Cholangiocarcinoma Associated With
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cholangiocarcinoma 2020: the Next Horizon in Mechanisms and Management
CONSENSUS STATEMENT Cholangiocarcinoma 2020: the next horizon in mechanisms and management Jesus M. Banales 1,2,3 ✉ , Jose J. G. Marin 2,4, Angela Lamarca 5,6, Pedro M. Rodrigues 1, Shahid A. Khan7, Lewis R. Roberts 8, Vincenzo Cardinale9, Guido Carpino 10, Jesper B. Andersen 11, Chiara Braconi 12, Diego F. Calvisi13, Maria J. Perugorria1,2, Luca Fabris 14,15, Luke Boulter 16, Rocio I. R. Macias 2,4, Eugenio Gaudio17, Domenico Alvaro18, Sergio A. Gradilone19, Mario Strazzabosco 14,15, Marco Marzioni20, Cédric Coulouarn21, Laura Fouassier 22, Chiara Raggi23, Pietro Invernizzi 24, Joachim C. Mertens25, Anja Moncsek25, Sumera Rizvi8, Julie Heimbach26, Bas Groot Koerkamp 27, Jordi Bruix2,28, Alejandro Forner 2,28, John Bridgewater 29, Juan W. Valle 5,6 and Gregory J. Gores 8 Abstract | Cholangiocarcinoma (CCA) includes a cluster of highly heterogeneous biliary malignant tumours that can arise at any point of the biliary tree. Their incidence is increasing globally, currently accounting for ~15% of all primary liver cancers and ~3% of gastrointestinal malignancies. The silent presentation of these tumours combined with their highly aggressive nature and refractoriness to chemotherapy contribute to their alarming mortality, representing ~2% of all cancer-related deaths worldwide yearly. The current diagnosis of CCA by non-invasive approaches is not accurate enough, and histological confirmation is necessary. Furthermore, the high heterogeneity of CCAs at the genomic, epigenetic and molecular levels severely compromises the efficacy of the available therapies. In the past decade, increasing efforts have been made to understand the complexity of these tumours and to develop new diagnostic tools and therapies that might help to improve patient outcomes. -

Rare APC Promoter 1B Variants in Gastric Cancer Kindreds Unselected
PostScript with familial adenomatous polyposis.3 However, the prevalence of APC promoter Gut: first published as 10.1136/gutjnl-2020-321990 on 7 September 2020. Downloaded from variants in molecularly undiagnosed GC kindreds unselected for fundic gland polyp- osis is unknown. To investigate the contribution of APC promoter variants to GC predisposition in families lacking causal germline vari- ants CDH1, which account for 19%–40% of HDGC, we performed multigene sequencing in 259 individuals from 254 families ascertained on the basis of personal and/or family history of GC (table 1). This included 174 individuals meeting Inter- national Gastric Cancer Linkage Consor- tium criteria for HDGC and one meeting criteria for FIGC.4 The majority (76.8%) of individuals had a personal history of GC, with 85.4% diffuse GC and median age of diagnosis of 42 years (range 9–87). Six additional individuals were potential obli- gate carriers for GC predisposition. The APC promoter 1B was analysed by next- Rare APC promoter 1B variants generation sequencing (n=232) or Sanger in gastric cancer kindreds sequencing (n=27) in all index cases. unselected for fundic We identified a pathogenic variant (APC gland polyposis c.-191T>C) in an obligate carrier meeting clinical criteria for HDGC (figure 1). The index case (III-8) was diagnosed with pros- Although multiple demographic, environ- tate cancer at the age of 73, following mental and genetic factors contribute to a diagnosis of GC in two children. IV-2 gastric cancer (GC) risk, familial clustering initially presented with lower abdominal occurs in around 10%–15% of cases.1 pain, distension and ascites at 37 years A strong genetic predisposition under- of age. -
C O N F E R E N C E 7 18 October 2017
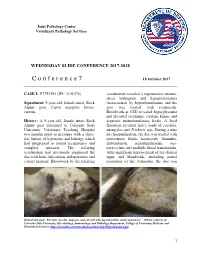
Joint Pathology Center Veterinary Pathology Services WEDNESDAY SLIDE CONFERENCE 2017-2018 C o n f e r e n c e 7 18 October 2017 CASE I: F1753191 (JPC 4101076). veterinarian revealed a regenerative anemia, stress leukogram and hypoproteinemia Signalment: 9-year-old, female intact, Rock characterized by hypoalbuminemia and the Alpine goat, Capra aegagrus hircus, goat was treated with ivermectin. caprine. Bloodwork at CSU revealed hyperglycemia and elevated creatinine, creatine kinase and History: A 9-year-old, female intact Rock aspartate aminotransferase levels. A fecal Alpine goat presented to Colorado State floatation revealed heavy loads of coccidia, University Veterinary Teaching Hospital strongyles and Trichuris spp. During a nine two months prior to necropsy with a three- day hospitalization, the doe was treated with day history of hyporexia and lethargy which intravenous fluids, kaopectate, thiamine, had progressed to lateral recumbency and fenbendazole, sulfadimethoxine, oxy- complete anorexia. The referring tetracycline and multiple blood transfusions. veterinarian had previously diagnosed the After significant improvement of her clinical doe with louse infestation, endoparasites and signs and bloodwork, including partial a heart murmur. Bloodwork by the referring resolution of the dermatitis, the doe was Haired skin goat. The skin was dry, alopecia, and covered with hyperkeratotic crusts and ulcers. (Photo courtesy of: Colorado State University, Microbiology, Immunology, and Pathology Department, College of Veterinary Medicine and Biomedical Sciences, http://csucvmbs.colostate.edu/academics/mip/Pages/default.aspx) 1 discharged. exfoliating epithelial crusts which were often tangled within scant remaining hairs. Two months later, the goat presented with a This lesion most severely affected the skin one month history of progressive scaling and over the epaxials, the ventral abdomen and ulceration over the withers, dew claws, and teats, coronary bands and dew claws. -

The Future: Surgical Advances in MEN1 Therapeutic Approaches And
2410 S M Sadowski et al. Advances in surgical 24:10 T243–T260 Thematic Review management of MEN1 The future: surgical advances in MEN1 therapeutic approaches and management strategies S M Sadowski1, G Cadiot2, E Dansin3, P Goudet4 and F Triponez1 1Thoracic and Endocrine Surgery and Faculty of Medicine, University Hospitals of Geneva, Geneva, Switzerland 2Gastroenterology and Hepatology, University Hospital of Reims, Reims, France 3 Oncology, Oscar Lambret Cancer Center, University of Lille, Lille, France Correspondence 4 Endocrine Surgery, University Hospital of Dijon, and INSERM, U866, Epidemiology and Clinical Research in Digestive should be addressed Oncology Team, and INSERM, CIC1432, Clinical Epidemiology Unit, University Hospital of Dijon, Clinical Investigation to F Triponez Centre, Clinical Epidemiology/Clinical Trials Unit, Dijon, France Email [email protected] Abstract Multiple endocrine neoplasia type 1 (MEN1) is a hereditary autosomal dominant Key Words disorder associated with numerous neuroendocrine tumors (NETs). Recent advances in f multiple endocrine the management of MEN1 have led to a decrease in mortality due to excess hormones; neoplasia type 1 (MEN1) however, they have also led to an increase in mortality from malignancy, particularly f neuro-endocrine tumors (NET) NETs. The main challenges are to localize these tumors, to select those that need f thymic NET therapy because of the risk of aggressive behavior and to select the appropriate therapy f pancreatico-gastro-intestinal associated with minimal morbidity. This must be applied to a hereditary disease with a NET Endocrine-Related Cancer Endocrine-Related high risk of recurrence. The overall aim of management in MEN1 is to ensure that the f lung NET patient remains disease- and symptom-free for as long as possible and maintains a good quality of life. -

Primary Hepatic Carcinoid Tumor with Poor Outcome Om Parkash Aga Khan University, [email protected]
eCommons@AKU Section of Gastroenterology Department of Medicine March 2016 Primary Hepatic Carcinoid Tumor with Poor Outcome Om Parkash Aga Khan University, [email protected] Adil Ayub Buria Naeem Sehrish Najam Zubair Ahmed Aga Khan University See next page for additional authors Follow this and additional works at: https://ecommons.aku.edu/ pakistan_fhs_mc_med_gastroenterol Part of the Gastroenterology Commons Recommended Citation Parkash, O., Ayub, A., Naeem, B., Najam, S., Ahmed, Z., Jafri, W., Hamid, S. (2016). Primary Hepatic Carcinoid Tumor with Poor Outcome. Journal of the College of Physicians and Surgeons Pakistan, 26(3), 227-229. Available at: https://ecommons.aku.edu/pakistan_fhs_mc_med_gastroenterol/220 Authors Om Parkash, Adil Ayub, Buria Naeem, Sehrish Najam, Zubair Ahmed, Wasim Jafri, and Saeed Hamid This report is available at eCommons@AKU: https://ecommons.aku.edu/pakistan_fhs_mc_med_gastroenterol/220 CASE REPORT Primary Hepatic Carcinoid Tumor with Poor Outcome Om Parkash1, Adil Ayub2, Buria Naeem2, Sehrish Najam2, Zubair Ahmed, Wasim Jafri1 and Saeed Hamid1 ABSTRACT Primary Hepatic Carcinoid Tumor (PHCT) represents an extremely rare clinical entity with only a few cases reported to date. These tumors are rarely associated with metastasis and surgical resection is usually curative. Herein, we report two cases of PHCT associated with poor outcomes due to late diagnosis. Both cases presented late with non-specific symptoms. One patient presented after a 2-week history of symptoms and the second case had a longstanding two years symptomatic interval during which he remained undiagnosed and not properly worked up. Both these cases were diagnosed with hepatic carcinoid tumor, which originates from neuroendocrine cells. Case 1 opted for palliative care and expired in one month’s time. -

Liver, Gallbladder, Bile Ducts, Pancreas
Liver, gallbladder, bile ducts, pancreas Coding issues Otto Visser May 2021 Anatomy Liver, gallbladder and the proximal bile ducts Incidence of liver cancer in Europe in 2018 males females Relative survival of liver cancer (2000 10% 15% 20% 25% 30% 35% 40% 45% 50% 0% 5% Bulgaria Latvia Estonia Czechia Slovakia Malta Denmark Croatia Lithuania N Ireland Slovenia Wales Poland England Norway Scotland Sweden Netherlands Finland Iceland Ireland Austria Portugal EUROPE - Germany 2007) Spain Switzerland France Belgium Italy five year one year Liver: topography • C22.1 = intrahepatic bile ducts • C22.0 = liver, NOS Liver: morphology • Hepatocellular carcinoma=HCC (8170; C22.0) • Intrahepatic cholangiocarcinoma=ICC (8160; C22.1) • Mixed HCC/ICC (8180; TNM: C22.1; ICD-O: C22.0) • Hepatoblastoma (8970; C22.0) • Malignant rhabdoid tumour (8963; (C22.0) • Sarcoma (C22.0) • Angiosarcoma (9120) • Epithelioid haemangioendothelioma (9133) • Embryonal sarcoma (8991)/rhabdomyosarcoma (8900-8920) Morphology*: distribution by sex (NL 2011-17) other other ICC 2% 3% 28% ICC 56% HCC 41% HCC 70% males females * Only pathologically confirmed cases Liver cancer: primary or metastatic? Be aware that other and unspecified morphologies are likely to be metastatic, unless there is evidence of the contrary. For example, primary neuro-endocrine tumours (including small cell carcinoma) of the liver are extremely rare. So, when you have a diagnosis of a carcinoid or small cell carcinoma in the liver, this is probably a metastatic tumour. Anatomy of the bile ducts Gallbladder -

Carcinoid Tumour of the Thymus Gland: Report of a Case
Thorax: first published as 10.1136/thx.30.4.470 on 1 August 1975. Downloaded from Thorax (1975), 30, 470. Carcinoid tumour of the thymus gland: report of a case J. PRESTON HUGHES', NELSON ANCALMO', GEORGE L. LEONARD2, and JOHN L. OCHSNER' Departments of Surgery1 and Pathology2, Alton Ochsner Medical Foundation, New Orleans, Louisiana, USA Preston Hughes, J., Ancalmo, N., Leonard, G. L., and Ochsner, J. L. (1975). Thorax, 30, 470-475. Carcinoid tumour of the thymus gland: report of a case. Carcinoid of the thymus is a rare problem. A case is reported to add to only 16 previously reported. None of these 17 patients had the carcinoid syndrome. Complete surgical excision, if possible, is the treatment of choice. A primary carcinoid tumour of the thymus is and a large anterior mediastinal tumour was re- very rare. Rosai and Higa (1972) collected eight sected through a median sternotomy. The involved cases and found only eight additional cases in the pericardium and left phrenic nerve were excised literature. A patient with this unusual lesion was with the large discrete mass. Grossly, the tumour treated at Ochsner Foundation Hospital and the measured 12X9X7 cm and weighed 290 g (Fig. case report is presented, emphasizing the import- 3). It was well-circumscribed, oval, and apparentlycopyright. ance of complete excision. encapsulated; the cut surface was homogeneous, smooth, firm, grey-white, and fleshy. Micro- CASE REPORT scopically the tumour was composed of small, A 32-year-old white man visited the emergency closely packed cells with nuclei that were uniform in http://thorax.bmj.com/ room on 16 February 1974, because of severe size and shape with few mitotic figures (Figs upper back and chest pain. -

Immunohistochemical Differential Diagnosis Between Thymic Carcinoma and Type B3 Thymoma: Diagnostic Utility of Hypoxic Marker, GLUT-1, in Thymic Epithelial Neoplasms
Modern Pathology (2009) 22, 1341–1350 & 2009 USCAP, Inc. All rights reserved 0893-3952/09 $32.00 1341 Immunohistochemical differential diagnosis between thymic carcinoma and type B3 thymoma: diagnostic utility of hypoxic marker, GLUT-1, in thymic epithelial neoplasms Masakazu Kojika1,2, Genichiro Ishii1, Junji Yoshida2, Mituyo Nishimura2, Tomoyuki Hishida2, Shu-ji Ota1, Yukinori Murata1, Kanji Nagai2 and Atsushi Ochiai1 1Pathology Division, Research Center for Innovative Oncology, National Cancer Center Hospital East, Kashiwa, Chiba, Japan and 2Thoracic Surgery Division, National Cancer Center Hospital East, Kashiwa, Chiba, Japan There are only a few immunohistochemical markers that are useful for differentiating thymic carcinomas from type B3 thymomas. The purpose of this study is to examine the additional markers that would be useful for differentiating between thymic carcinoma and thymoma type B3. We performed a tissue microarray analysis of surgically resected thymic tumor specimens from12 cases of thymic carcinoma, 7 cases of type B3 thymoma, and 68 cases of other types of thymoma. Immunostaining using 49 antibodies was scored based on staining intensity and the percentage of cells that stained positive. Seven proteins that were selected by the staining scores, namely, GLUT-1 (167 vs 4), CA-IX (110 vs 15), c-kit (162 vs 44), CD5 (33 vs 0), MUC-1 (54 vs 0), CEA (42 vs 0), and CK18 (110 vs 42), were significantly higher in the thymic carcinomas than in the type B3 thymomas. The staining sensitivity and specificity of the antibodies for thymic carcinoma were GLUT-1, sensitivity 72% and specificity 100%; CA-IX, 58 and 71%; c-kit, 72 and 85%; CD5, 33 and 100%; CK18, 58 and 71%; MUC-1, 25 and 100%; and CEA, 33 and 100%. -

Slug Overexpression Is Associated with Poor Prognosis in Thymoma Patients
306 ONCOLOGY LETTERS 11: 306-310, 2016 Slug overexpression is associated with poor prognosis in thymoma patients TIANQIANG ZHANG, XU CHEN, XIUMEI CHU, YI SHEN, WENJIE JIAO, YUCHENG WEI, TONG QIU, GUANZHONG YAN, XIAOFEI WANG and LINHAO XU Department of Thoracic Surgery, The Affiliated Hospital, Qingdao University, Qingdao, Shandong 266003, P.R. China Received November 4, 2014; Accepted May 22, 2015 DOI: 10.3892/ol.2015.3851 Abstract. Slug, a member of the Snail family of transcriptional previously been regarded as a benign disease, but more recent factors, is a newly identified suppressive transcriptional factor evidence indicated that it is a potentially malignant tumor of E‑cadherin. The present study investigated the expression requiring prolonged follow‑up (4). However, biomarkers for pattern of Slug in thymomas to evaluate its clinical significance. thymoma diagnosis and prognosis have not yet been estab- Immunohistochemistry was used to investigate the expression lished. pattern of the Slug protein in archived tissue sections from Slug is a member of the Snail family of zinc‑finger tran- 100 thymoma and 60 histologically normal thymus tissue scription factors and was first identified in the neural crest and samples. The associations between Slug expression and developing mesoderm of chicken embryos (5). Slug induces the clinicopathological factors, such as prognosis, were analyzed. downregulation of E-cadherin, an adhesion molecule, leading Positive expression of Slug was detected in a greater propor- to the breakdown of cell-cell adhesions and the acquisition of tion of thymoma samples [51/100 (51%) patients, P<0.001] invasive growth properties in cancer cells (6). These changes compared with normal thymus tissues [9/60 (15%) cases]. -

New Jersey State Cancer Registry List of Reportable Diseases and Conditions Effective Date March 10, 2011; Revised March 2019
New Jersey State Cancer Registry List of reportable diseases and conditions Effective date March 10, 2011; Revised March 2019 General Rules for Reportability (a) If a diagnosis includes any of the following words, every New Jersey health care facility, physician, dentist, other health care provider or independent clinical laboratory shall report the case to the Department in accordance with the provisions of N.J.A.C. 8:57A. Cancer; Carcinoma; Adenocarcinoma; Carcinoid tumor; Leukemia; Lymphoma; Malignant; and/or Sarcoma (b) Every New Jersey health care facility, physician, dentist, other health care provider or independent clinical laboratory shall report any case having a diagnosis listed at (g) below and which contains any of the following terms in the final diagnosis to the Department in accordance with the provisions of N.J.A.C. 8:57A. Apparent(ly); Appears; Compatible/Compatible with; Consistent with; Favors; Malignant appearing; Most likely; Presumed; Probable; Suspect(ed); Suspicious (for); and/or Typical (of) (c) Basal cell carcinomas and squamous cell carcinomas of the skin are NOT reportable, except when they are diagnosed in the labia, clitoris, vulva, prepuce, penis or scrotum. (d) Carcinoma in situ of the cervix and/or cervical squamous intraepithelial neoplasia III (CIN III) are NOT reportable. (e) Insofar as soft tissue tumors can arise in almost any body site, the primary site of the soft tissue tumor shall also be examined for any questionable neoplasm. NJSCR REPORTABILITY LIST – 2019 1 (f) If any uncertainty regarding the reporting of a particular case exists, the health care facility, physician, dentist, other health care provider or independent clinical laboratory shall contact the Department for guidance at (609) 633‐0500 or view information on the following website http://www.nj.gov/health/ces/njscr.shtml. -
(NCCN Guidelines®) Thymomas and Thymic Carcinomas
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Thymomas and Thymic Carcinomas Version 2.2019 — March 11, 2019 NCCN.org Continue Version 2.2019, 03/11/19 © 2019 National Comprehensive Cancer Network® (NCCN®), All rights reserved. NCCN Guidelines® and this illustration may not be reproduced in any form without the express written permission of NCCN. NCCN Guidelines Index NCCN Guidelines Version 2.2019 Table of Contents Thymomas and Thymic Carcinomas Discussion *David S. Ettinger, MD/Chair † Ramaswamy Govindan, MD † Sandip P. Patel, MD ‡ † Þ The Sidney Kimmel Comprehensive Siteman Cancer Center at Barnes- UC San Diego Moores Cancer Center Cancer Center at Johns Hopkins Jewish Hospital and Washingtn University School of Medicine Karen Reckamp, MD, MS † ‡ *Douglas E. Wood, MD/Vice Chair ¶ City of Hope National Medical Center Fred Hutchinson Cancer Research Matthew A. Gubens, MD, MS † Center/Seattle Cancer Care Alliance UCSF Helen Diller Family Gregory J. Riely, MD, PhD † Þ Comprehensive Cancer Center Memorial Sloan Kettering Cancer Center Dara L. Aisner, MD, PhD ≠ University of Colorado Cancer Center Mark Hennon, MD ¶ Steven E. Schild, MD § Roswell Park Cancer Institute Mayo Clinic Cancer Center Wallace Akerley, MD † Huntsman Cancer Institute Leora Horn, MD, MSc † Theresa A. Shapiro, MD, PhD Þ at the University of Utah Vanderbilt-Ingram Cancer Center The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins Jessica Bauman, MD ‡ † Rudy P. Lackner, MD ¶ Fox Chase Cancer Center Fred & Pamela Buffett Cancer Center James Stevenson, MD † Case Comprehensive Cancer Center/ Ankit Bharat, MD ¶ Michael Lanuti, MD ¶ University Hospitals Seidman Cancer Center Robert H. Lurie Comprehensive Cancer Massachusetts General Hospital Cancer Center and Cleveland Clinic Taussig Cancer Institute Center of Northwestern University Ticiana A. -

Biliary Tract Cancer*
Biliary Tract Cancer* What is Biliary Tract Cancer*? Let us answer some of your questions. * Cholangiocarcinoma (bile duct cancer) * Gallbladder cancer * Ampullary cancer ESMO Patient Guide Series based on the ESMO Clinical Practice Guidelines esmo.org Biliary tract cancer Biliary tract cancer* An ESMO guide for patients Patient information based on ESMO Clinical Practice Guidelines This guide has been prepared to help you, as well as your friends, family and caregivers, better understand biliary tract cancer and its treatment. It contains information on the causes of the disease and how it is diagnosed, up-to- date guidance on the types of treatments that may be available and any possible side effects of treatment. The medical information described in this document is based on the ESMO Clinical Practice Guideline for biliary tract cancer, which is designed to help clinicians with the diagnosis and management of biliary tract cancer. All ESMO Clinical Practice Guidelines are prepared and reviewed by leading experts using evidence gained from the latest clinical trials, research and expert opinion. The information included in this guide is not intended as a replacement for your doctor’s advice. Your doctor knows your full medical history and will help guide you regarding the best treatment for you. *Cholangiocarcinoma (bile duct cancer), gallbladder cancer and ampullary cancer. Words highlighted in colour are defined in the glossary at the end of the document. This guide has been developed and reviewed by: Representatives of the European