City Leadership for Health
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Information for Persons Who Wish to Seek Asylum in the Russian Federation
INFORMATION FOR PERSONS WHO WISH TO SEEK ASYLUM IN THE RUSSIAN FEDERATION “Everyone has the right to seek and to enjoy in the other countries asylum from persecution”. Article 14 Universal Declaration of Human Rights I. Who is a refugee? According to Article 1 of the Federal Law “On Refugees”, a refugee is: “a person who, owing to well‑founded fear of being persecuted for reasons of race, religion, nationality, membership of particular social group or politi‑ cal opinion, is outside the country of his nationality and is unable or, owing to such fear, is unwilling to avail himself of the protection of that country”. If you consider yourself a refugee, you should apply for Refugee Status in the Russian Federation and obtain protection from the state. If you consider that you may not meet the refugee definition or you have already been rejected for refugee status, but, nevertheless you can not re‑ turn to your country of origin for humanitarian reasons, you have the right to submit an application for Temporary Asylum status, in accordance to the Article 12 of the Federal Law “On refugees”. Humanitarian reasons may con‑ stitute the following: being subjected to tortures, arbitrary deprivation of life and freedom, and access to emergency medical assistance in case of danger‑ ous disease / illness. II. Who is responsible for determining Refugee status? The responsibility for determining refugee status and providing le‑ gal protection as well as protection against forced return to the country of origin lies with the host state. Refugee status determination in the Russian Federation is conducted by the Federal Migration Service (FMS of Russia) through its territorial branches. -
Foreign Relations
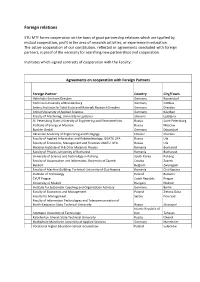
Foreign relations STU MTF forms cooperation on the basis of good partnership relations which are typified by mutual cooperation, profit in the area of research activities, or experience in education. The active cooperation of our constitution, reflected in agreements concluded with foreign partners, is proof of the necessity for searching new partnerships and cooperation. Institutes which signed contracts of cooperation with the Faculty: Agreements on cooperation with Foreign Partners Foreign Partner Country City/Town Helmholtz-Zentrum Dresden Germany Rossendorf Technical University of Brandenburg Germany Cottbus Leibniz-Institute for Solid State and Materials Research Dresden Germany Dresden Anhlat University of Applied Sciences Germany Koethen Faculty of Machining, University in Ljubljana Slovenia Ljubljana St. Petersburg State University of Engineering and Electrotechnics Russia Saint-Petersburg Institute of Energy in Moscow Russia Moscow Buehler GmbH Germany Düsseldorf Ukrainian Academy of Engineering and Pedagogy Ukraine Charkov Faculty of Applied Informatics and Robotechnology, UGATU UFA Russia Ufa Faculty of Economics, Management and Finances UGATU UFA Russia Ufa National Institute of R & D for Materials Physics Romania Bucharest Faculty of Physics, University of Bucharest Romania Bucharest University of Science and Technology in Pohang South Korea Pohang Faculty of Organisation and Informatics, University of Zagreb Croatia Zagreb Bekaert Belgium Zwevegem Faculty of Machine Building, Technical University of Cluj-Napoca Romania Cluj-Napoca -

The Situation of Minority Children in Russia
The Situation of Children Belonging to Vulnerable Groups in Russia Alternative Report March 2013 Anti- Discrimination Centre “MEMORIAL” The NGO, Anti-Discrimination Centre “MEMORIAL”, was registered in 2007 and continued work on a number of human rights and anti-discrimination projects previously coordinated by the Charitable Educational Human Rights NGO “MEMORIAL” of St. Petersburg. ADC “Memorial‟s mission is to defend the rights of individuals subject to or at risk of discrimination by providing a proactive response to human rights violations, including legal assistance, human rights education, research, and publications. ADC Memorial‟s strategic goals are the total eradication of discrimination at state level; the adoption of anti- discrimination legislation in Russia; overcoming all forms of racism and nationalism; Human Rights education; and building tolerance among the Russian people. ADC Memorial‟s vision is the recognition of non-discrimination as a precondition for the realization of all the rights of each person. Tel: +7 (812) 317-89-30 E-mail: [email protected] Contributors The report has been prepared by Anti-discrimination Center “Memorial” with editorial direction of Stephania Kulaeva and Olga Abramenko. Anti-discrimination Center “Memorial” would like to thank Simon Papuashvili of International Partnership for Human Rights for his assistance in putting this report together and Ksenia Orlova of ADC “Memorial” for allowing us to use the picture for the cover page. Page 2 of 47 Contents Executive Summary ........................................................................................................................ 4 Summary of Recommendations ..................................................................................................... 7 Overview of the legal and policy initiatives implemented in the reporting period ................. 11 Violations of the rights of children involving law enforcement agencies ............................... -

Baptist Union Council Meets in Moscow
Occasional Papers on Religion in Eastern Europe Volume 28 Issue 3 Article 3 8-2008 Baptist Union Council Meets in Moscow William Yoder Department for External Church Relations of the Russian Union of Evangelical Christian-Baptists, Moscow, Russia Follow this and additional works at: https://digitalcommons.georgefox.edu/ree Part of the Christianity Commons, and the Eastern European Studies Commons Recommended Citation Yoder, William (2008) "Baptist Union Council Meets in Moscow," Occasional Papers on Religion in Eastern Europe: Vol. 28 : Iss. 3 , Article 3. Available at: https://digitalcommons.georgefox.edu/ree/vol28/iss3/3 This Article, Exploration, or Report is brought to you for free and open access by Digital Commons @ George Fox University. It has been accepted for inclusion in Occasional Papers on Religion in Eastern Europe by an authorized editor of Digital Commons @ George Fox University. For more information, please contact [email protected]. BAPTIST UNION COUNCIL MEETS IN MOSCOW William Yoder Dr. William Yoder, with extensive experience in Germany as journalist, as well as in Poland and more recently in Russia, is now contributing a weekly news release in English and German for the Department for External Church Relations of the Russian Union of Evangelical Christian-Baptists, Moscow, Russia. Yoder is known to REE readers through numerous articles and his longtime role on the Editorial Advisory Board. The following is a composite of four news releases (appearing between October 22, 2007 and June 2008), with some editing. Despite setbacks, things are moving forward. That was the verdict following sessions of the Russian Union of Evangelical Christians-Baptists (RUECB) Council in Moscow on 20 and 21 March [2008]. -
Russian NGO Shadow Report on the Observance of the Convention
Russian NGO Shadow Report on the Observance of the Convention against Torture and Other Cruel, Inhuman or Degrading Treatment or Punishment by the Russian Federation for the period from 2001 to 2005 Moscow, May 2006 CONTENT Introduction .......................................................................................................................................4 Summary...........................................................................................................................................5 Article 2 ..........................................................................................................................................14 Measures taken to improve the conditions in detention facilities .............................................14 Measures to improve the situation in penal institutions and protection of prisoners’ human rights ..........................................................................................................................................15 Measures taken to improve the situation in temporary isolation wards of the Russian Ministry for Internal Affairs and other custodial places ..........................................................................16 Measures taken to prevent torture and cruel and depredating treatment in work of police and other law-enforcement institutions ............................................................................................16 Measures taken to prevent cruel treatment in the armed forces ................................................17 -

Name of City
Kirklees June, 2019 A comparison between 100 cities1 Introduction The Intercultural Cities is a Council of Europe flagship programme. It seeks to explore the potential of an intercultural approach to integration in communities with culturally diverse populations. The cities participating in the programme are reviewing their governance, policies, discourse and practices from an intercultural point of view. In the past, this review has taken the form of narrative reports and city profiles – a form which was rich in content and detail. However, narrative reports alone were relatively weak as tools to monitor and communicate progress. Thus, an “Intercultural City Index” has been designed as a benchmarking tool for the cities taking part in the programme as well as for future participants. As of today 100 cities have undergone their intercultural policies analysis using the Intercultural City Index: Albufeira (Portugal), Amadora (Portugal), Arezzo (Italy), Auckland (New Zealand), Ballarat (Australia), Barcelona (Spain), Beja (Portugal), Bergen (Norway), Bilbao (Spain), Botkyrka (Sweden), Braga (Portugal), Bucharest (Romania), Campi Bisenzio (Italy), Cartagena (Spain), Casalecchio di Reno (Italy), Cascais (Portugal), Castellón (Spain), Castelvetro (Italy), Catalonia (Spain), Coimbra (Portugal), Comune di Ravenna (Italy), Constanta (Romania), Copenhagen (Denmark), Donostia-San Sebastian2 (Spain), Dortmund (Germany), Dublin (Ireland), Dudelange (Luxembourg), Duisburg (Germany), Erlangen (Germany), Forlì (Italy), Fucecchio (Italy), Fuenlabrada -

IZHEVSK ELECTROMECHANICAL PLANT) ━━ Two-Component Solutions for Peritoneal Dialysis
INVESTMENT AUDIT OF THE UDMURT REPUBLIC. VERSION 1.0 UDMURTIA ON THE MAP OF RUSSIA 1 Moscow MADE IN UDMURTIA Kirov 42,100 SQ KM Perm Nizhny Novgorod Area Izhevsk (56th/85*) Kazan Yekaterinburg Ufa Samara 1.5M Population (30th/85*) UDMURTIA’S LARGEST CITIES RUB 556BN 970 КМ GRP IZHEVSK 650,000 Distance from Izhevsk (33rd/85*) to Moscow: SARAPUL 98,000 2 hours VOTKINSK 98,000 18 hours — 1200 km GLAZOV 93,000 RUB 356,043 GRP per capita (42nd/85) KEY TRANSPORT INFRASTRUCTURE: Trans-Siberian Railway (Balezino Station, Glazov Station) The P320 Elabuga-Izhevsk regional highway, connection to M7 Volga. Udmurt Republic * ranking among Russian regions Volga Federal District (VFD) IGOR SHUVALOV MAKSIM ORESHKIN DENIS MANTUROV DMITRY PATRUSHEV 3 Chairman of VEB.RF Minister of Economic Development Minister of Industry and Trade Minister of Agriculture THE REGIONAL ADMINISTRATION HAS INITIATED AN INVESTMENT AUDIT TO SUPPORT UDMURTIA’S LONG-TERM ECONOMIC DEVELOPMENT MADE IN UDMURTIA 2014 2017 2019 2020 “VEB.RF, the Russian Export “Udmurtia’s focus on driving non- “Udmurtia is a region with “Udmurtia’s climate and Centre, DOM.RF and the SME resource-based exports, training enormous investment potential environment provide an excellent Investment strategy Map of investment Investment audit Udmurt Republic’s 2027 opportunities Social and Economic Corporation are providing people entrepreneurs and promoting and ambitious goals to develop foundation for the further Udmurtia’s 2025 The investment audit of Strategy of Udmurtia with essential support entrepreneurship, enhancing the manufacturing sector. There development of the agribusiness, Investment Strategy In 2017, Udmurtia the Udmurt Republic will tools to attract investors, open productivity and adopting best is intense demand for investment food, raw materials and consumer is aimed at enhancing undertook a massive highlight the following: The strategy will be based on new manufacturing sites, create practices from other regions, among companies in Udmurtia goods sectors. -
Use Style: Paper Title
2017 15th International Conference on Emerging eLearning Technologies and Applications (ICETA 2017) Stary Smokovec, Slovakia 26-27 October 2017 IEEE Catalog Number: CFP1738M-POD ISBN: 978-1-5386-3297-0 Copyright © 2017 by the Institute of Electrical and Electronics Engineers, Inc. All Rights Reserved Copyright and Reprint Permissions: Abstracting is permitted with credit to the source. Libraries are permitted to photocopy beyond the limit of U.S. copyright law for private use of patrons those articles in this volume that carry a code at the bottom of the first page, provided the per-copy fee indicated in the code is paid through Copyright Clearance Center, 222 Rosewood Drive, Danvers, MA 01923. For other copying, reprint or republication permission, write to IEEE Copyrights Manager, IEEE Service Center, 445 Hoes Lane, Piscataway, NJ 08854. All rights reserved. *** This is a print representation of what appears in the IEEE Digital Library. Some format issues inherent in the e-media version may also appear in this print version. IEEE Catalog Number: CFP1738M-POD ISBN (Print-On-Demand): 978-1-5386-3297-0 ISBN (Online): 978-1-5386-3296-3 Additional Copies of This Publication Are Available From: Curran Associates, Inc 57 Morehouse Lane Red Hook, NY 12571 USA Phone: (845) 758-0400 Fax: (845) 758-2633 E-mail: [email protected] Web: www.proceedings.com TABLE OF CONTENTS Committees ...................................................................................................................... 3 Table of Contents ............................................................................................................ 7 Survey of Intelligent Collaborative E-Learning Systems .............................................. 17 A. Asselman*, A.-E. Nasseh*, S. Aammou* * LIROSA, Faculty of Sciences, Abdelmalek Essaadi University, Tetwan, Morocco Mobile Technologies Education based on Smart Laboratory Models ........................ -

Dear Colleagues, Udmurt State University (Russia) Invites Proposals for Papers in the Journal “Multilingualism and Education,” Issue X
Dear colleagues, Udmurt State University (Russia) invites proposals for papers in the journal “Multilingualism and Education,” issue X. The journal is included into the Russian Index of Scientific Citation (RISC) and is available on-line in eLIBRARY.ru: https://elibrary.ru/contents.asp?titleid=64145. It is also available in one of the leading e- libraries of Russia “CyberLeninka”: https://cyberleninka.ru/journal/n/mnogoyazychie-v- obrazovatelnom-prostranstveand and in Academic Resource Index “ResearchBible”: http://journalseeker.researchbib.com/view/issn/2500-3267. You can also find it at the scientific library of Udmurt State University: http://elibrary.udsu.ru/xmlui/handle/123456789/16051. The web site of the journal: http://mnogoyaz-eng.ucoz.net/. We constantly improve the quality of published materials and place the journal in other data bases, including foreign ones. Papers may be submitted in Russian, English, German, French and Spanish. All the papers will be peer-reviewed. The reviewers are prominent scholars from the universities of Russia (located in the cities of Ufa, Perm, Kazan, Izhevsk) as well as from Moldova, Sweden, Spain and the USA. The papers will be accepted for publication after getting a positive review. The main criteria are: correspondence to the suggested topics, relevance, and novelty of the results described, authenticity, structural adequacy, logical and precise wording. The papers of Master degree students should be submitted with their scientific supervisor as a co-author. The publication is free! Suggested topics include: 1. Multilingualism in education: Russian and international experience. 2. Psycholinguistic aspects of multilingualism. 3. Multilingual personality development: problems and solutions. 4. -

31 December 2017
YEAR-END REPORT 1 JANUARY – 31 DECEMBER 2017 “Continued growth” 1 OCTOBER – 31 DECEMBER 2017 (3 MONTHS) Net sales rose by 9 percent to SEK 668 million (611), which is acquired growth. EBITA rose by 4 percent to SEK 79 million (76), corresponding to an EBITA-margin of 11.7 percent (12.4). Profit after tax amounted to SEK 40 million (49). Cash flow from operating activities amounted to SEK 97 million (96). 1 JANUARY – 31 DECEMBER 2017 (12 MONTHS) Net sales rose by 20 percent to SEK 2,333 million (1,938), of which organic growth totalled 5 percent and acquired growth totalled 14 percent. EBITA rose by 24 percent to SEK 234 million (189), corresponding to an EBITA-margin of 10.0 percent (9.7). Profit after tax rose by 8 percent and amounted to SEK 120 million (112). Earnings per share amounted to SEK 4.95 (4.87). Cash flow from operating activities amounted to SEK 208 million (133). The equity ratio amounted to 40 percent (45). Return on working capital (P/WC) amounted to 63 percent (62). Three acquisitions have been carried out during the financial year, TM Techno Medica AB, Hepro AS and Krabat AS, with a combined annual sale of about SEK 225 million. The Board of Directors proposes a dividend of SEK 2.20 per share. 3 months ending 12 months ending SEKm 31 Dec 17 31 Dec 16 change 31 Dec 17 31 Dec 16 change Net sales 668 611 9 % 2,333 1,938 20 % EBITA 79 76 4 % 234 189 24 % EBITA-margin, % 11.7 12.4 10.0 9.7 Profit before tax 57 61 -7 % 158 142 11 % Profit for the period 40 49 -18 % 120 112 8 % Earnings per share SEK 1.67 2.01 -17 % 4.95 4.87 2 % Earnings per share after dilution, SEK 1.67 2.01 -17 % 4.94 4.87 1 % AddLife in brief AddLife is an independent provider in Life Science that offers high-quality products, services and advice to both the private and public sector, mainly in the Nordic region. -

National Healthy Cities Networks in the WHO European Region 3 1
NaƟ onal healthy ciƟ es networks in the WHO European Region PromoƟ ng health and well-being throughout Europe Edited by Leah Janss Lafond, consultant, United Kingdom Abstract National healthy cities networks form the backbone of the healthy cities movement in Europe. National networks overcome barriers to the local implementation of WHO-inspired and national policy frameworks by providing technical and strategic support to their city members with the direct engagement of local politicians. Every national network has developed according to the unique needs of its member cities and its available resources and according to its cultural and legal framework. This book has two parts: the analysis of the multifaceted work and achievements of 20 WHO-accredited national networks and a profile of each of these networks focusing on its organization, special features and achievements. Keywords URBAN HEALTH HEALTHY CITIES COMMUNITY NETWORKS SUSTAINABILITY EUROPE ISBN: 978 92 890 5102 6 Address requests about publica ons of the WHO Regional Offi ce for Europe to: Publica ons WHO Regional Offi ce for Europe UN City Marmorvej 51 DK-2100 Copenhagen Ø, Denmark Alterna vely, complete an online request form for documenta on, health informa on, or for permission to quote or translate, on the Regional Offi ce web site (h p://www. euro.who.int/pubrequest). © World Health OrganizaƟ on 2015 All rights reserved. The Regional Offi ce for Europe of the World Health Organiza on welcomes requests for permission to reproduce or translate its publica ons, in part or in full. The designa ons employed and the presenta on of the material in this publica on do not imply the expression of any opinion whatsoever on the part of the World Health Organiza on concerning the legal status of any country, territory, city or area or of its authori es, or concerning the delimita on of its fron ers or boundaries. -

Bhc Baseline Study
Building Healthy Communities The Baseline Study October 2008 2 Contents I. Health and Quality of Life: A State of the Art …………… p. 1 II. The Partner Cities ………………………………………… p. 13 Amaroussion ……………………………………………… p. 16 Bac ău ……………………………………………………… p. 33 Baia Mare …………………………………………………. p. 50 Barnsley …………………………………………………… p. 65 Belfast ……………………………………………………... p. 74 Lecce ………………………………………………………. p. 86 Lidingö …………………………………………………….. p. 95 Łodz ……………………………………………………….. p. 106 Madrid ……………………………………………………... p. 113 Torino ……………………………………………………… p. 132 III. Health and Quality of Life in EU Cities: A Synthesis ……… p. 149 This report has been elaborated by Marco SANTANGELO – BHC Lead Expert I I. Health and Quality of Life: A State of the Art In Europe On the European stage the EU, and especially the European Commission through the DG SANCO, is active in health promotion and linking issues of the environment and health policies together. “We need to ensure that health is at the very heart of policy making at regional, national and EU level. We need to promote health through all policies. Policy measures as different as inner city development, regional transport infrastructure, applied research, air pollution, or international trade must take health into account. Health needs to be integrated into all policies, from agriculture to environment, from transport to trade, from research to humanitarian aid and development .” (Byrne, 2004 1) Improving quality of life and good health is the EU major goal, and it is achievable by approaching it from a broad perspective. While acknowledging the role of Member States in this policy area, the EU do not proposes legislation at European level, just raises awareness of the issue. Under the EU Treaty (Treaty of Amsterdam, 1997), actions must aim to improve public health, prevent human illness and diseases and identify sources of danger to human health.