review
The Jackson Laboratory The Mouseion at the JAXlibrary Faculty Research 2018 Faculty Research 3-1-2018 Primary hepatic neuroendocrine carcinoma: report of two cases and literature review. Zi-Ming Zhao The Jackson Laboratory, [email protected] Jin Wang Ugochukwu C Ugwuowo Liming Wang Jeffrey P Townsend Follow this and additional works at: https://mouseion.jax.org/stfb2018 Part of the Life Sciences Commons, and the Medicine and Health Sciences Commons Recommended Citation Zhao, Zi-Ming; Wang, Jin; Ugwuowo, Ugochukwu C; Wang, Liming; and Townsend, Jeffrey P, "Primary hepatic neuroendocrine carcinoma: report of two cases and literature review." (2018). Faculty Research 2018. 71. https://mouseion.jax.org/stfb2018/71 This Article is brought to you for free and open access by the Faculty Research at The ousM eion at the JAXlibrary. It has been accepted for inclusion in Faculty Research 2018 by an authorized administrator of The ousM eion at the JAXlibrary. For more information, please contact [email protected]. Zhao et al. BMC Clinical Pathology (2018) 18:3 https://doi.org/10.1186/s12907-018-0070-7 CASE REPORT Open Access Primary hepatic neuroendocrine carcinoma: report of two cases and literature review Zi-Ming Zhao1,2*† , Jin Wang3,4,5†, Ugochukwu C. Ugwuowo6, Liming Wang4,8* and Jeffrey P. Townsend2,7* Abstract Background: Primary hepatic neuroendocrine carcinoma (PHNEC) is extremely rare. The diagnosis of PHNEC remains challenging—partly due to its rarity, and partly due to its lack of unique clinical features. Available treatment options for PHNEC include surgical resection of the liver tumor(s), radiotherapy, liver transplant, transcatheter arterial chemoembolization (TACE), and administration of somatostatin analogues. -

What Is a Gastrointestinal Carcinoid Tumor?
cancer.org | 1.800.227.2345 About Gastrointestinal Carcinoid Tumors Overview and Types If you have been diagnosed with a gastrointestinal carcinoid tumor or are worried about it, you likely have a lot of questions. Learning some basics is a good place to start. ● What Is a Gastrointestinal Carcinoid Tumor? Research and Statistics See the latest estimates for new cases of gastrointestinal carcinoid tumor in the US and what research is currently being done. ● Key Statistics About Gastrointestinal Carcinoid Tumors ● What’s New in Gastrointestinal Carcinoid Tumor Research? What Is a Gastrointestinal Carcinoid Tumor? Gastrointestinal carcinoid tumors are a type of cancer that forms in the lining of the gastrointestinal (GI) tract. Cancer starts when cells begin to grow out of control. To learn more about what cancer is and how it can grow and spread, see What Is Cancer?1 1 ____________________________________________________________________________________American Cancer Society cancer.org | 1.800.227.2345 To understand gastrointestinal carcinoid tumors, it helps to know about the gastrointestinal system, as well as the neuroendocrine system. The gastrointestinal system The gastrointestinal (GI) system, also known as the digestive system, processes food for energy and rids the body of solid waste. After food is chewed and swallowed, it enters the esophagus. This tube carries food through the neck and chest to the stomach. The esophagus joins the stomachjust beneath the diaphragm (the breathing muscle under the lungs). The stomach is a sac that holds food and begins the digestive process by secreting gastric juice. The food and gastric juices are mixed into a thick fluid, which then empties into the small intestine. -

Primary Hepatic Carcinoid Tumor with Poor Outcome Om Parkash Aga Khan University, [email protected]
eCommons@AKU Section of Gastroenterology Department of Medicine March 2016 Primary Hepatic Carcinoid Tumor with Poor Outcome Om Parkash Aga Khan University, [email protected] Adil Ayub Buria Naeem Sehrish Najam Zubair Ahmed Aga Khan University See next page for additional authors Follow this and additional works at: https://ecommons.aku.edu/ pakistan_fhs_mc_med_gastroenterol Part of the Gastroenterology Commons Recommended Citation Parkash, O., Ayub, A., Naeem, B., Najam, S., Ahmed, Z., Jafri, W., Hamid, S. (2016). Primary Hepatic Carcinoid Tumor with Poor Outcome. Journal of the College of Physicians and Surgeons Pakistan, 26(3), 227-229. Available at: https://ecommons.aku.edu/pakistan_fhs_mc_med_gastroenterol/220 Authors Om Parkash, Adil Ayub, Buria Naeem, Sehrish Najam, Zubair Ahmed, Wasim Jafri, and Saeed Hamid This report is available at eCommons@AKU: https://ecommons.aku.edu/pakistan_fhs_mc_med_gastroenterol/220 CASE REPORT Primary Hepatic Carcinoid Tumor with Poor Outcome Om Parkash1, Adil Ayub2, Buria Naeem2, Sehrish Najam2, Zubair Ahmed, Wasim Jafri1 and Saeed Hamid1 ABSTRACT Primary Hepatic Carcinoid Tumor (PHCT) represents an extremely rare clinical entity with only a few cases reported to date. These tumors are rarely associated with metastasis and surgical resection is usually curative. Herein, we report two cases of PHCT associated with poor outcomes due to late diagnosis. Both cases presented late with non-specific symptoms. One patient presented after a 2-week history of symptoms and the second case had a longstanding two years symptomatic interval during which he remained undiagnosed and not properly worked up. Both these cases were diagnosed with hepatic carcinoid tumor, which originates from neuroendocrine cells. Case 1 opted for palliative care and expired in one month’s time. -

Liver, Gallbladder, Bile Ducts, Pancreas
Liver, gallbladder, bile ducts, pancreas Coding issues Otto Visser May 2021 Anatomy Liver, gallbladder and the proximal bile ducts Incidence of liver cancer in Europe in 2018 males females Relative survival of liver cancer (2000 10% 15% 20% 25% 30% 35% 40% 45% 50% 0% 5% Bulgaria Latvia Estonia Czechia Slovakia Malta Denmark Croatia Lithuania N Ireland Slovenia Wales Poland England Norway Scotland Sweden Netherlands Finland Iceland Ireland Austria Portugal EUROPE - Germany 2007) Spain Switzerland France Belgium Italy five year one year Liver: topography • C22.1 = intrahepatic bile ducts • C22.0 = liver, NOS Liver: morphology • Hepatocellular carcinoma=HCC (8170; C22.0) • Intrahepatic cholangiocarcinoma=ICC (8160; C22.1) • Mixed HCC/ICC (8180; TNM: C22.1; ICD-O: C22.0) • Hepatoblastoma (8970; C22.0) • Malignant rhabdoid tumour (8963; (C22.0) • Sarcoma (C22.0) • Angiosarcoma (9120) • Epithelioid haemangioendothelioma (9133) • Embryonal sarcoma (8991)/rhabdomyosarcoma (8900-8920) Morphology*: distribution by sex (NL 2011-17) other other ICC 2% 3% 28% ICC 56% HCC 41% HCC 70% males females * Only pathologically confirmed cases Liver cancer: primary or metastatic? Be aware that other and unspecified morphologies are likely to be metastatic, unless there is evidence of the contrary. For example, primary neuro-endocrine tumours (including small cell carcinoma) of the liver are extremely rare. So, when you have a diagnosis of a carcinoid or small cell carcinoma in the liver, this is probably a metastatic tumour. Anatomy of the bile ducts Gallbladder -
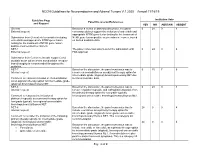
NCCN Guidelines for Neuroendocrine and Adrenal Tumors V.1.2020 – Annual 11/18/19
NCCN Guidelines for Neuroendocrine and Adrenal Tumors V.1.2020 – Annual 11/18/19 Guideline Page Institution Vote Panel Discussion/References and Request YES NO ABSTAIN ABSENT General Based on a review of data and discussion, the panel 0 24 0 4 External request: consensus did not support the inclusion of entrectinib and appropriate NTRK gene fusion testing for the treatment of Submission from Genentech to consider including NTRK gene fusion-positive neuroendocrine cancer, based entrectinib and appropriate NTRK gene fusion on limited available data. testing for the treatment of NTRK gene fusion- positive neuroendocrine cancers. NET-1 The panel consensus was to defer the submission until 0 24 0 4 External request: FDA approval. Submission from Curium to include copper Cu 64 dotatate as an option where somatostatin receptor- based imaging is recommended throughout the guideline. NET-7 Based on the discussion, the panel consensus was to 0 15 7 6 Internal request: remove chemoradiation as an adjuvant therapy option for intermediate grade (atypical) bronchopulmonary NET due Comment to reassess inclusion of chemoradiation to limited available data. as an adjuvant therapy option for intermediate grade (atypical) bronchopulmonary NET. NET-8 Based on the discussion, the panel consensus was to 0 24 0 4 Internal request: remove cisplatin/etoposide and carboplatin/etoposide from the primary therapy option for low grade (typical), Comment to reassess the inclusion of locoregional unresectable bronchopulmonary/thymus NET. platinum/etoposide as a primary therapy option for low grade (typical), locoregional unresectable bronchopulmonary/thymus NET. NET-8 Based on the discussion, the panel consensus was to 24 0 0 4 Internal request: include everolimus as a primary therapy option for intermediate grade (atypical), locoregional unresectable Comment to consider the inclusion of the following bronchopulmonary/thymus NET. -

Slug Overexpression Is Associated with Poor Prognosis in Thymoma Patients
306 ONCOLOGY LETTERS 11: 306-310, 2016 Slug overexpression is associated with poor prognosis in thymoma patients TIANQIANG ZHANG, XU CHEN, XIUMEI CHU, YI SHEN, WENJIE JIAO, YUCHENG WEI, TONG QIU, GUANZHONG YAN, XIAOFEI WANG and LINHAO XU Department of Thoracic Surgery, The Affiliated Hospital, Qingdao University, Qingdao, Shandong 266003, P.R. China Received November 4, 2014; Accepted May 22, 2015 DOI: 10.3892/ol.2015.3851 Abstract. Slug, a member of the Snail family of transcriptional previously been regarded as a benign disease, but more recent factors, is a newly identified suppressive transcriptional factor evidence indicated that it is a potentially malignant tumor of E‑cadherin. The present study investigated the expression requiring prolonged follow‑up (4). However, biomarkers for pattern of Slug in thymomas to evaluate its clinical significance. thymoma diagnosis and prognosis have not yet been estab- Immunohistochemistry was used to investigate the expression lished. pattern of the Slug protein in archived tissue sections from Slug is a member of the Snail family of zinc‑finger tran- 100 thymoma and 60 histologically normal thymus tissue scription factors and was first identified in the neural crest and samples. The associations between Slug expression and developing mesoderm of chicken embryos (5). Slug induces the clinicopathological factors, such as prognosis, were analyzed. downregulation of E-cadherin, an adhesion molecule, leading Positive expression of Slug was detected in a greater propor- to the breakdown of cell-cell adhesions and the acquisition of tion of thymoma samples [51/100 (51%) patients, P<0.001] invasive growth properties in cancer cells (6). These changes compared with normal thymus tissues [9/60 (15%) cases]. -

Cholangiocarcinoma Associated With
Schmidt et al. Journal of Medical Case Reports (2016) 10:200 DOI 10.1186/s13256-016-0989-1 CASE REPORT Open Access Cholangiocarcinoma associated with limbic encephalitis and early cerebral abnormalities detected by 2-deoxy-2- [fluorine-18]fluoro-D-glucose integrated with computed tomography-positron emission tomography: a case report Sergio L. Schmidt1,2,3*, Juliana J. Schmidt1,2, Julio C. Tolentino2, Carlos G. Ferreira4,5, Sergio A. de Almeida6, Regina P. Alvarenga2, Eunice N. Simoes2, Guilherme J. Schmidt2, Nathalie H. S. Canedo7 and Leila Chimelli7 Abstract Background: Limbic encephalitis was originally described as a rare clinical neuropathological entity involving seizures and neuropsychological disturbances. In this report, we describe cerebral patterns visualized by positron emission tomography in a patient with limbic encephalitis and cholangiocarcinoma. To our knowledge, there is no other description in the literature of cerebral positron emission tomography findings in the setting of limbic encephalitis and subsequent diagnosis of cholangiocarcinoma. Case presentation: We describe a case of a 77-year-old Caucasian man who exhibited persistent cognitive changes 2 years before his death. A cerebral scan obtained at that time by 2-deoxy-2-[fluorine-18]fluoro-D-glucose integrated with computed tomography-positron emission tomography showed low radiotracer uptake in the frontal and temporal lobes. Cerebrospinal fluid analysis indicated the presence of voltage-gated potassium channel antibodies. Three months before the patient’s death, a lymph node biopsy indicated a cholangiocarcinoma, and a new cerebral scan obtained by 2-deoxy-2-[fluorine-18]fluoro-D-glucose integrated with computed tomography- positron emission tomography showed an increment in the severity of metabolic deficit in the frontal and parietal lobes, as well as hypometabolism involving the temporal lobes. -

Rising Incidence of Neuroendocrine Tumors
Rising Incidence of Neuroendocrine Tumors Dasari V, Yao J, et al. JAMA Oncology 2017 S L I D E 1 Overview Pancreatic Neuroendocrine Tumors • Tumors which arise from endocrine cells of the pancreas • 5.6 cases per million – 3% of pancreatic tumors • Median age at diagnosis 60 years • More indolent course compared to adenocarcinoma – 10-year overall survival 40% • Usually sporadic but can be associated with hereditary syndromes – Core genetic pathways altered in sporadic cases • DNA damage repair (MUTYH) Chromatin remodeling (MEN1) • Telomere maintenance (MEN1, DAXX, ATRX) mTOR signaling – Hereditary: 17% of patients with germline mutation Li X, Wang C, et al. Cancer Med 2018 Scarpa A, Grimond S, et al. NatureS L I2017 D E 2 Pathology Classification European American Joint World Health Organization Neuroendocrine Committee on Cancer (WHO) Tumor Society (AJCC) (ENETS) Grade Ki-67 Mitotic rt TNM TNM T1: limit to pancreas, <2 cm T1: limit to pancreas, ≦2 cm T2: limit to pancreas, 2-4 cm T2: >limit to pancreas, 2 cm T3: limit to pancreas, >4 cm, T3: beyond pancreas, no celiac or Low ≤2% <2 invades duodenum, bile duct SMA T4: beyond pancreas, invasion involvement adjacent organs or vessels T4: involves celiac or SMA N0: node negative No: node negative Intermed 3-20% 2-20 N1: node positive N1: node positive M0: no metastases M0: no metastases High >20% >20 M1: metastases M1: metastases S L I D E 3 Classification Based on Functionality • Nonfunctioning tumors – No clinical symptoms (can still produce hormone) – Accounts for 40% of tumors – 60-85% -

Primary Neuroendocrine Neoplasms of the Kidney, a Distinct Entity but Classifiable- Like the Gastroenteropancreatic Neuroendocrine Neoplasms
C-60 Primary Neuroendocrine Neoplasms of the Kidney, A Distinct Entity but Classifiable- Like the Gastroenteropancreatic Neuroendocrine Neoplasms Manik Amin1; Deyali Chatterjee2 1Washington University in St Louis; 2Washington University School of Medicine BACKGROUND: Primary neuroendocrine neoplasms of the kidney are a distinct and rare entity, but classifiable-like the gastroenteropancreatic neuroendocrine neoplasms. Due to rarity of these tumors, not much is known about histopathology and behaviors of these tumors. We attempted to review pathology of primary kidney neuroendocrine tumor patients at our institution. METHODS: Retrospective chart review identified 8 primary kidney neuroendocrine tumors from Siteman Cancer Registry database from 1/1/2000 until 1/1/2018. Pathology review was done for all the patients to confirm their diagnosis and other pathological features. RESULTS: In our cohort, we identified eight cases of neuroendocrine neoplasms of the kidney. Three of the cases were poorly differentiated neuroendocrine carcinoma. All cases of well-differentiated neuroendocrine tumor (either grade 1 or grade 2) were identified in females (age range 44 – 60). All the tumors characteristically extended to the perirenal fat. These tumors showed diffuse positivity for synaptophysin, variable positivity for chromogranin, and did not stain for markers specific for renal differentiation (PAX-8). The growth pattern in well differentiated neuroendocrine tumors is predominantly trabeculated, but a diffuse plasmacytoid growth is also noted, which is unusual in gastroenteropancreatic neuroendocrine neoplasms. Two patients had Primary tumor measuring 9 cm and 14 cm respectively also presented with positive lymph nodes and lymphovascular invasion developed metastatic disease in 2 years. NANETS 2019 Symposium Abstracts | 175 CONCLUSION: Primary kidney neuroendocrine tumors are very rare. -

Solitary Duodenal Metastasis from Renal Cell Carcinoma with Metachronous Pancreatic Neuroendocrine Tumor: Review of Literature with a Case Discussion
Published online: 2021-05-24 Practitioner Section Solitary Duodenal Metastasis from Renal Cell Carcinoma with Metachronous Pancreatic Neuroendocrine Tumor: Review of Literature with a Case Discussion Abstract Saphalta Baghmar, Renal cell cancinoma (RCC) is a unique malignancy with features of late recurrences, metastasis S M Shasthry1, to any organ, and frequent association with second malignancy. It most commonly metastasizes Rajesh Singla, to the lungs, bones, liver, renal fossa, and brain although metastases can occur anywhere. RCC 2 metastatic to the duodenum is especially rare, with only few cases reported in the literature. Herein, Yashwant Patidar , 3 we review literature of all the reported cases of solitary duodenal metastasis from RCC and cases Chhagan B Bihari , of neuroendocrine tumor (NET) as synchronous/metachronous malignancy with RCC. Along with S K Sarin1 this, we have described a unique case of an 84‑year‑old man who had recurrence of RCC as solitary Departments of Medical duodenal metastasis after 37 years of radical nephrectomy and metachronous pancreatic NET. Oncology, 1Hepatology, 2Radiology and 3Pathology, Keywords: Late recurrence, pancreatic neuroendocrine tumor, renal cell carcinoma, second Institute of Liver and Biliary malignancy, solitary duodenal metastasis Sciences, New Delhi, India Introduction Case Presentation Renal cell carcinoma (RCC) is unique An 84‑year‑old man with a medical history to have many unusual features such as notable for hypertension and RCC, 37 years metastasis to almost every organ in the body, postright radical nephrectomy status, late recurrences, and frequent association presented to his primary care physician with second malignancy. The most common with fatigue. When found to be anemic, sites of metastasis are the lung, lymph he was treated with iron supplementation nodes, liver, bone, adrenal glands, kidney, and blood transfusions. -

Biliary Tract Cancer*
Biliary Tract Cancer* What is Biliary Tract Cancer*? Let us answer some of your questions. * Cholangiocarcinoma (bile duct cancer) * Gallbladder cancer * Ampullary cancer ESMO Patient Guide Series based on the ESMO Clinical Practice Guidelines esmo.org Biliary tract cancer Biliary tract cancer* An ESMO guide for patients Patient information based on ESMO Clinical Practice Guidelines This guide has been prepared to help you, as well as your friends, family and caregivers, better understand biliary tract cancer and its treatment. It contains information on the causes of the disease and how it is diagnosed, up-to- date guidance on the types of treatments that may be available and any possible side effects of treatment. The medical information described in this document is based on the ESMO Clinical Practice Guideline for biliary tract cancer, which is designed to help clinicians with the diagnosis and management of biliary tract cancer. All ESMO Clinical Practice Guidelines are prepared and reviewed by leading experts using evidence gained from the latest clinical trials, research and expert opinion. The information included in this guide is not intended as a replacement for your doctor’s advice. Your doctor knows your full medical history and will help guide you regarding the best treatment for you. *Cholangiocarcinoma (bile duct cancer), gallbladder cancer and ampullary cancer. Words highlighted in colour are defined in the glossary at the end of the document. This guide has been developed and reviewed by: Representatives of the European