Glial Cells Are Involved in Itch Processing
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Schwann Cells (Cell Culture/Laminin) SETH PORTER*T, Luis GLASER*T, and RICHARD P
Proc. Natl. Acad. Sci. USA Vol. 84, pp. 7768-7772, November 1987 Neurobiology Release of autocrine growth factor by primary and immortalized Schwann cells (cell culture/laminin) SETH PORTER*t, Luis GLASER*t, AND RICHARD P. BUNGEt Departments of *Biological Chemistry and tAnatomy and Neurobiology, Washington University School of Medicine, St. Louis, MO 63110; and tDepartments of Biology and Biochemistry, University of Miami, Coral Gables, FL 33156 Communicated by Gerald D. Fischbach, July 20, 1987 ABSTRACT Schwann cells derived from neonatal rat proliferation. Because Schwann cells secrete laminin and sciatic nerve are quiescent in culture unless treated with specific form a basement membrane at an initial stage of neuronal mitogens. The use of glial growth factor (GGF) and forskolin ensheathment (21), it is important to establish the role of has been found to be an effective method for stimulating these components in the control of proliferation and differ- proliferation of Schwann cells on a poly(L-lysine) substratum entiation. while maintaining their ability to myelinate axons in vitro. We We report that repetitive passaging of Schwann cells find that repetitive passaging of Schwann cells with GGF and derived from neonatal rat can result in a population of forskolin results in the loss of normal growth control; the cells immortalized cells that, depending upon their duration in are able to proliferate without added mitogens. The immor- culture, display all or most ofthe functional characteristics of talized cells grow continuously in the absence of added growth a primary Schwann cell. It was found that both immortalized factor and in the presence or absence of serum yet continue to and primary Schwann cells secrete growth-promoting activ- express distinctive Schwann cell-surface antigens. -

Clustering of Na+ Channels and Node of Ranvier Formation in Remyelinating Axons
The Journal of Neuroscience, January 1995, 15(l): 492503 Clustering of Na+ Channels and Node of Ranvier Formation in Remyelinating Axons Sanja Dugandgija-NovakoviC,’ Adam G. Koszowski,2 S. Rock Levinson,2 and Peter Shragerl ‘Department of Physiology, University of Rochester Medical Center, Rochester, New York 14642 and 2Department of Physiology, University of Colorado Health Sciences Center, Denver, Colorado 80262 Polyclonal antibodies were raised against a well conserved nodal regions(Black et al., 1990). The density of Na+ channels, region of the vertebrate Na+ channel and were affinity pu- in particular, is about 25 times higher at nodesof Ranvier than rified for use in immunocytochemistry. Focal demyelination at internodal sites (Shrager, 1989). There has been vigorous of rat sciatic axons was initiated by an intraneural injection debate over the mechanism of Na+ channel clustering during of lysolecithin and Na+ channel clustering was followed at myelination, particularly with respect to the role of Schwann several stages of myelin removal and repair. At 1 week post- cells, and studies have included both developing nerve and injection axons contained long, fully demyelinated regions. pathological conditions (Ellisman, 1979; Rosenbluth, 1979; Ro- Na+ channel clusters appeared only at heminodes forming senbluth and Blakemore, 1984; Le Beau et al., 1987; England the borders of these zones, and at widely spaced isolated et al., 1990, 1991; Joe and Angelides, 1992, 1993).There remain sites that may represent former nodes of Ranvier. Over the many interesting questions, particularly regarding remodeling next few days proliferating Schwann cells adhered to axons that occurs following myelin disruption. When axons are de- and began to extend processes. -

Schwann Cell Processes Guide Regeneration of Peripheral Axons
Neuron, Vol. 14, 125-132, January, 1995, Copyright © 1995 by Cell Press Schwann Cell Processes Guide Regeneration of Peripheral Axons Young-Jin Son and Wesley J. Thompson come immunoreactive (Astrow et al., 1994). There is a Center for Developmental Biology similar up-regulation of immunoreactivity in Schwann cells and Department of Zoology of the nerve following axonal degeneration. University of Texas Motor axons commonly reinnervate muscle fibers by Austin, Texas 78712 growing down the old endoneurial Schwann cell tubes leading to each endplate. Some axons continue to grow beyond their endplates (Tello, 1907; Ramon y Cajal, 1928; Summary Gutmann and Young, 1944; Letinsky et al., 1976; Gorio et al., 1983), forming so-called "escaped" fibers. In some Terminal Schwann cells overlying the neuromuscular cases these escaped fibers grow to reinnervate nearby junction sprout elaborate processes upon muscle de- endplates. Muscle fibers reinnervated by an escaped fiber nervation. We show here that motor axons use these from an adjacent endplate as well as by an axon regenerat- processes as guides/substrates during regeneration; ing down the old Schwann cell tube become polyneuro- in so doing, they escape the confines of endplates and nally innervated (Rich and Lichtman, 1989). We wondered grow between endplates to generate polyneuronal in- whether the processes extended by terminal Schwann nervation. We also show that Schwann cells in the cells play a role in the generation of escaped fibers and nerve provide similar guidance. Axons extend from the polyneuronal reinnervation. Using immunocytochemistry, cut end of a nerve in association with Schwann cell we found that motor axons use processes of terminal processes and appear to navigate along them. -
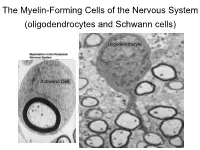
The Myelin-Forming Cells of the Nervous System (Oligodendrocytes and Schwann Cells)
The Myelin-Forming Cells of the Nervous System (oligodendrocytes and Schwann cells) Oligodendrocyte Schwann Cell Oligodendrocyte function Saltatory (jumping) nerve conduction Oligodendroglia PMD PMD Saltatory (jumping) nerve conduction Investigating the Myelinogenic Potential of Individual Oligodendrocytes In Vivo Sparse Labeling of Oligodendrocytes CNPase-GFP Variegated expression under the MBP-enhancer Cerebral Cortex Corpus Callosum Cerebral Cortex Corpus Callosum Cerebral Cortex Caudate Putamen Corpus Callosum Cerebral Cortex Caudate Putamen Corpus Callosum Corpus Callosum Cerebral Cortex Caudate Putamen Corpus Callosum Ant Commissure Corpus Callosum Cerebral Cortex Caudate Putamen Piriform Cortex Corpus Callosum Ant Commissure Characterization of Oligodendrocyte Morphology Cerebral Cortex Corpus Callosum Caudate Putamen Cerebellum Brain Stem Spinal Cord Oligodendrocytes in disease: Cerebral Palsy ! CP major cause of chronic neurological morbidity and mortality in children ! CP incidence now about 3/1000 live births compared to 1/1000 in 1980 when we started intervening for ELBW ! Of all ELBW {gestation 6 mo, Wt. 0.5kg} , 10-15% develop CP ! Prematurely born children prone to white matter injury {WMI}, principle reason for the increase in incidence of CP ! ! 12 Cerebral Palsy Spectrum of white matter injury ! ! Macro Cystic Micro Cystic Gliotic Khwaja and Volpe 2009 13 Rationale for Repair/Remyelination in Multiple Sclerosis Oligodendrocyte specification oligodendrocytes specified from the pMN after MNs - a ventral source of oligodendrocytes -
Specific Labeling of Synaptic Schwann Cells Reveals Unique Cellular And
RESEARCH ARTICLE Specific labeling of synaptic schwann cells reveals unique cellular and molecular features Ryan Castro1,2,3, Thomas Taetzsch1,2, Sydney K Vaughan1,2, Kerilyn Godbe4, John Chappell4, Robert E Settlage5, Gregorio Valdez1,2,6* 1Department of Molecular Biology, Cellular Biology, and Biochemistry, Brown University, Providence, United States; 2Center for Translational Neuroscience, Robert J. and Nancy D. Carney Institute for Brain Science and Brown Institute for Translational Science, Brown University, Providence, United States; 3Neuroscience Graduate Program, Brown University, Providence, United States; 4Fralin Biomedical Research Institute at Virginia Tech Carilion, Roanoke, United States; 5Department of Advanced Research Computing, Virginia Tech, Blacksburg, United States; 6Department of Neurology, Warren Alpert Medical School of Brown University, Providence, United States Abstract Perisynaptic Schwann cells (PSCs) are specialized, non-myelinating, synaptic glia of the neuromuscular junction (NMJ), that participate in synapse development, function, maintenance, and repair. The study of PSCs has relied on an anatomy-based approach, as the identities of cell-specific PSC molecular markers have remained elusive. This limited approach has precluded our ability to isolate and genetically manipulate PSCs in a cell specific manner. We have identified neuron-glia antigen 2 (NG2) as a unique molecular marker of S100b+ PSCs in skeletal muscle. NG2 is expressed in Schwann cells already associated with the NMJ, indicating that it is a marker of differentiated PSCs. Using a newly generated transgenic mouse in which PSCs are specifically labeled, we show that PSCs have a unique molecular signature that includes genes known to play critical roles in *For correspondence: PSCs and synapses. These findings will serve as a springboard for revealing drivers of PSC [email protected] differentiation and function. -

Advances in Transcription Factors Related to Neuroglial Cell Reprogramming
Translational Neuroscience 2020; 11: 17–27 Review Article Kuangpin Liu, Wei Ma, Chunyan Li, Junjun Li, Xingkui Zhang, Jie Liu, Wei Liu, Zheng Wu, Chenghao Zang, Yu Liang, Jianhui Guo, Liyan Li* Advances in transcription factors related to neuroglial cell reprogramming https://doi.org/10.1515/tnsci-2020-0004 glia. Neuroglial cells are intimate partners of neurons Received August 23, 2019; accepted January 7, 2020 throughout their life cycle [2]. In embryos, neuroglial cells form a cellular framework and regulate the survival Abstract: Neuroglial cells have a high level of plasticity, and differentiation of neurons. In addition, during and many types of these cells are present in the nervous neurogenesis and early development, neuroglial cells system. Neuroglial cells provide diverse therapeutic mediate the proliferation and differentiation of neurons targets for neurological diseases and injury repair. Cell by synthesizing and secreting various growth factors and reprogramming technology provides an efficient pathway extracellular matrix components [2]. The most prominent for cell transformation during neural regeneration, while function of neuroglial cells during development is transcription factor-mediated reprogramming can facilitate formation of myelin sheaths around axons, which provide the understanding of how neuroglial cells mature into necessary signals and maintain rapid conduction for functional neurons and promote neurological function nervous system function [3]. Additionally, neuroglial recovery. cells maintain homeostasis in nerve cells and participate in synaptic plasticity and cell repair [2]. Similar to Keywords: Neuroglial cell; Reprogramming; Transcription developmental processes in other types of animal cells, factor the development of neuroglial cells is influenced by interactions between cells; cell lineage and extracellular signaling can regulate the migration, proliferation and 1 Introduction differentiation of glial cells. -

Human Nerve-On-A-Chip. Engineering 3D Functional Human Peripheral Nerve in Vitro
bioRxiv preprint doi: https://doi.org/10.1101/458463; this version posted November 8, 2018. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Human Nerve-on-a-Chip. Engineering 3D functional human peripheral nerve in vitro Anup D. Sharma1,*, Laurie McCoy1, Elizabeth Jacobs1, Hannah Willey1, Jordan Q. Behn1, Hieu Ngyuen1, Brad Bolon4, J. Lowry Curley1, Michael J. Moore1,2,3,* AxoSim Inc.1, Dept. of Biomedical Engineering2, and Brain Institute3, Tulane University, New Orleans, LA. GEMpath, Inc.,4 Longmont, CO, USA *Corresponding authors Anup Dutt Sharma Research Scientist AxoSim, Inc. 1441 Canal Street, Suite 205 New Orleans BioInnovation Center New Orleans, LA 70112 Email: [email protected] Michael J. Moore Associate Professor 526 Lindy Boggs Center Department of Biomedical Engineering Tulane University New Orleans, LA 70118 Email: [email protected] bioRxiv preprint doi: https://doi.org/10.1101/458463; this version posted November 8, 2018. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Abstract Development of ”organ-on-a-chip” systems in the space of the nervous system is lagging because of lack of availability of human neuronal & glial cells and the structural complexity of the nervous system. Furthermore, a sizeable challenge in the drug development pipeline and an often-cited reason for failure in a vast number of clinical trials conducted for neuropathological ailments is the lack of translation from animal models. A preclinical in vitro model capable of mimicking the function and structure of the human nervous system is well desired. -

Neuron-Satellite Glial Cell Interactions in Sympathetic Nervous System Development
NEURON-SATELLITE GLIAL CELL INTERACTIONS IN SYMPATHETIC NERVOUS SYSTEM DEVELOPMENT by Erica D. Boehm A dissertation submitted to the Johns Hopkins University in conformity with the requirements for the degree of Doctor of Philosophy Baltimore, Maryland July 2020 © 2020 Erica Boehm All rights reserved. ABSTRACT Glial cells play crucial roles in maintaining the stability and structure of the nervous system. Satellite glial cells are a loosely defined population of glial cells that ensheathe neuronal cell bodies, dendrites, and synapses of the peripheral nervous system (Elfvin and Forsman 1978; Pannese 1981). Satellite glial cells are closely juxtaposed to peripheral neurons with only 20nm of space between their membranes (Dixon 1969). This close association suggests a tight coupling between the cells to allow for possible exchange of important nutrients, yet very little is known about satellite glial cell function and development. How neurons and glial cells co-develop to create this tightly knit unit remains undefined, as well as the functional consequences of disrupting these contacts. Satellite glial cells are derived from the same population of cells that give rise to peripheral neurons, but do not begin differentiation and proliferation until neurogenesis has been completed (Hall and Landis 1992). A key signaling pathway involved in glial specification is the Delta/Notch signaling pathway (Tsarovina et al. 2008). However, recent studies also implicate Notch signaling in the maturation of glia through non- canonical Notch ligands such as Delta/Notch-like EGF-related Receptor (DNER) (Eiraku et al. 2005). Interestingly, it has been reported that levels of DNER in sympathetic neurons may be dependent on the target-derived growth factor, nerve growth factor (NGF), and this signal is prominent in sympathetic neurons at the time in which satellite glial cells are developing (Deppmann et al. -

Schwann Cells, but Not Oligodendrocytes, Depend Strictly
RESEARCH ARTICLE Schwann cells, but not Oligodendrocytes, Depend Strictly on Dynamin 2 Function Daniel Gerber1†, Monica Ghidinelli1†, Elisa Tinelli1, Christian Somandin1, Joanne Gerber1, Jorge A Pereira1, Andrea Ommer1, Gianluca Figlia1, Michaela Miehe1, Lukas G Na¨ geli1, Vanessa Suter1, Valentina Tadini1, Pa´ ris NM Sidiropoulos1, Carsten Wessig2, Klaus V Toyka2, Ueli Suter1* 1Department of Biology, Institute of Molecular Health Sciences, Swiss Federal Institute of Technology, ETH Zurich, Zurich, Switzerland; 2Department of Neurology, University Hospital of Wu¨ rzburg, University of Wu¨ rzburg, Wu¨ rzburg, Germany Abstract Myelination requires extensive plasma membrane rearrangements, implying that molecules controlling membrane dynamics play prominent roles. The large GTPase dynamin 2 (DNM2) is a well-known regulator of membrane remodeling, membrane fission, and vesicular trafficking. Here, we genetically ablated Dnm2 in Schwann cells (SCs) and in oligodendrocytes of mice. Dnm2 deletion in developing SCs resulted in severely impaired axonal sorting and myelination onset. Induced Dnm2 deletion in adult SCs caused a rapidly-developing peripheral neuropathy with abundant demyelination. In both experimental settings, mutant SCs underwent prominent cell death, at least partially due to cytokinesis failure. Strikingly, when Dnm2 was deleted in adult SCs, non-recombined SCs still expressing DNM2 were able to remyelinate fast and efficiently, accompanied by neuropathy remission. These findings reveal a remarkable self-healing capability of peripheral nerves that are affected by SC loss. In the central nervous system, however, *For correspondence: we found no major defects upon Dnm2 deletion in oligodendrocytes. [email protected] DOI: https://doi.org/10.7554/eLife.42404.001 †These authors contributed equally to this work Competing interests: The Introduction authors declare that no Motor, sensory, and cognitive functions of the nervous system require rapid and refined impulse competing interests exist. -
Mechanisms of Node of Ranvier Assembly
REVIEWS Mechanisms of node of Ranvier assembly Matthew N. Rasband 1 ✉ and Elior Peles 2 ✉ Abstract | The nodes of Ranvier have clustered Na+ and K+ channels necessary for rapid and efficient axonal action potential conduction. However, detailed mechanisms of channel clustering have only recently been identified: they include two independent axon–glia interactions that converge on distinct axonal cytoskeletons. Here, we discuss how glial cell adhesion molecules and the extracellular matrix molecules that bind them assemble combinations of ankyrins, spectrins and other cytoskeletal scaffolding proteins, which cluster ion channels. We present a detailed molecular model, incorporating these overlapping mechanisms, to explain how the nodes of Ranvier are assembled in both the peripheral and central nervous systems. Axolemma In the early 1800s, engineers dreamed of communication mechanisms for their assembly have been revealed. In The plasma membrane of between North America and Europe using a transatlan- this Review, we emphasize and discuss nodal proteins the axon. tic telegraph cable. Their vision was realized in 1858 in the context of the multiple overlapping axon–glia and introduced a new ‘Age of Information'1. Although interactions that combine and converge on the axonal Extracellular matrix (ECM). A complex mixture of this earliest cable only transmitted a few words per cytoskeleton to efficiently cluster and maintain high + + extracellular macromolecules, hour, it still reduced the time required for the transmis- densities of Na and K channels at the nodes of Ranvier. including glycoproteins, that sion of a message by more than tenfold. Today, mod- surround cells. ern fibre- optic cable systems have further reduced this Myelinating glia control node assembly time to just milliseconds! However, these technological Myelination is a late developmental process mediated wonders lag ~400 million years behind the revolution by Schwann cells in the peripheral nervous system in speed of axonal action potential conduction that (PNS) and oligodendrocytes in the CNS. -

Unexpected Central Role of the Androgen Receptor in the Spontaneous Regeneration of Myelin
Unexpected central role of the androgen receptor in the spontaneous regeneration of myelin Bartosz Bieleckia,b, Claudia Matternc, Abdel M. Ghoumaria, Sumaira Javaida,d, Kaja Smietankaa,b, Charly Abi Ghanema, Sakina Mhaouty-Kodjae, M. Said Ghandourf,g, Etienne-Emile Baulieua,1, Robin J. M. Franklinh,i, Michael Schumachera,1,2, and Elisabeth Traifforta,2 aU1195 INSERM, University Paris-Sud, University Paris-Saclay, Kremlin-Bicêtre 94276, France; bDepartment of Neurology and Stroke, Medical University of Lodz, Lodz 90-549, Poland; cMattern Foundation, Vaduz 9490, Liechtenstein; dHussain Ebrahim Jamal Research Institute of Chemistry, International Center for Chemical and Biological Sciences, University of Karachi, Karachi 75270, Pakistan; eU1130 INSERM, UMR 8246 CNRS, University Pierre and Marie Curie, Paris 75005, France; fUMR 7357 CNRS, University of Strasbourg, Strasbourg 67000, France; gDepartment of Anatomy and Neurobiology, Virginia Commonwealth University, Richmond 23284, VA; hWellcome Trust-Medical Research Council Cambridge Stem Cell Institute, University of Cambridge, Cambridge CB2 0AH, United Kingdom; and iDepartment of Clinical Neurosciences, University of Cambridge, Cambridge CB2 0AH, United Kingdom Contributed by Etienne-Emile Baulieu, September 9, 2016 (sent for review June 23, 2016; reviewed by Pamela E. Knapp and Bruce S. McEwen) Lost myelin can be replaced after injury or during demyelinating remyelination was prevented by X-irradiation (4, 6, 7). Unequivocal diseases in a regenerative process called remyelination. In the central confirmation that most Schwann cells contributing to CNS remyeli- nervous system (CNS), the myelin sheaths, which protect axons and nation are indeed derived from OPs has been provided by genetic allow the fast propagation of electrical impulses, are produced by fate-mapping in transgenic mice (5). -

Ultrastructural Anatomy of Nodes of Ranvier in the Peripheral Nervous
Ultrastructural anatomy of nodes of Ranvier in the PNAS PLUS peripheral nervous system as revealed by STED microscopy Elisa D’Estea,1, Dirk Kamina, Francisco Balzarottia, and Stefan W. Hella,1 aDepartment of NanoBiophotonics, Max Planck Institute for Biophysical Chemistry, 37077 Goettingen, Germany Contributed by Stefan W. Hell, November 28, 2016 (sent for review August 9, 2016; reviewed by Frank Bradke and Hjalmar Brismar) We used stimulated emission depletion (STED) superresolution also in oligodendrocyte precursors (5) and in Schwann cells (6). microscopy to analyze the nanoscale organization of 12 glial and During axon ensheathment, cytoskeletal rearrangements—and axonal proteins at the nodes of Ranvier of teased sciatic nerve fibers. actin disassembly in particular—constitute a fundamental process Cytoskeletal proteins of the axon (betaIV spectrin, ankyrin G) exhibit (10, 11). Altogether, these observations raise questions as to the a high degree of one-dimensional longitudinal order at nodal gaps. In relation and the possible reciprocal influence between the axonal contrast, axonal and glial nodal adhesion molecules [neurofascin-186, and glial cytoskeletal lattices, especially at paranodes, which are neuron glial-related cell adhesion molecule (NrCAM)] can arrange in a the regions flanking the nodal gaps. There, the myelin loops more complex, 2D hexagonal-like lattice but still feature a ∼190-nm contact the axon to form the paranodal junctions (PNJs), and the periodicity. Such a lattice-like organization is also found for glial ac- axon–glia interaction is extremely tight (12, 13). This interaction is tin. Sodium and potassium channels exhibit a one-dimensional peri- also important for the recruitment of Nav channels at nodal gaps odicity, with the Nav channels appearing to have a lower degree of the PNS, as this process is orchestrated by proteins present on of organization.