Exotics Oncology: Special Focus on Updates on Therapies for Rabbits & Ferrets
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Misunderstood Teenager with Paediatric Inflammatory Multisystem Syndrome – Temporarily Associated with SARS-Cov-2 Admitted Under Adult Medicine
LESSONS OF THE MONTH Clinical Medicine 2021 Vol 21, No 1: e96–9 Lessons of the month: A misunderstood teenager with paediatric inflammatory multisystem syndrome – temporarily associated with SARS-CoV-2 admitted under adult medicine Authors: Sachin T PatelA and Harry WrightB The emergence of SARS-CoV-2 has proven to be a challenge low total protein (52 g/L), albumin (28 g/L), globulin (23 g/L) and to healthcare bodies globally. The virus has been associated alkaline phosphatase (49 U/L). A surgical review was sought, and with a spectrum of clinical features, from anosmia to they recommended radiological imaging. Contrast computed gastrointestinal upset to multiorgan dysfunction in the tomography (CT) of the chest, abdomen and pelvis showed most severe cases. Given the range of features observed, it is multiple enlarged mesenteric nodes, especially in the RIF, possibly ABSTRACT important to be aware that infectious diseases can present in keeping with mesenteric adenitis (Fig 1). The visualised appendix atypically. Furthermore, in many hospitals, including our own, was unremarkable and both lung fields were clear. All other teenagers aged 16 to 18 years old are admitted under the abdominal and pelvic viscera were unremarkable. care of adult medical services. Clinicians should be aware of As appendicitis was ruled out by the surgical team, he was patients presenting with the novel condition of paediatric started on intravenous (IV) aciclovir 600 mg, 3 times a day, and IV inflammatory multisystem disorder – temporarily associated ceftriaxone 2 g, 12 hourly, to cover for meningitis. He also received with SARS-CoV-2 (PIMS-TS). -

Advancement in Diagnostic Imaging of Thymic Tumors
cancers Commentary Advancement in Diagnostic Imaging of Thymic Tumors Francesco Gentili 1,*, Ilaria Monteleone 2, Francesco Giuseppe Mazzei 1, Luca Luzzi 3, Davide Del Roscio 2, Susanna Guerrini 1 , Luca Volterrani 2 and Maria Antonietta Mazzei 2 1 Unit of Diagnostic Imaging, Department of Radiological Sciences, Azienda Ospedaliero-Universitaria Senese, 53100 Siena, Italy; [email protected] (F.G.M.); [email protected] (S.G.) 2 Unit of Diagnostic Imaging, Department of Medical, Surgical and Neuro Sciences and of Radiological Sciences, University of Siena, Azienda Ospedaliero-Universitaria Senese, 53100 Siena, Italy; [email protected] (I.M.); [email protected] (D.D.R.); [email protected] (L.V.); [email protected] (M.A.M.) 3 Thoracic Surgery Unit, Department of Medical, Surgical and Neuro Sciences, University of Siena, Azienda Ospedaliero-Universitaria Senese, 53100 Siena, Italy; [email protected] * Correspondence: [email protected] Simple Summary: Diagnostic imaging is pivotal for the diagnosis and staging of thymic tumors. It is important to distinguish thymoma and other tumor histotypes amenable to surgery from lymphoma. Furthermore, in cases of thymoma, it is necessary to differentiate between early and advanced disease before surgery since patients with locally advanced tumors require neoadjuvant chemotherapy for improving survival. This review aims to provide to radiologists a full spectrum of findings of thymic neoplasms using traditional and innovative imaging modalities. Abstract: Thymic tumors are rare neoplasms even if they are the most common primary neoplasm of the anterior mediastinum. In the era of advanced imaging modalities, such as functional MRI, dual- Citation: Gentili, F.; Monteleone, I.; Mazzei, F.G.; Luzzi, L.; Del Roscio, D.; energy CT, perfusion CT and radiomics, it is possible to improve characterization of thymic epithelial Guerrini, S.; Volterrani, L.; Mazzei, tumors and other mediastinal tumors, assessment of tumor invasion into adjacent structures and M.A. -

Rare APC Promoter 1B Variants in Gastric Cancer Kindreds Unselected
PostScript with familial adenomatous polyposis.3 However, the prevalence of APC promoter Gut: first published as 10.1136/gutjnl-2020-321990 on 7 September 2020. Downloaded from variants in molecularly undiagnosed GC kindreds unselected for fundic gland polyp- osis is unknown. To investigate the contribution of APC promoter variants to GC predisposition in families lacking causal germline vari- ants CDH1, which account for 19%–40% of HDGC, we performed multigene sequencing in 259 individuals from 254 families ascertained on the basis of personal and/or family history of GC (table 1). This included 174 individuals meeting Inter- national Gastric Cancer Linkage Consor- tium criteria for HDGC and one meeting criteria for FIGC.4 The majority (76.8%) of individuals had a personal history of GC, with 85.4% diffuse GC and median age of diagnosis of 42 years (range 9–87). Six additional individuals were potential obli- gate carriers for GC predisposition. The APC promoter 1B was analysed by next- Rare APC promoter 1B variants generation sequencing (n=232) or Sanger in gastric cancer kindreds sequencing (n=27) in all index cases. unselected for fundic We identified a pathogenic variant (APC gland polyposis c.-191T>C) in an obligate carrier meeting clinical criteria for HDGC (figure 1). The index case (III-8) was diagnosed with pros- Although multiple demographic, environ- tate cancer at the age of 73, following mental and genetic factors contribute to a diagnosis of GC in two children. IV-2 gastric cancer (GC) risk, familial clustering initially presented with lower abdominal occurs in around 10%–15% of cases.1 pain, distension and ascites at 37 years A strong genetic predisposition under- of age. -

Familial Mediterranean Fever and Periodic Fever, Aphthous Stomatitis, Pharyngitis, and Adenitis (PFAPA) Syndrome: Shared Features and Main Differences
Rheumatology International (2019) 39:29–36 Rheumatology https://doi.org/10.1007/s00296-018-4105-2 INTERNATIONAL REVIEW Familial Mediterranean fever and periodic fever, aphthous stomatitis, pharyngitis, and adenitis (PFAPA) syndrome: shared features and main differences Amra Adrovic1 · Sezgin Sahin1 · Kenan Barut1 · Ozgur Kasapcopur1 Received: 10 June 2018 / Accepted: 13 July 2018 / Published online: 17 July 2018 © Springer-Verlag GmbH Germany, part of Springer Nature 2018 Abstract Autoinflammatory diseases are characterized by fever attacks of varying durations, associated with variety of symptoms including abdominal pain, lymphadenopathy, polyserositis, arthritis, etc. Despite the diversity of the clinical presentation, there are some common features that make the differential diagnosis of the autoinflammatory diseases challenging. Familial Mediterranean fever (FMF) is the most commonly seen autoinflammatory conditions, followed by syndrome associated with periodic fever, aphthous stomatitis, pharyngitis, and adenitis (PFAPA). In this review, we aim to evaluate disease charac- teristics that make a diagnosis of FMF and PFAPA challenging, especially in a regions endemic for FMF. The ethnicity of patient, the regularity of the disease attacks, and the involvement of the upper respiratory systems and symphonies could be helpful in differential diagnosis. Current data from the literature suggest the use of biological agents as an alternative for patients with FMF and PFAPA who are non-responder classic treatment options. More controlled studies -

Copy Number Aberrations of Genes Regulating Normal Thymus Development in Thymic Epithelial Tumors
Published OnlineFirst February 26, 2013; DOI: 10.1158/1078-0432.CCR-12-3260 Clinical Cancer Human Cancer Biology Research Copy Number Aberrations of Genes Regulating Normal Thymus Development in Thymic Epithelial Tumors Iacopo Petrini1, Yisong Wang1, Paolo A. Zucali3, Hye Seung Lee1,4, Trung Pham1, Donna Voeller1, Paul S. Meltzer2, and Giuseppe Giaccone1 Abstract Purposes: To determine whether the deregulation of genes relevant for normal thymus development can contribute to the biology of thymic epithelial tumors (TET). Experimental Design: Using array comparative genomic hybridization, we evaluated the copy number aberrations of genes regulating thymus development. The expression of genes most commonly involved in copy number aberrations was evaluated by immunohistochemistry and correlated with patients’ outcome. Correlation between FOXC1 copy number loss and gene expression was determined in a confirmation cohort. Cell lines were used to test the role of FOXC1 in tumors. Results: Among 31 thymus development-related genes, PBX1 copy number gain and FOXC1 copy number loss were presented in 43.0% and 39.5% of the tumors, respectively. Immunohistochemistry on a series of 132 TETs, including those evaluated by comparative genomic hybridization, revealed a correlation between protein expression and copy number status only for FOXC1 but not for PBX1. Patients with FOXC1- negative tumors had a shorter time to progression and a trend for a shorter disease-related survival. The correlation between FOXC1 copy number loss and mRNA expression was confirmed in a separate cohort of 27 TETs. Ectopic FOXC1 expression attenuated anchorage-independent cell growth and cell migration in vitro. Conclusion: Our data support a tumor suppressor role of FOXC1 in TETs. -
C O N F E R E N C E 7 18 October 2017
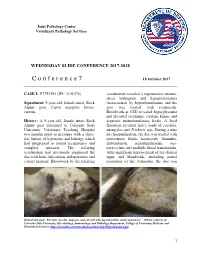
Joint Pathology Center Veterinary Pathology Services WEDNESDAY SLIDE CONFERENCE 2017-2018 C o n f e r e n c e 7 18 October 2017 CASE I: F1753191 (JPC 4101076). veterinarian revealed a regenerative anemia, stress leukogram and hypoproteinemia Signalment: 9-year-old, female intact, Rock characterized by hypoalbuminemia and the Alpine goat, Capra aegagrus hircus, goat was treated with ivermectin. caprine. Bloodwork at CSU revealed hyperglycemia and elevated creatinine, creatine kinase and History: A 9-year-old, female intact Rock aspartate aminotransferase levels. A fecal Alpine goat presented to Colorado State floatation revealed heavy loads of coccidia, University Veterinary Teaching Hospital strongyles and Trichuris spp. During a nine two months prior to necropsy with a three- day hospitalization, the doe was treated with day history of hyporexia and lethargy which intravenous fluids, kaopectate, thiamine, had progressed to lateral recumbency and fenbendazole, sulfadimethoxine, oxy- complete anorexia. The referring tetracycline and multiple blood transfusions. veterinarian had previously diagnosed the After significant improvement of her clinical doe with louse infestation, endoparasites and signs and bloodwork, including partial a heart murmur. Bloodwork by the referring resolution of the dermatitis, the doe was Haired skin goat. The skin was dry, alopecia, and covered with hyperkeratotic crusts and ulcers. (Photo courtesy of: Colorado State University, Microbiology, Immunology, and Pathology Department, College of Veterinary Medicine and Biomedical Sciences, http://csucvmbs.colostate.edu/academics/mip/Pages/default.aspx) 1 discharged. exfoliating epithelial crusts which were often tangled within scant remaining hairs. Two months later, the goat presented with a This lesion most severely affected the skin one month history of progressive scaling and over the epaxials, the ventral abdomen and ulceration over the withers, dew claws, and teats, coronary bands and dew claws. -

Cells, Tissues and Organs of the Immune System
Immune Cells and Organs Bonnie Hylander, Ph.D. Aug 29, 2014 Dept of Immunology [email protected] Immune system Purpose/function? • First line of defense= epithelial integrity= skin, mucosal surfaces • Defense against pathogens – Inside cells= kill the infected cell (Viruses) – Systemic= kill- Bacteria, Fungi, Parasites • Two phases of response – Handle the acute infection, keep it from spreading – Prevent future infections We didn’t know…. • What triggers innate immunity- • What mediates communication between innate and adaptive immunity- Bruce A. Beutler Jules A. Hoffmann Ralph M. Steinman Jules A. Hoffmann Bruce A. Beutler Ralph M. Steinman 1996 (fruit flies) 1998 (mice) 1973 Discovered receptor proteins that can Discovered dendritic recognize bacteria and other microorganisms cells “the conductors of as they enter the body, and activate the first the immune system”. line of defense in the immune system, known DC’s activate T-cells as innate immunity. The Immune System “Although the lymphoid system consists of various separate tissues and organs, it functions as a single entity. This is mainly because its principal cellular constituents, lymphocytes, are intrinsically mobile and continuously recirculate in large number between the blood and the lymph by way of the secondary lymphoid tissues… where antigens and antigen-presenting cells are selectively localized.” -Masayuki, Nat Rev Immuno. May 2004 Not all who wander are lost….. Tolkien Lord of the Rings …..some are searching Overview of the Immune System Immune System • Cells – Innate response- several cell types – Adaptive (specific) response- lymphocytes • Organs – Primary where lymphocytes develop/mature – Secondary where mature lymphocytes and antigen presenting cells interact to initiate a specific immune response • Circulatory system- blood • Lymphatic system- lymph Cells= Leukocytes= white blood cells Plasma- with anticoagulant Granulocytes Serum- after coagulation 1. -

The Future: Surgical Advances in MEN1 Therapeutic Approaches And
2410 S M Sadowski et al. Advances in surgical 24:10 T243–T260 Thematic Review management of MEN1 The future: surgical advances in MEN1 therapeutic approaches and management strategies S M Sadowski1, G Cadiot2, E Dansin3, P Goudet4 and F Triponez1 1Thoracic and Endocrine Surgery and Faculty of Medicine, University Hospitals of Geneva, Geneva, Switzerland 2Gastroenterology and Hepatology, University Hospital of Reims, Reims, France 3 Oncology, Oscar Lambret Cancer Center, University of Lille, Lille, France Correspondence 4 Endocrine Surgery, University Hospital of Dijon, and INSERM, U866, Epidemiology and Clinical Research in Digestive should be addressed Oncology Team, and INSERM, CIC1432, Clinical Epidemiology Unit, University Hospital of Dijon, Clinical Investigation to F Triponez Centre, Clinical Epidemiology/Clinical Trials Unit, Dijon, France Email [email protected] Abstract Multiple endocrine neoplasia type 1 (MEN1) is a hereditary autosomal dominant Key Words disorder associated with numerous neuroendocrine tumors (NETs). Recent advances in f multiple endocrine the management of MEN1 have led to a decrease in mortality due to excess hormones; neoplasia type 1 (MEN1) however, they have also led to an increase in mortality from malignancy, particularly f neuro-endocrine tumors (NET) NETs. The main challenges are to localize these tumors, to select those that need f thymic NET therapy because of the risk of aggressive behavior and to select the appropriate therapy f pancreatico-gastro-intestinal associated with minimal morbidity. This must be applied to a hereditary disease with a NET Endocrine-Related Cancer Endocrine-Related high risk of recurrence. The overall aim of management in MEN1 is to ensure that the f lung NET patient remains disease- and symptom-free for as long as possible and maintains a good quality of life. -

Hyperleukocytosis (Re)Visited- Is It Case Series Always Leukaemia: a Report of Two Pathology Section Cases and Review of Literature Short Communication
Review Article Clinician’s corner Original Article Images in Medicine Experimental Research Miscellaneous Letter to Editor DOI: 10.7860/JCDR/2020/40556.13409 Case Report Postgraduate Education Hyperleukocytosis (Re)Visited- Is it Case Series always Leukaemia: A Report of Two Pathology Section Cases and Review of Literature Short Communication ASHUTOSH RATH1, RICHA GUPTA2 ABSTRACT Hyperleukocytosis is defined as total leukocyte count of more than 100×109/L. Commonly seen in leukaemic conditions, non- leukaemic causes are usually not encountered and thought of. We report two such non-malignant cases of hyperleukocytosis. A six-year old girl presented with fever, cough and respiratory distress with a leukocyte count of 125.97×109/L. Another case is of a two-month old female infant, who presented with fever and respiratory distress and a leukocyte count of 112.27×109/L. The present case thrives to highlight various possible causes of hyperleukocytosis with an emphasis on non-malignant causes. Also, important complications and management of hyperleukocytosis are discussed. Keywords: Benign, Leukocytosis, Leukostasis CASE REPORT 1 for methicillin-resistant Staphylococcus aureus and was started A six-year-old girl was admitted with complaints of fever, non- on intravenous Vancomycin along with supportive care. Serial productive cough for one week and severe respiratory distress for monitoring of TLC revealed a gradual reduction and it returned to the the past one day. There was no other significant history. On physical baseline of 15×109/L after eight days. The patient was discharged examination, the patient had mild pallor. Respiratory examination after 10 days of hospital stay. -

Einstein Healthcare Network Cancer Center Active
EINSTEIN HEALTHCARE NETWORK CANCER CENTER ACTIVE CLINICAL TRIALS 1 TABLE OF CONTENTS PAGE Studies by Organ/System 3 Brain 4 - 6 Breast – Neoadjuvant/Adjuvant 6 Breast – Advanced/Metastatic 7-8 Gastrointestinal – Colorectal – Adjuvant 9 Gastrointestinal –Advanced, Metastatic 10 Gastrointestinal –Hepatocellular 11 Gastrointestinal –Pancreatic 12-13 Genitourinary – Prostate 14 Gynecological 15-16 Head and Neck 17 Myeloma 18-20 Lung – NSCLC 21-22 Lung – SCLC/Thymoma, Thymic Carcinoma/Mesothelioma 23-24 Supportive care 25 Multiple cancer diagnoses 26 Trials pending activation 27 ECOG Path. Coordinating Ctr Information “NEW” 10/24/2014 2 BRAIN PROTOCOL CONTACTS Radiation Oncology Investigator – Kenneth Zeitzer, MD 215-456-6280 Coordinator – Jeff Mealey, RN 215-456-6316 No active studies at this time. 3 BREAST PROTOCOL CONTACTS MEDICAL ONCOLOGY Investigator – Mark S. Morginstin, DO 215-456-3880 Coordinator – Joann R. Ackler, RN, OCN, CCRP 215-456-8295 RADIATION ONCOLOGY Investigator – Angelica T. Montesano, MD 215-456-6280 Coordinator – Jeff Mealy, RN 215-456-6316 STUDY# TITLE and ELIGIBILITY CRITERIA THERAPY ADJUVANT NRG BR-003/ A Randomized Phase III Trial of Adjuvant Therapy Arm 1: CIRB-005 Comparing Doxorubicin Plus Cyclophosphamide Followed by Doxorubicin 60 mg/M2 IV Weekly Paclitaxel with or without Carboplatin for Node- Cyclophosphamide 600 mg/m2 IV # Pts: _____ Positive or High-Risk Node Negative Invasive Breast Cancer Q 2 Weeks X 4 cycles Eligibility: Unilateral breast IDC: pT1-3; pN0 – pN3b, Followed by: underwent mastectomy or clear margins on lumpectomy/re- Paclitaxel 80 mg/m2 IV weekly x 12 doses excision; ER, PR, & HER2 negative (please see pgs. 14-15 of protocol for specifics). -

Periodic Fever with Aphtous Pharyngitis Adenitis (PFAPA) What
Pædiatric Rheumatology InterNational Trials Organisation Periodic fever with Aphtous Pharyngitis Adenitis (PFAPA) What is it? The patient suffers from recurrent attacks of fever and affects children in early childhood, two to four years). This disease has a chronic course, but is a benign disease with a tendency toward improvement over time. This disease was recognised for the first time in 1987 and called Marschalls’ syndrome at that time. How common is it? The frequency of PFAPA is not known, but the disease appears to be more common than generally appreciated. What are the causes of the disease? The exact cause of the disease is currently unknown. During periods of fever, the immune system is activated. This activation leads to an inflammatory response with fever and inflammation of the mouth, or throat. This inflammation is self-limited as there are no signs of inflammation to be found between two episodes. There is no infectious agent present during attacks. Is it inherited? Familial cases have been described, but no genetic cause has been found so far. Is it contagious? Infectious agents may play a role in the PFAPA syndrome, but it is not an infectious disease and is not contagious. What are the main symptoms? The main symptom is a recurrent fever, accompanied by a sore throat, mouth ulcers, or enlarged cervical lymph nodes (an important part of the immune system). The episodes of fever start abruptly and last for three to six days. During episodes, the child looks very ill and complains about at least one of the three above-mentioned symptoms. -

Practice Parameter for the Diagnosis and Management of Primary Immunodeficiency
Practice parameter Practice parameter for the diagnosis and management of primary immunodeficiency Francisco A. Bonilla, MD, PhD, David A. Khan, MD, Zuhair K. Ballas, MD, Javier Chinen, MD, PhD, Michael M. Frank, MD, Joyce T. Hsu, MD, Michael Keller, MD, Lisa J. Kobrynski, MD, Hirsh D. Komarow, MD, Bruce Mazer, MD, Robert P. Nelson, Jr, MD, Jordan S. Orange, MD, PhD, John M. Routes, MD, William T. Shearer, MD, PhD, Ricardo U. Sorensen, MD, James W. Verbsky, MD, PhD, David I. Bernstein, MD, Joann Blessing-Moore, MD, David Lang, MD, Richard A. Nicklas, MD, John Oppenheimer, MD, Jay M. Portnoy, MD, Christopher R. Randolph, MD, Diane Schuller, MD, Sheldon L. Spector, MD, Stephen Tilles, MD, Dana Wallace, MD Chief Editor: Francisco A. Bonilla, MD, PhD Co-Editor: David A. Khan, MD Members of the Joint Task Force on Practice Parameters: David I. Bernstein, MD, Joann Blessing-Moore, MD, David Khan, MD, David Lang, MD, Richard A. Nicklas, MD, John Oppenheimer, MD, Jay M. Portnoy, MD, Christopher R. Randolph, MD, Diane Schuller, MD, Sheldon L. Spector, MD, Stephen Tilles, MD, Dana Wallace, MD Primary Immunodeficiency Workgroup: Chairman: Francisco A. Bonilla, MD, PhD Members: Zuhair K. Ballas, MD, Javier Chinen, MD, PhD, Michael M. Frank, MD, Joyce T. Hsu, MD, Michael Keller, MD, Lisa J. Kobrynski, MD, Hirsh D. Komarow, MD, Bruce Mazer, MD, Robert P. Nelson, Jr, MD, Jordan S. Orange, MD, PhD, John M. Routes, MD, William T. Shearer, MD, PhD, Ricardo U. Sorensen, MD, James W. Verbsky, MD, PhD GlaxoSmithKline, Merck, and Aerocrine; has received payment for lectures from Genentech/ These parameters were developed by the Joint Task Force on Practice Parameters, representing Novartis, GlaxoSmithKline, and Merck; and has received research support from Genentech/ the American Academy of Allergy, Asthma & Immunology; the American College of Novartis and Merck.